
Traumatology · from the upper section of the clavicle and the acromion. By hol-ding off the...
14
Traumatology ISIS INTEGRIERTES SCHULTER-IMPLANTAT-SYSTEM Entwickelt in Zusammenarbeit mit Prof. Dr. med. K.-K. Dittel INTEGRATED SHOULDER IMPLANT SYSTEM Developed in cooperation with Prof. Dr. med. K.-K. Dittel
Transcript of Traumatology · from the upper section of the clavicle and the acromion. By hol-ding off the...

Traumatology
ISISINTEGRIERTES SCHULTER-IMPLANTAT-SYSTEM
Entwickelt in Zusammenarbeit mit Prof. Dr. med. K.-K. Dittel
INTEGRATED SHOULDER IMPLANT SYSTEM
Developed in cooperation with Prof. Dr. med. K.-K. Dittel
ISIS – Integriertes Schulter-Implantat-System
Einleitung
Der weltweite Anstieg der Sportaktivitäten führt zueiner hohen Rate an knöchernen, ligamentären oderkombinierten Verletzungen am Schultergelenk. Unsere Bemühungen, eine Verbesserung der operati-ven Resultate durch Reduktion der Komplikationsratenzu erzielen, sollten unter dem Aspekt des Schultertrau-mas nicht vernachlässigt werden.
Die operativen Standardverfahren am Schultergelenkweisen nach Literaturangaben langfristig Komplikati-onsraten zwischen 5 % und 20 % auf. Abhängigkeitenfinden sich in Bezug auf das verwendete Implantat, die Operationstechnik und die Patienten-Compliance.
Die Proportionen der neuen Implantate nehmen beson-dere Rücksicht auf die anatomischen Gegebenheiten derSchulter. Sie haben entscheidende Vorteile in Bezugauf die Weichteilsituation am Schultergelenk. Die Funktionsstabilität der neuen Titanplatten ist ex-zellent und garantiert frühe Übungsstabilität mit eineraußergewöhnlich niedrigen Komplikationsrate.
K. K. Dittel
Vorteile
Biokompatibles Titanimplantat
Exakte anatomische Passform
multidirektionale winkelstabile Schrauben +/- 20°
Winkelstabile Osteosynthese
Bedarfsgerechte multidimensionale Fixationsmöglichkeit
Optimale Weichteilschonung
Kein subacromiales Impingement
Spezielle Oberflächenbehandlung der Plattenminimiert Ermüdung und Abrieb des Materials
Verjüngung der Plattenstege vereinfacht die Anpassung der Platte an den Knochen.
•
•
•
•
•
•
•
•
•
Entwickelt in Zusammenarbeit mit Prof. Dr. med. K.-K. Dittel
Introduction
The worldwide increase of sporting activities is leadingto a high rate of bony, ligamentary or combinated injuriesat the shoulder joint. The efforts to improve the opera-tive results by reducing complications should not beneglected under the special item of the traumatizedshoulder.
The implants being used in trauma surgery at theshoulder joint include complication rates ranging from5 % up to 20 % due to the operative technique, theskill of the surgeon and the patient´s compliance.
The proportions of the new implants regard the anato-mical structures of the shoulder to a very high degreewith decisive advantages concerning the soft tissuesituation at the shoulder joint. The functional stabilityof each individual plate is excellent for its purpose and its efficiency guarantees early functional physiotherapywith an extraordinary low complication rate.
K. K. Dittel
Advantages
Biocompatible titanium alloy
Excellent anatomical adaptability
multidirectional locking screws +/- 20°
Functional angle-stable osteosynthesis
Optional multidimensional fixation
Optimal soft tissue preservation
Missing subacromial impingement
Special surface treatment of the plates minimizes material fatigue and abrasion
Thinning the ribs of the plate facilitates plate adaptation to bone contours
33
•
•
•
•
•
•
•
•
•
ISIS – Integrated Shoulder Implant system
Developed in cooperation with Prof. Dr. med. K.-K. Dittel

ACP Akromion-Klavikula-Platte
• AC-Luxation (Typ Tossy III, Rockwood III – V)
• laterale Fraktur der Klavikula
Fig.1a/b: Supraklavikulärer Hautschnitt entlang dem Akromion und
der lateralen Klavikula. Subperiostales Ablösen des M. deltoideus
vom oberen Anteil der Klavikula und des Akromions. Durch Weg-
halten der Muskulatur kann das Akromioklavikulargelenk sowie der
Processus coracoideus mit den Ligg. conoideum und trapezoideum
dargestellt werden.
