HIV / AIDS 2005 Sky R. Blue, MD Mother To Child Transmission.
95
HIV / AIDS 2005 Sky R. Blue, MD Mother To Child Transmission
-
Upload
richard-wiggins -
Category
Documents
-
view
218 -
download
0
Transcript of HIV / AIDS 2005 Sky R. Blue, MD Mother To Child Transmission.

HIV / AIDS 2005
Sky R. Blue, MD
Mother To Child Transmission


HIV - The Numbers Number of people living with HIV/AIDS
Total 40 million (34 - 46 million) Adults 37 million (31 - 43 million) Children under 15 years 2.5 million (2.1 - 2.9 million)
People newly infected with HIV in 2003 Total 5 million (4.2 - 5.8 million)
Adults 4.2 million (3.6 - 4.8 million) Children under 15 years 700 000 (590 000 - 810 000)
AIDS deaths in 2003 Total 3 million (2.5 - 3.5 million)
Adults 2.5 million (2.1 - 2.9 million) Children under 15 years 500 000 (420 000 - 580 000

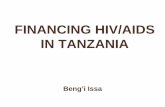
Adults and Children Living with HIV/AIDS 2003
Total: 40 millionData from UNAIDS
N. America950,000
Caribbean420,000
Latin America1.5 million
Western Europe550,000
Sub-SaharanAfrica 28.5 million
Asia & Pacific6.6 million
Australia & NewZealand 15,000
North Africa500,000
Eastern Europe1 million
44,000
53,00092,000
21,000
240,000
210,000
1,800,000
3,100,000 5,000
New Cases

Prevalence15 – 30 %5.0 - 15 %1.0 – 5.0 %0.5 – 1.0 %0.1 – 0.5 %0.0 – 0.1 %Not Available HIV Prevalence HIV Prevalence
WorldwideWorldwide

Men to Women RatiosUS
14 : 1Haiti
3 : 1Africa
1 : 1


Quarter-Year
Nu
mb
er
of
Case
s/D
eath
s
*Adjusted for reporting delays
1985198619871988198919901991199219931994199519961997199819990
5,000
10,000
15,000
20,000
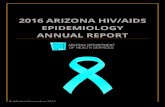
25,0001993 definitionimplementationDeaths
Prevalence
AIDS
0
150,000
100,000
50,000
200,000
250,000
300,000
350,000
Estimated Incidence of AIDS, Deaths, and Prevalence by Quarter-Year of Diagnosis/Death,
United States, 1985-1999*
Pre
vale
nce



Epidemiology
Distribution of AIDS/HIV status1
340K AIDS
130K HIV+
200K HIV+ but not in care
280K Undiagnosed
200K
400K
600K
800K
1000K 950K

HIV in Idaho – Prevalence
District 1 50 40 District 2 32 15 District 3 60 36 District 4 214 113 District 5 48 23 District 6 44 18 District 7 26 15 Total 478 260
HIV AIDS
738(As of Dec 2003)

HIV Services Clinic – Family Medicine Residency of Idaho (FMRI)
Gender Male 78% Female 22%
Ethnicity White 79% Black 5% Hispanic 14% Asian 1% Native Am 1% Other <1%

HIV Services Clinic - FMRI
0
10
20
30
40
50
60
70
<12 13-24 25-44 45-64 >65
HIV/AIDS
AGE
%

HIV and Pregnancy AIDS in women has risen from 7% of adult
cases early in the epidemic to 27% today 7,000-10,000 babies are born each year to
HIV infected mothers 2,000-3,000 would be born with HIV Universal screening and perinatal treatment
could reduce this to <500

HIV Testing in Pregnancy National Recommendations Universal voluntary testing with patient
notification as a routine component of prenatal care American Academy of Pediatrics and American
College of Obstetricians and Gynecologists. Human Immunodeficiency Virus screening: joint statement of the AAP and ACOG. Pediatrics 1999;104:128.
Institute of Medicine. Reducing the odds: preventing perinatal transmission of HIV in the United States. Washington, DC: National Academy Press, 1999

HIV Testing in Pregnancy CDC (USPHS) recommendations for HIV
screening of pregnant women Prenatal: routine HIV screening for all pregnant
women using the “opt out” approach — women will be notified that they will be tested unless they decline
Labor and delivery: routine rapid testing for women whose HIV status is unknown
Postnatal: rapid testing for all infants whose mother’s status is unknown.
MMWR November 15, 2002 Regulations, laws, & policies about HIV
screening of pregnant women vary state to state

Untreated Populations15% of women with HIV infection have
no prenatal care compared to 2% of all pregnant women (MMWR, 1998)
Risk of HIV infection at least 2- to 4-fold higher among women presenting for delivery without prenatal care
E Aaron, CRNP. Presented at Clinical Pathway, August 2002.

