Gender: male Age: 12 y/o. Chief compliant Neck mass noted about 1 year.
53
Gender: male Age: 12 y/o
-
Upload
noah-baker -
Category
Documents
-
view
213 -
download
0
Transcript of Gender: male Age: 12 y/o. Chief compliant Neck mass noted about 1 year.

Gender: male Age: 12 y/o

Chief compliant
Neck mass noted about 1 year

Present illness This 12 y/o boy 何 o 銳 suffered from right neck mas
s (initial size: 3cm) for about 1 years . Therefore he came to KMUH for help in Oct 2006 and NP biopsy was done, it showed chronic inflammation. Biopsy of lymph node over right side of neck showed metastatic carcinoma. The primary lesion was unknown after a series of exam were done there. He had also been to CGMH and PET was arranged, which showed no primary site. Then he came to our ENT OPD for help in Aug 2007. PE showed previous op scar over right neck and bulging mass over nasopharynx. Then he received NP biopsy, and it showed nonkeratinizing undifferentiated carcinoma.

Present illness Under the impression of NPC with right neck metastas
is, he was admitted for tumor survey in Oct 2007. MRI revealed NPC with right side skull base involvement and multiple lymph nodes over carotid space and posterior triangle of bil. submandibular and neck region, the maxium one size about 2cm over the right side,and above 1.5cm over the left side noted. Abdominal sono showed hyperechoic area (1.2cm) in right lobe of liver, hemangioma or focal fatty liver change was suspected. Whole body bone scan showed no distant bony metastases except direct basal skull invasion. Radiotherapy was suggested then, but his family preferred traditional therapy. However, the mass over right side of neck progressed in size. So he was brought to our hospital again and he was referred to our department for further survey and CCRT.

Past and personal history:
– DM/HTN:denied– habit of Smoking: denied– habit of drinking: denied– habit of betel nuts chewing: (-)– drug allergy: unkown– Previous op history: (-)

Physical examination
General: consciousness clear HEENT: no pale conjunctiva, no icteric sclera
– Nasopharynx: bulging mass over right side – Neck:
• A neck mass about 3x6.5cm over right side of upper neck, firm, immovable
Chest: clear breathing sound, no rales, no wheezing Heart: regular heart beats, no murmurs Abdomen: soft & flat, no tenderness, normoactive bowel
sound Karnofsky scale: 90%

Lab data
EB-VCA IgA: 5.68(+), IgG: 5.63 (+)

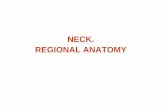
MRI (N/Y contrast), Nasopharynx (2007-10-31) (2008-04-17)
– lymph nodes noted over the carotid space and posterior triangle of bil. submandibular and neck region
• Right side: 2cm 2.7cm
• Left side: 1.5cm1.7 cm

2007-10-31 MRI

2008-04-17 MRI

Whole body bone scan (2007-11-01)– Direct basal skull invasion can't be ruled out. – No scintigraphic evidence of distant bony metas
tasis is demonstrable.
Whole body bone scan (2008-04-17)– similar focal mild uptake in basal skull.
– presence of growth plate activity over major app
endicular joints.
– no definite new bony abnormality elsewhere.

Sono, Upper abdomen (2007-10-31)– A small hyperechoic area (1.2cm) in right lob
e of liver, hemangioma or focal fatty liver change was first considered, regular ultrasound F/U was suggested, no other focal lesion in upper abdomen

Treatment planning
Energy and purpose: 6 MVX-rays with curative intent
Position: supine with mask Technique: SAD 100cm, IMRT with ? portals t
o cover tumor in nasopahrynx Dosage:
– Tumor in nasopahrynx and LN over bil. neck: 70Gy/35Fx/7weeks
– Bilateral level II ,III,IV and 1/2 of postrior nasal cavity and 1/3 of maxillary sinus: 63Gy/35Fx/7weeks

Childhood nasopharyngeal carcinoma: from biology to treatment
Lancet Oncol 2003; 4: 13–21

Childhood NPC close association with EBV infection
– high titer of IgG, IgA Undifferentiated histology High incidence of locoregionally advanced
disease and distant metastases

Epidemiology and aetiology Children under 16 years of age
– 1–2% of all patients with NPC in China,
– 2.4% in the UK– 7.2% in Turkey– 10% in the USA– 12%in Israel– 13% in Kenya– 14.5% in Tunisia– 18% in Uganda

Epidemiology and aetiology NPC constitutes 20–50% of all
primary nasopharyngeal malignant tumors in children– Median age: 13 years– Male : female = 1.8:1– Black people

Epidemiology and aetiology Genetic Risk factor:
– HLA A2 Bsin2 haplotype, Aw19, Bw46, and B17 types
– deletions of chromosomes 3p, 9p, 11q,13q, and 14q
– inactivation of p53, rearrangements in retinoblastoma (RB2/p130) tumor suppressor genes, and genetic polymorphism of the CYP2E1 gene

