PHYSIOLOGY: KIDNEY AND SODIUM ADH BRAIN CELL VOLUME REGULATION HYPONATRAEMIA: PATHOPHYSIOLOGY...
30
SODIUM AND THE BRAI N
-
Upload
alberta-turner -
Category
Documents
-
view
216 -
download
0
Transcript of PHYSIOLOGY: KIDNEY AND SODIUM ADH BRAIN CELL VOLUME REGULATION HYPONATRAEMIA: PATHOPHYSIOLOGY...

SODIUM AND THE
BRAIN

OUTLINE PHYSIOLOGY: KIDNEY AND SODIUM
ADH BRAIN CELL VOLUME REGULATION
HYPONATRAEMIA: PATHOPHYSIOLOGY
ENCEPHALOPATHY MANAGEMENT
OSMOTIC DEMYELINATION SYNDROME
HYPERNATRAEMIA: PATHOPHYSIOLOGY ENCEPHALOPATHY MANAGEMENT

PHYSIOLOGY – KIDNEYS

PHYSIOLOGY – KIDNEYS Sodium:
- content: 3% intracellular; 40% in bone; remainder interstitial and intravascular- intake: readily absorbed through GIT; presence of glucose enhances sodium absorption due to co-transporter; intake recommended not to exceed 2500mg/d- excretion: stool minimal unless diarrhoea sweat normally 5-40mmol/l (cystic fibrosis, aldosterone deficiency, pseudohypoaldosteronism) kidneys principal site

PHYSIOLOGY – KIDNEYS Sodium concentration determined by water balance, not
sodium balance; renal excretion of sodium therefore not regulated by plasma osmolality
Proximal tubule: 60% reabsorbed; Na-H exchangeThick ascending loop: 30%; Na-2Cl-K cotransporterDistal tubule: 7%; Na-Cl cotransporterCollecting ducts: 3%; ENaC channels aldosterone
Factors affecting sodium excretion- changes in GFR- changes in tubular reabsorption, esp at collecting ducts (aldosterone and other adrenocortical
hormones, natriuretic hormones, rate of tubular secretion of H and K

PHYSIOLOGY – ADH Arginine vasopressin: peptide hormone which is most
important regulator of water excretion, also vasoconstrictor
Stimuli:
Mechanism: hypothalamus
posterior pituitary
V2 receptor on basolateral aspect collecting duct cells
aquaporin2 insertion on luminal membrane
Plasma osmolarity:
Osmoreceptors anterior
hypothalamus
Blood volume:Low pressure receptors in
great veins, atria, pulmonary
vessels
Blood pressure:Carotid and
aortic baroreceptors

PHYSIOLOGY – ADH


PHYSIOLOGY – BRAIN MECHANISMS Brain particularly vulnerable to changes in
body fluid osmolality- oedema with hypo-osmolar states- dehydration with cell shrinkage in hyperosmolar states
Brain adapts to osmotic stresses through many mechanisms - transient changes in water content- sustained changes in electrolyte and organic osmolyte contents
*Ref: Review in 2010 Neuroscience issue by JG Verbalis “Brain volume regulation in response to changes in osmolality”

PHYSIOLOGY – BRAIN MECHANISMS Hypo-osmolality/hyponatremia:
- water into intracellular compartment oedema - brain adapts by losing solute, thus decreasing cellular water
content. Movement by diffusion, not energy-dependent carriers. solutes (a) electrolytes (K, Cl)
(b) organic osmolytes (amino acids [glycine, GABA, glutamate, aspartate], polyalcohols, sugars, methylamines)- rate of fall of sodium correlates with morbidity and mortality
acute greater volume of water accumulates before brain loses enough solute to compensate
(acute=24-48hrs)chronic almost complete normalization of water content in hyponatremia maintained over 21 days
- Deadaptation: takes longer for brain to re-accumulate its solutes – risk of cellular dehydration with rapid correction

PHYSIOLOGY – BRAIN MECHANISMS Hyperosmolality/hypernatremia:
- osmotic shifts of intracellular water into extracelullar compartment cellular dehydration- brain cells adapt by accumulating solutes; rapid accumulation of electrolytes, more gradual accumulation of organic osmolytes, AKA idiogenic osmoles- Mechanisms of brain organic osmolyte accumulation remain poorly understood, but likely combination of uptake and synthesis- acute developing in 24-48hours; less likely; accidental salt poisoning, severe diarrhoea
45% morbidity and mortality in children: rapid accumulation of electrolytes
- chronic developing over several days; generally better tolerated with less neurological symptoms than acute;
gradual accumulation of organic solutes beginning after 9-24hrs, steady state at 2-7 days- Neurological symptoms and mortality higher in acute rather than chronic hypernatremia

PHYSIOLOGY – BRAIN MECHANISMS
Fig. 4. Relative increases in individual brain electrolytes and organicosmolytes during adaptation to chronic hypernatremia in rats. Thecategory “other” represents GPC, urea, and several other amino acids.Reproduced with permission from (Gullans and Verbalis, 1993).