Missed Opportunities Women who do not receive prenatal care Pregnant women who seek prenatal care
erratically Non-legal residents Injection drug users Homeless Women who receive prenatal care but are not
offered testing
E Aaron, CRNP. Presented at Clinical Pathway, August 2002.

3rd Trimester Testing Retesting in the third trimester, preferably
before 36 weeks of gestation, is recommended for women known to be at high risk for acquiring HIV: who have a history of sexually transmitted diseases, who exchange sex for money or drugs, who have multiple sex partners during pregnancy, who use illicit drugs, who have sex partner(s) known to be HIV-positive or
at high risk who have signs and symptoms of seroconversion.
CDC. Revised US Public Health Service recommendations for human immunodeficiency virus screening of pregnant women. MMWR 2001;50(No. RR-19):59--86.

Rapid Testing at Delivery
High risk of perinatal transmission in women without antenatal care and without HIV counseling and testing
Rapid testing during labor can make it possible to initiate ART prophylaxis and to refer the woman for care
ART prophylaxis should be initiated as soon as possible after a positive rapid HIV test (before confirmatory test results are available)

HIV Antibody Tests Serum antibody (EIA) Saliva and urine antibody tests (EIA) Rapid tests
SUDS (Microfiltration EIA) Laboratory-based
OraQuick Point of care
Western blot assay Confirmatory test

Western Blot
CDC criteria 1 p160, p120 AND p41
CDC criteria 2 p160, p120 OR p41 PLUS p24
p160 p120 p41 p68 p53 p32 p55 p40 p24 p18G
AG
PO
L
EN
V

HIV Direct Tests
Viral Load Qualitative / quantitative RNA through bDNA or PCR
p24 antigen tests


HIV care During Pregnancy Use optimal ART for the woman’s health Add ZDV to regimen to reduce perinatal HIV
transmission Discuss preventable risk factors Counsel on cesarean delivery Support decision-making by woman following
discussion of known and unknown benefits and risks
Acceptance or refusal of ART or ZDV should not result in denial of care or punitive action

Pregnancy Effects on HIVIn all women, the absolute CD4 count
decreases no matter whether HIV-positive or negative (pregnancy does not make HIV worse)
In HIV-positive women, percentage of CD4 cells should not change and viral load should not change because of pregnancy

Adult Treatment Guidelines
Clinical Category CD4+ count HIV RNA Recommendations Symptomatic
Asymptomatic,AIDS
Asymptomatic
Asymptomatic
Asymptomatic
Any value Any value
CD4+ T cells Any value<200/mm3
CD4+ T cells Any value >200/mm3 but <350 /mm3
CD4+ T cells >100,000 >350/mm3
CD4+ T cells <100,000 >350/mm3
Treat
Treat
Treatment should be offered
Most recommend deferring treatment, but some would treat.
Defer therapy

Antiretroviral Agents - 1
Nucleoside / nucleotide analogues (NRTIs) ABC ddI
FTC 3TC d4T
TDF ddC ZDV/ AZT
C – No studies. Concern for hypersensitivity B – Concern for lactic acidosis (do not use w/
d4T) B – No studies. C – Well tolerated. Widely used. C – Concern for lactic acidosis (do not use w/
ddI) B – No studies. Animal reports of bone abnls C – No studies. Teratogenic in animals. C – Well tolerated. The most experience.

Antiretroviral Agents - 2
Non-nucleoside RT inhibitors (NNRTIs) DLV EFV
NVP
C – No studies. D – Teratogenic. 4/142 birth defects. Avoid
in 1st trimester C – Well tolerated. Avoid initiating if CD4
>250 cells/mm3. Used as single-dose Rx in labor to prevent
perinatal transmission (consider adding ZDV/3TC for 3-7 days to reduce risk of NVP resistance) .