Invasiveness:– Gains of genes on chromosome 12 – allelic loss on 11q, 13q, and 16q
metastatic disease– mutation of p53 – aberrant expression of cadherins

High titer of IgA, IgG– particularly those with the undifferentiated form
of the disease– IgA antibodies specific to EBV are used as marker
s for screening– Good indicator for disease activity
High concentrations of antibodies against ZEBRA (BamH1 Z Epstein-Barr replication activator)– ZEBRA is a nuclear transactivator that induces vir
al production by infected cells– IgGZ may be a useful marker for the follow-up of
young patients with NPC

NPC & EBV Clonal EBV genomes are found in cells that f
orm early preinvasive dysplastic lesions– EBV infection is an early event in multistep carci
nogenesis of NPC EBV
– double-stranded DNA molecule that encodes more than 100 genes of which only 10 are expressed in latently infected cells in vitro
– 6 nuclear proteins (EBNAs),– 2 membrane proteins (LMPs),– 2 non-translated RNA molecules (EBER)

EBNA1– Expressed in nearly all cases of EBV-positive NPC – important in replication and maintenance of t
he viral genome during cell division LMP1
– Oncogenic substance• upregulates several cellular proteins that inhibit apop
tosis, including BCL-2 and A20, and binds to numerous• Binds to proteins associated with the tumor necrosis-fa
ctor receptor– expressed in almost two thirds of EBV positive
NPC tumors

LMP2– Prevents reactivation of the virus by bl
ocking phosphorylation by tyrosine kinases
EBER– Do not encode proteins– important for oncogenesis and resistanc
e to programmed cell death (apoptosis).

pathogenesis of childhood NPC– multistep process involving EBV infecti
on that leads to increased expression of LMP1 and p53 in epithelial cells
– oncoprotein BCL-2 is highly expressed in 80% of adults with NPC, it is probably not associated with paediatric NPC.

Immune suppression T-cell immunity to EBV
– suppression of EBV-infected B-cell proliferation and the growth and invasion of NPC tumors
– ratio of CD4 to CD8 is reduced– production of interleukin 2 and its receptor is de
creased– the numbers of CD8-positive cells in peripheral
blood and the tumor are increased interferon-β could be useful for immunosti
mulation because of its direct and indirect effects on tumor cells

Histopathology Type I: keratinising squamous-cell carcin
oma– Keratin production
type II :non-keratinising epidermoid carcinoma– IIa: pleiomorphism– IIb: lymphoid infiltration
type III :undifferentiated carcinoma– IIIa: Large nucleoli and eosinophilic cytoplas
m– IIIb: small nucleoli and basophilic structure

The most common histopathological type in children is WHO type III

Clinical presentation The most common presenting sympto
m is a painless mass in the upper neck– nasal obstruction– blood-tinged drainage– Bleeding– conductive hearing loss or serous otitis c
aused by obstruction of the eustachian tubes
– Earache and tinnitus

Clinical presentation
Tumor invade the base of the skull..– Drooping of the upper eyelid– displacement of the eyeball, eye pain, los
s of vision, double vision– Difficulty swallowing– spasms of masticatory muscles– Disturbances of taste and voice can also
occur– Headache, facial pain, and neck pain


Clinical presentation Distant metastatic regions
– bones (67%) – liver(30%)– bone marrow (23%)– lungs (20%), and mediastinum

Diagnosis and staging MRI
– detection of the primary tumour and the extent of locoregional spread including nodal metastasis and perineural extension
CT– identification of bone erosion

More than 80% of children with NPC present with stage IV locoregional advanced disease

Lab data– LDH > 500IU/ml poor prognosis– Viral caspid antigen IgA and ZEBRA protein c
oncentration• Monitoring disease recurrence

Treatment and prognosis Surgical therapy
– unresectable due to complex anatomical location of disease
– radical neck dissection is appropriate • primary tumor seems to be controlled • persistent neck nodes following
chemoradiation• isolated recurrence in the neck occurs
after radiotherapy

Treatment and prognosis Radiotherapy
– Undifferentiated NPC is very sensitive to radiation
– R/T alone• 5-year survival: 20–60% in most paediatric series• Local control could be achieved by doses of 35–65
Gy– optimum dose for sustained control of NPC in children is
not yet known• Doses of 50–72 Gy directed to the primary tumor ar
e recommended for patients older than 10 years– 5–10% reduction in this dose is recommended for childre
n younger than 10 years of age

clinical target volume (CTV)– the nasopharynx– posterior 2 cm of nasal cavity– Posterior ethmoid sinuses– entire sphenoid sinus and basioccipital bone– cavernous sinus– base of skull (7–8 cm width encompassing the fora
men ovale carotid canal, and foramen spinosum laterally)
– pterygoid fossae– posterior one third of the maxillary sinus– oropharyngeal wall to the midtonsillar fossa– retropharyngeal nodes– bilateral cervical nodes– supraclavicular nodes

If the tumor has invaded the base of the skull or if cranial nerves II–VI are involved– superior border should be raised to include
• Pituitary gland, the base of the brain in the suprasellar area, the adjacent middle cranial fossa, and the posterior portion of the anterior cranial fossa
If the tumor extends into the anterior nasal cavity – a single anterior field may be necessary.