Fig. 1a/b: Supraclavicular incision along the acromion and the
lateral clavicle. Subperiosteal detachment of the deltoid muscle
from the upper section of the clavicle and the acromion. By hol-
ding off the muscles, the acromioclavicular (AC) joint and the
coracoid process can now be exposed together with the conoid
and trapezoid ligaments.
Fig.2: Am posterioren Rand des AC-Gelenkes wird stumpf ein-
gegangen und der Haken der ACP 26-184-10 (rechts) oder
26-184-11 (links) eingeschoben, so dass er mittig unter dem
Akromion zu liegen kommt. Ein zusätzliches Anpassen der seit-
lichen Flügel der Platte an die anatomische Form der lateralen
Klavikula kann durch die Verwendung der beiden Biegeeisen
26-185-20 erfolgen.
Fig. 2: A blunt incision is made at the posterior edge of the AC joint
and the hook of the ACP 26-184-10 (right) or 26-184-11 (left) is
inserted so that it will rest centrally underneath the acromion.
Additional adaptation of the lateral wings of the plate to the anato-
mical shape of the lateral clavicle may be necessary, using the two
bending irons 26-185-20.
ACP Acromion Clavicle Plate
• AC-Luxation (Type Tossy III,Rockwood III – V)
• lateral fracture of the clavicle
OperationsverfahrenOperative Technique

55
Fig.3: Die Platte kann nun mittels geeigneter Repositionszangen
(z.B. 23-757-01)an der Klavikula temporär fixiert und sukzessive
angeschraubt werden. Das laterale Plattenloch ist für die Aufnah-
me einer winkelstabilen Schraube 26-102-XX (Ø 2,7 mm) oder
26-104-XX (Ø 3,5 mm) vorgesehen. Bei Vorliegen einer zusätz-
lichen lateralen Fraktur der Klavikula kann die längere ACP
26-184-10 (rechts) oder 26-184-11 (links) verwendet werden.
Auch bei dieser Platte ist das laterale Plattenloch für die Aufnah-
me einer winkelstabilen Schraube 26-102-XX (Ø 2,7 mm) oder
26-104-XX (Ø 3,5 mm) vorgesehen.
Fig. 3: The plate can now be temporarily fixed to the clavicle with
suitable repositioning pliers (i.e. 23-757-01) and can then be
screwed in place step by step. The lateral plate hole is intended
to hold a fixed-angle screw 26-102-XX (Ø 2.7 mm) or 26-104-XX
(Ø 3.5 mm). If a lateral clavicle fracture is involved as well, the
longer ACP 26-184-10 (right) or 26-184-11 (left) can be used.
This plate also has a lateral hole for insertion of a fixed-angle
screw 26-102-XX (Ø 2.7 mm) or 26-104-XX (Ø 3.5 mm).
Fig.4a/b: Die Operationswunde wird nach Einlage einer Redondrai-
nage schichtweise verschlossen.
Die zylindrische Form und die abgerundeten Kanten des Hakenan-
teils der Implantate verhindern eine Schädigung der Gelenkflächen
während der postoperativen Phase. Der Patient wird angehalten,
während dieser Zeit den Oberarm nicht über eine Winkelstellung
von 90° zu abduzieren, um einen Hakenbruch zu vermeiden.
Mechanisch überbeanspruchende Bewegungsabläufe in anderen
Bewegungsebenen sind ebenfalls zu unterlassen. Nach Ausheilung
der ligamentären Verletzungen des Bandapparates des Akromio-
klavikulargelenkes wird das Implantat im Regelfall 6 Wochen
postoperativ entfernt.
Fig. 4a/b: Following placement of a redon drain, the wound is then
closed layerwise.
The cylindrical shape and the rounded edges of the hook section
of the implants prevent joint surface damage during the postope-
rative phase. To prevent hook fracture, the patient is required not
to abduct the upper arm beyond an angle of 90 degrees during
this period. Mechanically straining movements in other movement
planes should also be avoided. Once the injuries of the ligament
apparatus of the acromioclavicular joint have healed up, the
implant can be removed – usually 6 weeks after the operation.

BCP Bi-kortikale Platte
• dislozierte proximale Humeruskopffraktur
• dislozierte Fraktur des Tuberculum majus
Fig.1a/b: Die Inzision der Haut beginnt in der Höhe des Akromio-
klavikulargelenkes, verläuft in gerader Richtung anterolateral in
kaudaler Richtung bis in Höhe des Ansatzes des M. deltoideus.