Antiretroviral Agents - 3
Protease inhibitors (PIs) APV ATV FPV IDV LP/r NFV RTV SQV TPV
C – No studies. Oral solution contraindicated. B – No studies. Concern hyperbilirubinemia C – No studies C – Unboosted: poor blood levels in preg C – No studies B – Registry data shows no incr in birth def B –Not used alone due to GI side effects B – Well tolerated, used boosted C – No studies

ART in Pregnant Women: NRTIsRecommended
agents
zidovudine
lamivudine
Efficacy studies and extensive experience
Zidovudine + lamivudine is the recommended dual NRTI backbone

ART in Pregnant Women: NRTIsAlternate
agents
abacavir
didanosine
emtricitabine
stavudine
Cases of lactic acidosis with didanosine + stavudine; use only if no other alternatives
Insufficient data to recommend
tenofovir No studies in human pregnancy; bone toxicity in monkey studies
Not recommended
zalcitabine Teratogenic in animals

ART in Pregnant Women: NNRTIs
Recommended
agent
nevirapine No evidence of teratogenicity
Increased risk of liver toxicity in women who start nevirapine with CD4>250; monitor closely, especially for first 18 weeks of therapy
Not recommended
efavirenz
delavirdine
Teratogenic in monkeys
Avoid in first trimester; consider after second trimester only if no other alternatives
Teratogenic in rodent studies

ART in Pregnant Women: PIsRecommended
agents
nelfinavir
saquinavir
(soft gel capsule)/ ritonavir
PK studies and extensive experience
Preferred PI for combination therapy
PK studies and moderate experience
Unboosted saquinavir: inadequate drug levels in pregnant women
No PK data on saquinavir hard gel capsule

ART in Pregnant Women: PIs
Alternate
agents
indinavir
lopinavir/
ritonavir
ritonavir
Lower drug levels during pregnancy
May require boosting with ritonavir; PK study underway
Concern for possible hyperbilirubinemia in the neonate
Limited experience; study underway
Dosing recommendations not established; may require increased dose during pregnancy
Lower drug levels in pregnancy
Minimal experience

ART in Pregnant Women: PIsInsufficient data to recommend
amprenavir
atazanavir
fosamprenavir
No studies in human pregnancy
Oral solution contraindicated (contains propylene glycol)
No studies in human pregnancy
Concern for possible hyperbilirubinemia in neonate
No studies in human pregnancy

ART in Pregnant Women: Fusion Inhibitors
Insufficient data to recommend
enfuvirtide No studies in human pregnancy

NRTI Toxicity Bone marrow suppression ZDV (AZT)
Anemia(1%- severe, 50%-mild) Mitochondrial toxicity
Related to inhibition of DNA polymerase ddC > ddI > d4T > ZDV > 3TC > ABC > TDF
Peripheral neuropathy(15-35%) ddC > ddI > d4T
Pancreatitis (6-10%) ddI > ddC > 3TC
Hypersensitivity rash (3-5%) Abacavir Not related to mitochondria

NRTI Toxicity During Pregnancy Symptoms may be subtle, insidious, and non-
specific Fatigue, nausea, anorexia, abdominal pain,
weakness May be synergistic with maternal changes
seen during pregnancy Overlaps with other complications of
pregnancy Acute fatty liver of pregnancy HELLP syndrome

Lactic Acidosis Lactic acidosis is a rare life-threatening complication
of antiretroviral therapy Nucleoside analogue therapy-induced mitochondrial
toxicity appears to be the cause of this syndrome Diagnosis is difficult because symptoms are vague
and non-specific Routine monitoring of lactate levels is not
recommended in asymptomatic patients; however, lactate should be measured in patients with unexplained weight loss, nausea, or abdominal pain
Treatment includes discontinuing NRTIs, followed by supportive care measures

Lactic Acidosis
Symptoms Nausea and
vomiting Abdominal pain Weight loss Malaise Dyspnea/tachypnea
Laboratory Findings Increased anion gap Increased lactic acid levels Increased lactate/pyruvate
Adapted from: Boxwell DE, Styrt BA. 39th ICAAC, San Adapted from: Boxwell DE, Styrt BA. 39th ICAAC, San Francisco, CA, 1999. Abstract 1284.Francisco, CA, 1999. Abstract 1284.