Total dose of 65–70 Gy– daily fractions of 1·8–2·0 Gy– 5 days a week.
The spinal cord, brain stem, and optic nerve are shielded after 45–50 Gy
The posterior lymphatic chains are treated with electron beams.
The lower cervical and supraclavicular regions are treated with a single anterior portal and a median shield to protect the larynx the spinal cord, with doses of 45–50 Gy
Clinically involved neck areas are boosted with direct oppositional fields to doses of 65–70 Gy by 6–13 MeV

IMRT: smaller dose to normal tissue, improved coverage of the primary tumor, skull base and nodal regions

Survival rate Stage:
– T stage • T1–2 :75% • T3–4: 37%
– N stage • N0: 64% • N3: 36%
– Metastatic disease at presentation :<10% Irradiation dose:
– < 60 Gy: 10-36%– > 60 Gy: 60-76%

Relapses! Most occur in the first 2 years > 50 % patients have overt distant
metastases

Adverse events Acute complications
– grade 2–3 skin reactions and mucositis leading to dysphagia and weight loss
Chronic complication– Late endocrine effects
• hypopituitarism (stunted growth,thyroid dysfunction (73%), and fertility defects)
• reported in 30% of long-term survivors– xerostomia (dry mouth;45–100%), chronic sinusitis
(73%), dental caries (bacterial tooth erosion; 15–30%), ear inflammation or hearing loss (18%), neck fibrosis (10–64%), encephalopathy (18%),second malignancies (6–8%), occasional facial motor disturbance
– Rare: Osteoradionecrosis, cranial-nerve dysfunction, hypoplasia, and fibrosis of facial bones

Treatment and prognosis Chemotherapy
– adriamycin, epirubicin, cisplatin, and bleomycin are the most active agents for treatment of NPC
– Neoadjuvant cisplatin-based chemotherapy• early eradication of microscopic disease and decrease i
n primary tumour mass before radiation• International randomised trial
– adults with stage IV undifferentiated NPC– a significant difference in disease-free survival between p
atients who receive 3 courses of cisplatin, bleomycin, and epirubicin and those receiving radiotherapy alone (42% at 4 years with chemotherapy versus 29% with radiotherapy;p<0·001)
– No difference in overall survival• 2 courses of cisplatin and fluorouracil induction, but sh
owed no benefit from chemotherapy over radiotherapy alone

– Concomitant chemoradiotherapy • eradicate local occult metastatic disease by r
adiosensitisation • the systemic effects of cytotoxic agents.• concomitant cisplatin and radiotherapy follo
wed by 3 courses of adjuvant cisplatin and fluorouracil is now the standard of care for adults with NPC in the USA
– childhood NPC: not yet been determined

Treatment and prognosis immunostimulative interferon therapy
– interferon- β • antitumour effects in EBV-positive NPC• antiproliferative and directly cytotoxic to tumou
r cells.• enhances the expression of cell-surface antigen
on tumour cells– indirect antitumour effects via activation of macroph
ages and monocytes, T cells, and natural killer cells.– inhibits suppressor T lymphocytes induced by the tu
mour and activates cytotoxic and natural killer cells

– Interferon- β• Adminstered following C/T and R/T: 15–25%
response rate• Germany, prospective multicentre trial in chil
dren with advanced stage NPCPreradiation chemotherapy with cisplatin, fluorou
racil, andMethotrexate followed by radiotherapy (60 Gy to primary and 45
Gy to uninvolved areas)and interferon- β treatment (10 U/kg 3 times a we
ek for 6 months) 91% response rate !!



Metastatic and recurrent disease 20–50% of patients still suffer from recurr
ent or metastatic disease– Most within 1-2 years of diagnosis– 48% of relapses occurred at distant sites onl
y– 43% at local and regional sites– 9% both at distant and locoregional regions.
Median survival– 3–6 months in untreated patients – 8–12 months for those treated by chemother
apy

Metastatic and recurrent disease Chemotherapy:
– Cisplatin and ifosfamide, weekly PF (cisplatin, fluorouracil), and interferon are also combinations that are used in recurrent disease.• Response rates are around 60–90% • Complete response about 20%
Second line irradiation or brachytherapy– Locoregional recurrence– Severe complication– 5-year survival of about 40%

Conclusion
Early administration of an effective chemotherapeutic agent is needed for treatment of childhood NPC– Advanced stage– This tumor type is sensitive to chemotherapy