HYPONATREMIA – PATHOPHYSIOLOGY
Most common electrolyte disturbance in children More serious than previously believed Primary defence to development of
hyponatremia: kidney excretes free water For hyponatremia to occur: excess free water
coupled with underlying renal impairment of free water excretion
Disorders:- marked decrease in GFR- renal hypoperfusion- excess of ADH

HYPONATREMIA – PATHOPHYSIOLOGY
Table 2 Disorders in impaired renal water excretion1. Effective circulating volume depletiona) Gastrointestinal losses: vomiting, diarrheab) Skin losses: cystic fibrosisc) Renal losses: salt-wasting nephropathy, diuretics, cerebral saltwasting, hypoaldosteronismd) Oedematous states: heart failure, cirrhosis, nephrosis,hypoalbuminemiae) Decreased peripheral vascular resistance: sepsis, hypothyroidism2. Thiazide diuretics3. Renal failurea) Acuteb) Chronic4. Non-hypovolemic states of antidiuretic hormone (ADH)
excessa) Syndrome of inappropriate secretion of antidiuretic hormone(SIADH)b) Nausea, emesis, pain, stressc) Post-operative stated) Cortisol deficiency5. Nephrogenic syndrome of inappropriate antidiuresis
(NSIAD)

HYPONATREMIA – PATHOPHYSIOLOGY
Cerebral Salt Wasting:- cerebral disease causes disorder in sodium and water handling- renal function usually normal- natriuresis hyponatremia and hypovolaemia- clinically: polyuria
dehydration (despite adequate intake) elevated urine sodium levels
- postulated mechanism: (a) interference with sympathetic input to kidney decrease in renin
secretion decreased aldosterone. Also dilatation of afferent arteriole increased glomerular filtration of plasma and sodium (b) circulating natriuretic factors abnormally elevated dilatation of afferent arteriole with increased filtration of water and sodium; inhibit angiotensin-induced sodium reabsorption at proximal convoluted tubule; antagonize action of ADH at collecting ducts- NB: Differentiate cerebral salt wasting (hypovolemic) from SIADH (euvolemic)

HYPONATREMIA – PATHOPHYSIOLOGY
Asymptomatic hyponatremia:- in adults with mild chronic hyponatremia with Na
mean of 128mmol/l found to have subtle neurological impairment affecting gait and attention
- preterm neonates show impaired growth and development and have increased sodium
intake as adolescents- lacking data in older children
Hyponatremia also significant risk factor for sensorineural hearing loss, CP and intracranial haemorrhage
Risk factor for increased mortality in neonates with perinatal asphyxia

HYPONATREMIA – ENCEPHALOPATHY Most serious complication of hyponatremia and is
medical emergency Primary symptoms are those of cerebral oedema
coma
EARLY ADVANCED
headache seizures
N&V coma
lethargy apnoea
weakness pulmonary oedema
confusion decorticate posturing
altered LOC dilated pupils
agitation anisocoria
gait disturbances papilloedema
cardiac arrythmia
myocardial ischemia
central diabetes insipidus

HYPONATREMIA – ENCEPHALOPATHY Progression from mild to advanced symptoms can be
abrupt with no consistent progression Common yet under-recognised feature is non-cardiogenic
pulmonary oedema called Ayus-Arieff syndrome- mechanism 1: centrally mediated increase in pulmonary vascular permeability to proteins, leading to increased alveolar and interstitial fluid- mechanism 2: increased sympathetic neuronal activity with catecholamine release, resulting in pulmonary vasoconstriction with increased capillary hydrostatic pressure and capillary wall injury
- primarily reported in patients with post-op and exercise-associated hyponatremia- rapidly reversible with hypertonic saline, and almost universally fatal if untreated.