NNRTI Toxicities Rash 5-20%
Delavirdine > nevirapine > efavirenz
CNS 5% Dizziness, vivid dreams, psychiatric
Efavirenz >> nevirapine
Nausea/diarrhea Any
Liver toxicity 2-5% Nevirapine (400mg QD > 200mg BID; risk greater if CD4
count before initiation of NVP in women is >250 cells/mm3)
Fetal abnormalities Efavirenz


PI Toxicities
Lipodystrophy (up to 84%, severe in 12%)Glucose intolerance (up to 23%)Dyslipidemia (up to 90%)
Cutaneous changes, e.g., dry skin

Glucose MetabolismAbnormalities of glucose homeostasis
(primarily insulin resistance) are common in patients on ART
Higher incidence in patients receiving PIs
Mechanisms remain unclear at this timeTreatment with insulin-sensitizing
agents may be beneficial

Insulin Resistance
Increased insulin levels found Blood sugars normal State of compensated insulin resistance

Antiretroviral Pregnancy Registry Collaborative project managed by PharmaResearch
Corporation on behalf of an advisory committee (specialists in OB/GYN, ID, teratology, epidemiology, and CDC and NIH members) and sponsored by: Abbott Laboratories, Agouron Pharmaceuticals, Inc.,
Boehringer Ingelheim Company, Bristol-Myers Squibb, Co., Gilead Sciences, Inc., GlaxoSmithKline, F. Hoffmann-LaRoche Ltd., Merck & Co., Inc. and PharmaResearch.
Purpose: To assess safety of ARVs during pregnancy Telephone: (800) 258-4263 Fax: (800) 800-1052
available at http://www.apregistry.com

Antiretroviral Pregnancy Registry Through January 31, 2004 there were 5010
voluntarily reported prospective cases
www.apregistry.com



2.8%

3.7%

HIV and PregnancyPerinatal Transmission
Historical risk: 28% ACTG 076: 8% Effective ART (VL<50 copies/mm3) : <1% C-section: 50%

Perinatal HIV TransmissionDocumented transmission: intrauterine,
intrapartum, and postpartum through breastfeeding In utero 25%–40% of cases Intrapartum 60%–75% of cases Postpartum additional risk with
breastfeeding 14% risk with established infection 29% risk with primary infection

Perinatal HIV Transmission
In utero
At delivery
After delivery
Effective ART Decrease fetal trauma Intrapartum ART C-section Alternatives to breast feeding Postpartum prophylaxis for baby
TimingTiming InterventionIntervention

Risk Factors for Transmission HIV viral load (HIV-
RNA level) Genital tract viral load CD4 cell count Clinical stage of HIV Smoking cigarettes Substance abuse Vitamin A deficiency Unprotected sex with
multiple partners
STDs and other coinfections
Antiretroviral agents Preterm delivery Placental disruption Invasive fetal monitoring Duration of membrane
rupture (2% per hr) Breastfeeding Vaginal delivery vs.
cesarean section
Anderson J (ed). 2001. A Guide to the Clinical Care of Women with HIV, 2nd ed. U.S. Department of Health and Human Services, Health Resources and Services Administration: Rockville, Maryland.

ACTG 076 A phase III randomized placebo-controlled trial of
zidovudine (ZDV, AZT) for the prevention of maternal-fetal HIV transmission
Treatment Regimen Antepartum
100 mg ZDV po 5x day, started at 14-34 weeks gestation Intrapartum
During labor, 1- hour initial dose 2 mg/kg IV followed by continuous infusion of 1 mg/kg until delivery
Postpartum/Infant 2 mg/kg po q 6 hr for 6 weeks, started within 8-12 hours after birth

ACTG 076
Eligibility
Protocol ZDV 100 mg 5X day antepartum Placebo 2 mg/kg, 1 mg/kg/hr intrapartum 2 mg/kg q 6 hr infant thru 6wks
n=180 HIV status known n=185
Results HIV+ =13 67.5% reduction HIV+ = 40(8.3%) (25.5%)
pregnant HIV+ womenCD4 >200 cells/mm3
no symptoms or clinical indication for ZDVno prior ZDV
n= 477
p= 0.000006

ACTG 076 Follow-up Follow-up of uninfected infants PACTG 076
No significant differences in infant growth, development, or immune function in placebo vs. ZDV
No differences in Bayley developmental scores in uninfected infants (ACTG 219)
No other safety abnormalities have been identified Follow-up of infants with exposure to nucleoside
analogues is ongoing due to the potential for mitochondrial toxicity
In the U.S. no cases of mitochondrial toxicity have been identified

ACTG 076 Follow-up
Follow-Up of Mothers (ACTG 288) Median follow-up 4.2 years No substantial differences in CD4 count,
time to progression to AIDS, or death in women who received ZDV vs. placebo