Der Sulcus deltoideopectoralis und die V. cephalica werden nach
medial abgehalten (Deltoideussplit).
Fig. 1 a/b: The skin incision begins at the level of the acromio-
clavicular joint, takes a straight anterolateral course in caudal
direction up to the point of insertion of the deltoid muscle. The
deltopectoral sulcus and the cephalic vein are then located and
retracted medially (split of the deltoid muscle!).
Fig.2: Etwa 2 Querfinger lateral des Sulcus wird unter Schonung
der V. cephalica der M. deltoideus etwa 1 cm stumpf eröffnet und
entsprechend der benötigten Plattenlänge in Längsrichtung stumpf
gespalten. Eine Verletzung des Ramus deltoideus der A. thoraco-
acromialis ist zu vermeiden. Die Ränder des M. deltoideus können
nun nach lateral und medial abgehalten werden. Die Faszie wird
parallel zu den Fasern des kurzen Bizepskopfes längs inzidiert, die
Gelenkkapsel und der proximale Anteil des Humerus dargestellt.
Das Schultergelenk wird über den vorderen Zugang eröffnet.
Fig. 2: Approximately two finger widths laterally of the sulcus, a
blunt incision of about 1 cm is made into the deltoid muscle while
preserving the cephalic vein, followed by blunt splitting of the
deltoid muscle in longitudinal direction as far as required for the
length of the plate.
The deltoid ramus of the thoracoacromial artery should not be
injured in this process. The edges of the deltoid muscle can now
be held off in lateral and medial direction. The fascia is incised
longitudinally parallel to the fibers of the short head of biceps and
the joint capsule and the proximal section of the humerus are then
exposed. The shoulder joint is opened through the frontal access.
The shoulder joint is opened through the frontal access.
BCP Bi-Cortical Plate
• dislocated proximal numeral head fracture
• dislocated fracture of the tuberculum majus
OperationsverfahrenOperative Technique

7
Fig.3: Nach sparsamem Abschieben des Perio-
stes wird die Fraktur reponiert und die Platte
probeweise so angelegt, dass das proximale Ende
der Platte ca. 1 cm unterhalb der Apex des
Humeruskopfes antero-lateral zum Liegen kommt.
Diese Positionierung des Implantates verhindert
ein Impingement während der postoperativen
Mobilisation. Eine Anpassung der seitlichen Flü-
gel der Platte im Kopfteil an die anatomische
Form des distalen Anteils des Humeruskopfes
kann durch die Verwendung der beiden Biegeei-
sen 26-185-20 notwendig sein.
Fig. 3: After peeling off as little of the periosteum
as possible, the fracture is reduced and the plate
is applied testwise so its proximal end lies antero-
lateral approx. 1 cm below the apex of the head
of humerus. This implant position prevents a
possible impingement during the postoperative
mobilization. It may be necessary to adapt the
lateral wings of the plate’s head section to the
anatomical shape of the distal section of the
head of humerus, using the two bending irons
26-185-20.
Fig. 5: Die Operationswunde
wird nach Einlage einer
Redondrainage schichtweise
verschlossen.
Fig. 5: Following placement
of a redon drain, the wound
is then closed layerwise.
Fig. 4: Das Kopffragment wird nun mit der Platte verschraubt.
Alle runden Löcher im Kopfteil der Platte können mit winkel-
stabilen Schrauben 26-102-XX (Ø 2,7 mm) oder 26-104-XX
(Ø 3,5 mm) besetzt werden. Im Zentrum des Kopfteils befindet
sich ein Schraubengewinde in 20° Winkelstellung nach kranial
geneigt, welches mit winkelstabilen Schrauben 26-102-XX
(Ø 2,7 mm) oder 26-104-XX (Ø 3,5 mm) besetzt werden kann.
Diese Schraube wirkt mit ihrem abstützenden Effekt einem
eventuellen postoperativen Korrekturverlust im Sinne einer
Varuskippung entgegen.
Anschließend können die Schraubenlöcher in den beiden
Schenkeln des Implantats besetzt werden. Die beiden Brücken
im Zentrum des Implantatkopfes dienen zur Fixierung der
distalen Sehnenansätze der Muskulatur der Rotatorenman-
schette, die mittels nicht resorbierbaren Fäden fixiert werden
können.
Fig. 4: The head fragment is now fixed to the plate using
screws. All round holes in the plate’s head section can be
filled with fixed-angle screws 26-102-XX (Ø 2.7 mm) or
26-104-XX (Ø 3.5 mm). The center of the head section
features a screw thread arranged at a 20-degree angle towards
cranial, for which fixed-angle screws 26-102-XX (Ø 2.7 mm)
or 26-104-XX (Ø 3.5 mm) can be used as well. The supporting
function of this screw prevents a potential postoperative loss
of correction in the form of a varus tilt.