HYPONATREMIA – ENCEPHALOPATHY Risk factors:
(1) decreased cranial capacity children>adults – average Na in children with encephalopathy is 120mmol/l, in adults 111mmol/l
– children have relatively larger brain to intracranial volume ratio (brain reaches adult size by age 6, skull only by age 16)space-occupying lesionshydrocephalus
(2) impaired brain cell volume regulation and decreased cerebral perfusionincreased ADH levelsfemale sex steroids (oestrogens reduce Na/K/ATPase pump activity, androgens enhance it)
hypoxia(3) CNS disorders
infection (meningitis, encephalitis)encephalopathy (metabolic, hepatic, ischaemic, toxic)cerebritisbrain injury and neurosurgeryseizure disorders

HYPONATREMIA – ENCEPHALOPATHY Hypoxaemia combined with hyponatremia more deleterious
than either factor alone – hypoxaemia impairs brain’s ability to adapt to hyponatremia leading to worsening encephalopathy
Patient with CNS disorder already at risk for raised ICP and have impaired brain cell volume regulation, additional water movement into brain from even mild hyponatremia can be lethal
One study in children with pneumococcal meningitis showed mortality of 100% in those with sNa <130mmol/l
In maple-syrup-urine disease, hyponatremia found to lead to progressive cerebral oedema during episodes of acute metabolic intoxication
In DKA, mild hyponatremia sNa <135mmol/l appears to play role in development of cerebral oedema
NO DEGREE OF HYPONATREMIA SHOULD BE CONSIDERED SAFE IN PATIENTS WITH CNS DISEASE

HYPONATREMIA – MANAGEMENT

HYPONATREMIA – MANAGEMENT Preventing hospital-acquired hyponatremia
- 0.9% NaCl in patients at risk for ADH excess- abandonment of routine administration of hypotonic and
near- isotonic IV fluids (Na<130) NB: 0.9%NaCl not suited to all clinical circumstances, e.g. causes hypernatraemia if used in diabetes insipidus or profuse watery diarrhoea; may not always prevent hyponatremia in CNS injury where there is cerebral salt wasting or SIADH
Management:Hypertonic saline (3%NaCl, 513mmol/l) 2ml/kg bolus over 10mins, with maximum of 100mlsingle bolus results in 2mmol/l acute rise in sNa which would quickly reduce cerebral oedemabolus can be repeated one or two times
Goal of correction 5-6mmol/l in first 1-2hr. Thereafter, various recommendations of safe limits for correction: 6-8mmol/l In 24hr, or 10mmol/l in 24hours, or 15 mmol/l in 24hrs, or 20mmol/l in 48hrs

OSMOTIC DEMYELINATION SYNDROME
Rare and acute demyelinating process commonly associated with rapid correction of hyponatremia – sNa increased by more than 12mmol/l/d
Initially described in 1959 as condition seen in alcoholic and malnourished patients
Pathophysiology:- not fully understood- linked to intramyelinitic splitting, vacuolization, and rupture of myelin sheaths presumably caused by osmotic effects- oligodendrocytes particularly sensitive to osmotic changes; distribution of changes of ODS parallel distribution of oligodendroglial cells- damage is characteristically symmetrical- J Am Soc Nephr 2011, Kengne et al: apoptosis in astrocytes followed by a loss of trophic communication between astrocytes and oligodendrocytes, secondary inflammation, microglial activation, and finally demyelination.

OSMOTIC DEMYELINATION SYNDROME
Pontine myelinolysisExtrapontine myelinolysis: basal ganglia, cerebral white matter, peripheral cortex, hippocampi, lateral geniculate bodies
Very infrequently seen in infants possibly due to ongoing myelination process which occurs under age 2yrs
- Supratentorial white matter myelination occurs later than pontine myelination; therefore, extrapontine myelinolysis is even more rare
Predisposing factors: prolonged use of diuretics, liver failure, organ transplantation, extensive burns, diabetes mellitus, metabolic disorders, uraemia, dialysis, hypoxic-ischaemic states
Clinical:- spastic quadriplegia - pseudobulbar palsy- loss of consciousness - cranial nerve palsies