ACTG 076 ProtocolShould be used as part of ART regimen
in all pregnant women, if possible Antepartum: AZT 300 bid or 200 tid po,
from week 14 until delivery Intrapartum: AZT 2 mg/kg IV over first
hour, then 1 mg/kg/hr until delivery Postpartum: (Infant): AZT syrup 2 mg/kg po
q 6h (or 1.5 mg/kg q 6h IV) x 6 wks

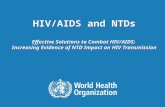
Viral Load and Transmission
00
16.616.6
21.321.3
30.930.9
40.640.6
HIV-1 RNAHIV-1 RNA Transmission %Transmission %
<1000 copies/mL<1000 copies/mL
1000 - 10,0001000 - 10,000
10,001- 50,00010,001- 50,000
50,001-100,00050,001-100,000
>100,000>100,000
NN
0/570/57
32/19332/193
39/18339/183
17/5417/54
26/6426/64
Women & Infants Transmission Study (WITS) Garcia, et al, NEJM 1999

0
20
40
60
HAART
Multi-ART
ZDV Mono (>4/94)
ZDV Mono (<4/94)
None
Maternal Delivery HIV RNA Levels and Antiretroviral Use are Independently Associated With Perinatal TransmissionCooper E et al. JAIDS 2002;29:484-94
Perinatal Transmission%
MTC
T

Studies of Short Course Therapy Oral ZDV in a non-breastfeeding population
(Thailand) from 36 weeks and during labor Transmission rate: 9.4 % ZDV vs 18.9 % placebo Lancet. 1999 Mar 6;353(9155):773-80
Petra study – intrapartum/postpartum oral ZDV/3TC in a breast-feeding population (Uganda, S. Africa, Tanzania) Transmission rate: 10% ZDV/3TC vs 17% placebo Lancet. 2002 Apr 6;359(9313):1178-86
HIVNet 012 – intrapartum/postpartum/neonatal nevirapine (NVP) vs short course/neonatal ZDV in a breast-feeding population (Uganda) Transmission rate: 12% NVP vs 21% ZDV Lancet. 1999 Sep 4;354(9181):795-802

Studies of Short Course Therapy Thai
18.9 % placebo 9.4 % ZDV
Petra study 17% placebo 10% ZDV/3TC
HIVNet 012 21% ZDV 12% NVP 0
5
10
15
20
25
Thai PETR O12

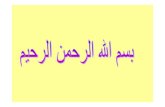
Suboptimal RegimensHIV transmission rates with partial ZDV
(AZT) regimens (New York cohort): 6.1% with prenatal, intrapartum, and
infant ZDV 10% with only intrapartum ZDV 9.3% with only infant ZDV started within
first 48 hours 26.6% with no ZDV

Suboptimal Regimens
0
5
10
15
20
25
30
Prenatal/Intrapartum/Infant ZDVOnly intraparutm ZDVInfant ZDV only by 48 hrs.No ZDV
The New York Cohort
HIV Transmission
%

Perinatal Guidelines USPHS Task Force
Recommendations for the Use of Antiretroviral Drugs in Pregnant HIV-1 Infected Women for Maternal Health and to Reduce Perinatal HIV-1 Transmission in the United States
Developed in 1994 in response to ACTG 076 Working Group reconvened in December 1999
and meets monthly Last Updated November 17, 2005

Clinical Scenario - 1 HIV-1-infected pregnant women who have not received
prior antiretroviral therapy. Pregnant women with HIV-1 infection must receive standard
clinical, immunologic, and virologic evaluation. Recommendations for initiation and choice of antiretroviral therapy
should be based on the same parameters used for persons who are not pregnant, although the known and unknown risks and benefits of such therapy during pregnancy must be considered and discussed.
The three-part ZDV chemoprophylaxis regimen, initiated after the first trimester, is recommended for all pregnant women with HIV-1 infection regardless of antenatal HIV RNA copy number to reduce the risk for perinatal transmission.
The combination of ZDV chemoprophylaxis with additional antiretroviral drugs for treatment of HIV-1 infection is recommended for infected women whose clinical, immunologic or virologic status requires treatment or who have HIV-1 RNA over 1,000 copies/mL regardless of clinical or immunologic status, and can be considered for women with HIV-1 RNA < 1,000 copies/mL.
Women who are in the first trimester of pregnancy may consider delaying initiation of therapy until after 10-12 weeks’ gestation.

Clinical Scenario - 2 HIV-1-infected women receiving antiretroviral therapy
during the current pregnancy. HIV-1 infected women receiving antiretroviral therapy in whom
pregnancy is identified after the first trimester should continue therapy.
ZDV should be a component of the antenatal antiretroviral treatment regimen after the first trimester whenever possible, although this may not always be feasible.
For women receiving antiretroviral therapy in whom pregnancy is recognized during the first trimester
The woman should be counseled regarding the benefits and potential risks of antiretroviral administration during this period
Continuation of therapy should be considered If therapy is discontinued during the first trimester, all drugs should be
stopped and reintroduced simultaneously to avoid the development of drug resistance.
Regardless of the antepartum antiretroviral regimen, ZDV administration is recommended during the intrapartum period and for the newborn.

Clinical Scenario – 3 (1)
HIV-1-infected women in labor who have had no prior therapy. Several effective regimens are available. These
include:1. intrapartum intravenous ZDV followed by six weeks of
ZDV for the newborn;2. oral ZDV and 3TC during labor, followed by one week of
oral ZDV-3TC for the newborn;3. a single dose nevirapine at the onset of labor followed
by a single dose of nevirapine for the newborn at age 48 hours; and
4. the two-dose nevirapine regimen combined with intrapartum intravenous ZDV and six week ZDV for the newborn.

Clinical Scenario – 3 (2)
HIV-1-infected women in labor who have had no prior therapy. If single-dose NVP is given to the mother, alone or
in combination with ZDV, consider adding maternal ZDV/3TC starting as soon as possible (intrapartum or immediately postpartum) and continuing for 3 to 7 days. This may reduce development of NVP resistance.
In the immediate postpartum period, the woman should have appropriate assessments (e.g., CD4 count and HIV-1 RNA viral load) to determine whether antiretroviral therapy is recommended for her own health.

Clinical Scenario - 4 Infants born to mothers who have received no antiretroviral
therapy during pregnancy or intrapartum. The six-week neonatal ZDV component of the ZDV chemoprophylactic
regimen should be discussed with the mother and offered for the newborn.
ZDV should be initiated as soon as possible after delivery - preferably within 6-12 hours of birth.
Some clinicians may choose to use ZDV in combination with other antiretroviral drugs, particularly if the mother is known or suspected to have ZDV-resistant virus.
However, the efficacy of this approach for prevention of transmission has not been proven in clinical trials, and appropriate dosing regimens for neonates are incompletely defined for many drugs.
In the immediate postpartum period, the woman should undergo appropriate assessments (e.g., CD4 count and HIV-1 RNA viral load) to determine if antiretroviral therapy is required for her own health. The infant should undergo early diagnostic testing so that if HIV-infected, treatment can be initiated as soon as possible.

Cesarean vs. Vaginal Birth Risk of transmission increased 2% each hour after
membranes have been ruptured Cesarean before labor and/or rupture of membranes
reduces risk of transmission by 50–80% compared with other modes of delivery in women on no antiretroviral therapy or on ZDV alone and VL >1000
No clear benefit with cesarean after onset of labor or membranes have been ruptured
Cesarean increases morbidity and possible mortality to mother
Give antibiotic prophylaxis for cesarean in HIV-infected women
Complications of similar to HIV uninfected women Patient’s decision should be respected and honored

Delivery Clinical Situation A HIV+ woman presenting late in pregnancy (after
36 weeks), not receiving ART, VL and CD4 count pending, unlikely to be available before delivery Discuss options for therapy Start ART, including at least 076 ZDV regimen Counsel about scheduled cesarean delivery If cesarean chosen, schedule for 38 weeks; start IV ZDV 3
hours before surgery Infant should receive 6 weeks ZDV after birth Discuss options for continuing/starting combination therapy
as soon as HIV viral load and CD4 count available

Delivery Clinical Situation B
HIV+ women who began prenatal care early in 3rd trimester, are receiving and responding to ART, but still have VL > 1000 at 36 weeks gestation Continue ART because VL is decreasing Inform woman
VL level falling but unlikely to be <1000 before delivery
Scheduled cesarean may reduce risk of intrapartum transmission
Increased risks of cesarean delivery If chosen, schedule cesarean for 38 weeks; start IV
ZDV 3 hours before surgery; continue other ART Infant should receive 6 weeks ZDV after birth Stress importance of adherence to therapy after
delivery