OSMOTIC DEMYELINATION SYNDROME
EXTRA-PONTINE MYELINOLYSIS:T2 weighted magnetic resonance scan image showing bilaterally symmetrical hyperintensities in caudate nucleus, putamen, with sparing of globus pallidus.
CENTRAL PONTINE MYELINOLYSIS: Axial fat-saturated T2-weighted image showing hyperintensity in the pons with sparing of the peripheral fibres.
HYPERNATREMIA – PATHOPHYSIOLOGY
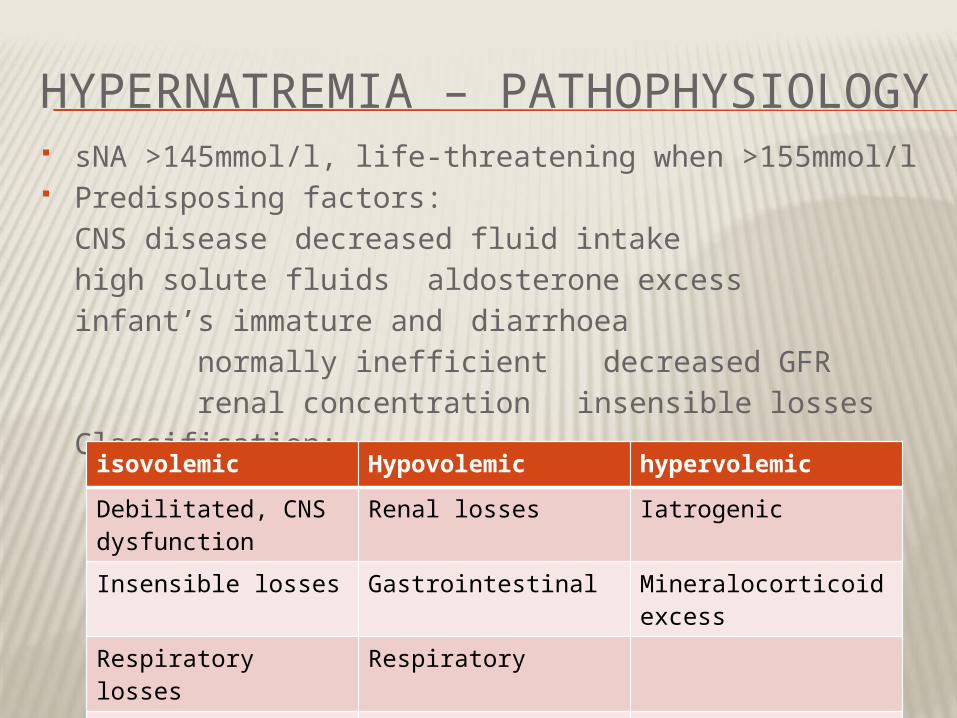
sNA >145mmol/l, life-threatening when >155mmol/l Predisposing factors:
CNS disease decreased fluid intakehigh solute fluids aldosterone excess
infant’s immature and diarrhoea normally inefficient decreased GFR renal concentration insensible losses
Classification:
isovolemic Hypovolemic hypervolemic
Debilitated, CNS dysfunction
Renal losses Iatrogenic
Insensible losses Gastrointestinal Mineralocorticoid excess
Respiratory losses Respiratory
Diabetes insipidus Skin losses (burns)

HYPERNATREMIA – CLINICAL MANIFESTATION
In hypernatremic dehydration, 2/3 water lost is intracellular with better preservation of intravascular compartment – skin turgor may be normal despite loss of 10% body weight
BP and urine output also maintained Abdominal skin has doughy feel probably due to
intracellular water loss Hypernatraemia may cause fever, although usually
from underlying process Hypernatraemia associated with hyperglycaemia
and mild hypocalcaemia – mechanism unknown

HYPERNATRAEMIA – ENCEPHALOPATHY
CNS symptoms prominent; tend to parallel degree of hypernatraemia and acuity of the increase
CNS cells attempt to increase osmolarity:- water moves out of the cells - Intracellular proteins break down to form solutes severe disruption of intracellular proteins could account for drastic and sometimes permanent impairment of brain function
Manifestations:- pronounced irritability, restlessness - convulsions- weak and lethargic - coma- muscular hypertonicity - subdural haematomas- cerebral petechiae - cerebral haemorrhage- cerebral vein thrombosis - stroke

HYPERNATREMIA – MANAGEMENT

HYPERNATREMIA – MANAGEMENT
Hypernatraemia should not be corrected rapidly due to risk of oedema with resultant seizures and coma.
Decrease at rate of not more than 12mmol/l/d or 0.5mmol/l/hr
Managing shock: 0.9%NaCl preferable over Ringers Correction: - 0.45% NaCl with fluid rate only
20-30% greater than maintenance - if hypernatraemia due to sodium
administration, can correct faster or peritoneal dialysis severe
Cerebral Oedema: 3%NaCl stop hypotonic solution