Delivery Clinical Situation C HIV+ women receiving ART with
undetectable VL at 36 weeks gestation Inform woman that her risk of perinatal
transmission is low (approximately 2% or less), even with vaginal delivery
Current information suggests cesarean will not lower her risk further
Cesarean delivery has increased risks of complication compared to vaginal delivery
Risks should be balanced against uncertain benefit of cesarean in this case
Infant should receive 6 weeks ZDV after birth

Delivery Clinical Situation D HIV+ women who have elected scheduled
cesarean delivery but present in early labor or shortly after rupture of membranes IV ZDV should be started immediately If cervical dilatation is minimal and a long period of labor is
anticipated administer loading dose of ZDV and proceed expeditiously with cesarean
Alternatively, consider oxytocin augmentation to expedite vaginal delivery
If labor is progressing rapidly—allow for vaginal delivery If allowed to labor, avoid invasive monitoring, and operative
delivery Continue oral ART during labor Infant should receive 6 weeks ZDV after birth

Obstetric ProceduresBecause of increased fetal exposure to
infected maternal blood and secretions, increased risk of transmission may come from: Amniotomy Fetal scalp electrode/sampling Forceps/vacuum extractor Episiotomy Vaginal tears

Adverse Pregnancy Outcomes
Pregnancy Outcome Relationship to HIV Infection
Spontaneous abortion Limited data, but evidence of possible increased risk
Stillbirth No association noted in developed countries; evidence of increased risk in developing countries
Perinatal mortality No association noted in developed countries, but data limited; evidence of increased risk in developing countries
Newborn mortality Limited data in developed countries; evidence of increased risk in developing countries
Intra-uterine growth retardation
Evidence of possible increased risk
Anderson J (ed). 2001. A Guide to the Clinical Care of Women with HIV, 2nd ed. U.S. Department of Health and Human Services, Health Resources and Services Administration: Rockville, Maryland.

Adverse Pregnancy Outcomes
Pregnancy Outcome Relationship to HIV Infection
Low birth weight Evidence of possible increased risk
Preterm delivery Evidence of possible increased risk, especially w/ more advanced disease
Pre-eclampsia No data
Gestational diabetes No data
Amnionitis Limited data; more recent studies do not suggest an increased risk; some earlier studies found increased histologic placental inflammation, particularly in those with preterm deliveries
Oligohydramnios Minimal data
Fetal malformation No evidence of increased risk
Anderson J (ed). 2001. A Guide to the Clinical Care of Women with HIV, 2nd ed. U.S. Department of Health and Human Services, Health Resources and Services Administration: Rockville, Maryland.

Breastfeeding and HIV Infection
Women with HIV infection in the U.S. should not breastfeed
Women considering breastfeeding should know their HIV status

Neonates Wash newborn after birth, especially face Avoid hypothermia ZDV (AZT) prophylaxis for 6 weeks
Hemoglobin at baseline and 6 wks Adherence
Referral to an HIV specialist HIV diagnostic testing to establish or rule out HIV
infection as early as possible Negative virologic tests during first 6 wks should be
repeated after completion of ZDV PCP prophylaxis initiated at 6 weeks of age Long-term follow-up of HIV- and ART-exposed
infants Support services for the family

Summary HIV testing in pregnancy should be universal Mother-to-child-transmission of HIV can be
reduced to < 2% with appropriate care Antiretroviral therapy including zidovudine Obstetric interventions
Avoid amniotomy Avoid procedures: forceps/vacuum extractor, scalp
electrode, scalp blood sampling Restrict episiotomy Elective cesarean section in certain cases
Neonate prophylaxis Avoid breastfeeding

HIV Services for Pregnant Women
Counseling and confidential testing Comprehensive medical care Case management Adherence counseling Mental health Support groups Clinical trials

Resources http://www.aidsinfo.nih.gov/guidelines
Guidelines for the Use of Antiretroviral Agents in HIV-Infected Adults and Adolescents
Updated October 6, 2005
Public Health Service Task Force Recommendations for Use of Antiretroviral Drugs in Pregnant HIV-1-Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV-1 Transmission in the United States
Updated November 17, 2005


Resources
www.aidsetc.org Perinatal Antiretroviral Guidelines Slide Set
[PPT]
Date: 11/2005Source: National Resource CenterNote: 68 slides, includes 6 case studies and speaker notes



References
Anderson J (ed). 2001. A Guide to the Clinical Care of Women with HIV, 2nd ed. U.S. Department of Health and Human Services, Health Resources and Services Administration: Rockville, Maryland.
Coutsoudis A et al. 1999. Influence of infant-feeding patterns on early mother-to-child transmission of HIV-1 in Durban, South Africa: A prospective cohort study. Lancet 354: 471–476.
DeCock K et al. 2000. Prevention of mother-to-child transmission in resource-poor countries: Translating research into policy and practice. J Am Med Assoc 283(9): 1175–1182.
Dunn D et al. 1992. Risk of HIV-1 transmission through breastfeeding. Lancet 340(8819): 585–588.
Gray G. 2000. The PETRA study: Early and late efficacy of three short ZDV/3TC combinations regimens to prevent mother-to-child transmission of HIV-1. XIII International AIDS Conference, Durban, South Africa.
Comparison of two strategies for administering nevirapine to prevent perinatal HIV transmission in high-prevalence, resource-poor settings Stringer JS, Sinkala M, Stout JP, Goldenberg RL, Acosta EP, Chapman V, Kumwenda-Phiri R, Vermund SH. J Acquir Immune Defic Syndr. 2003 Apr 15;32(5):506-13.

International Perinatal HIV Group. 1999. The mode of delivery and the
risk of vertical transmission of human immunodeficiency virus type 1. N Engl J Med 340(14): 977–987.
Mandelbrot L et al. 1996. Obstetric factors and mother-to-child transmission of human immunodeficiency virus type 1: The French perinatal cohorts. Amer J Obstet Gynecol 175(3 pt 1): 661–667.
Semprini AE et al. 1995. The incidence of complications after cesarean section in 156 women. AIDS 9:913–917.
Shaffer N et al. 1999. Short-course ZDV for perinatal HIV-1 transmission in Bangkok, Thailand: A randomized controlled trial. Lancet 353: 773–780.
Sperling RS et al. 1996. Maternal viral load, ZDV treatment, and the risk of transmission of HIV type 1 from mother to infant. N Engl J Med 335(22): 1621–1629.
UNICEF/UNAIDS/WHO Technical Consultation on HIV and Infant Feeding. 1998. HIV and Infant Feeding: Implementation of Guidelines. WHO: Geneva.
World Health Organization (WHO)/Joint United Nations Programme on HIV/AIDS (UNAIDS). 1999. HIV In Pregnancy: A Review. WHO/UNAIDS: Geneva.

HIV and infant feeding: issues in developed and developing countries
Jackson DJ, Chopra M, Witten C, Sengwana MJ. J Obstet Gynecol Neonatal Nurs 2003 Jan-Feb;32(1):117-27.
Nevirapine resistance after single dose prophylaxis Eshleman SH, Jackson JB. AIDS Rev 2002 Apr-Jun;4(2):59-63.
HIV Infection in Women: Selected Issues in Pregnancy Currier JS. Topics in HIV Medicine, International AIDS Society-USA May 2002. [PDF, 45K]
Antiretrovirals for reducing the risk of mother-to-child transmission of HIV infection Brocklehurst P, Volmink J Cochrane Database Syst Rev 2002:CD003510.
Effect of breastfeeding on mortality among HIV-1 infected women: a randomised trial Nduati R, Richardson BA, John G, Mbori-Ngacha D, Mwatha A, Ndinya-Achola J, Bwayo J, Onyango FE, Kreiss J. Lancet 2001 May 26;357(9269):1651-55. Free registration required.

Breastmilk RNA viral load in HIV-infected South African women: effects of
subclinical mastitis and infant feeding Willumsen JF, Filteau SM, Coutsoudis A, Newell ML, Rollins NC, Coovadia HM, Tomkins AM. AIDS 2003 Feb 14;17(3):407-14.
Timing of breast milk HIV-1 transmission: a meta-analysis John GC, Richardson BA, Nduati RW, Mbori-Ngacha D, Kreiss JK. East Afr Med J 2001 Feb;78(2):75-9.
Mastitis and transmission of human immunodeficiency virus through breast milk Semba RD. Ann N Y Acad Sci 2000 Nov;918:156-62. Reproduced with permission.
Vaginal lavage with chlorhexidine during labour to reduce mother-to-child HIV transmission: clinical trial in Mombasa, Kenya Gaillard P, Mwanyumba F, Verhofstede C, Claeys P, Chohan V, Goetghebeur E, Mandaliya K, Ndinya-Achola J, Temmerman M. AIDS 2001 Feb 16;15(3):389-96.