Thereafter, the screw holes located in the two legs of the
implant can be filled. The two bridges in the center of the
implant’s head are intended for the fixation of the distal ten-
don insertions of the rotator cuff muscles, for which purpose
non-resorbable sutures can be used.
OperationsverfahrenOperative Technique
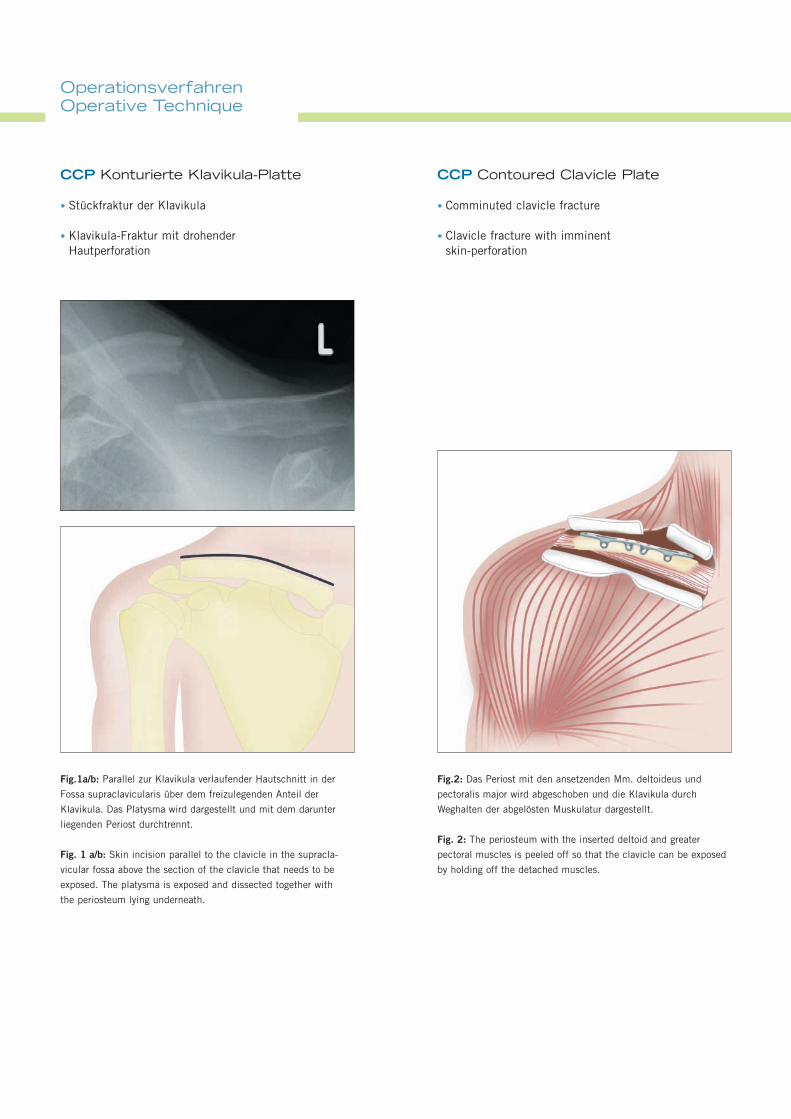
CCP Konturierte Klavikula-Platte
• Stückfraktur der Klavikula
• Klavikula-Fraktur mit drohender Hautperforation
Fig.1a/b: Parallel zur Klavikula verlaufender Hautschnitt in der
Fossa supraclavicularis über dem freizulegenden Anteil der
Klavikula. Das Platysma wird dargestellt und mit dem darunter
liegenden Periost durchtrennt.
Fig. 1 a/b: Skin incision parallel to the clavicle in the supracla-
vicular fossa above the section of the clavicle that needs to be
exposed. The platysma is exposed and dissected together with
the periosteum lying underneath.
Fig.2: Das Periost mit den ansetzenden Mm. deltoideus und
pectoralis major wird abgeschoben und die Klavikula durch
Weghalten der abgelösten Muskulatur dargestellt.
Fig. 2: The periosteum with the inserted deltoid and greater
pectoral muscles is peeled off so that the clavicle can be exposed
by holding off the detached muscles.
CCP Contoured Clavicle Plate
• Comminuted clavicle fracture
• Clavicle fracture with imminent skin-perforation

9
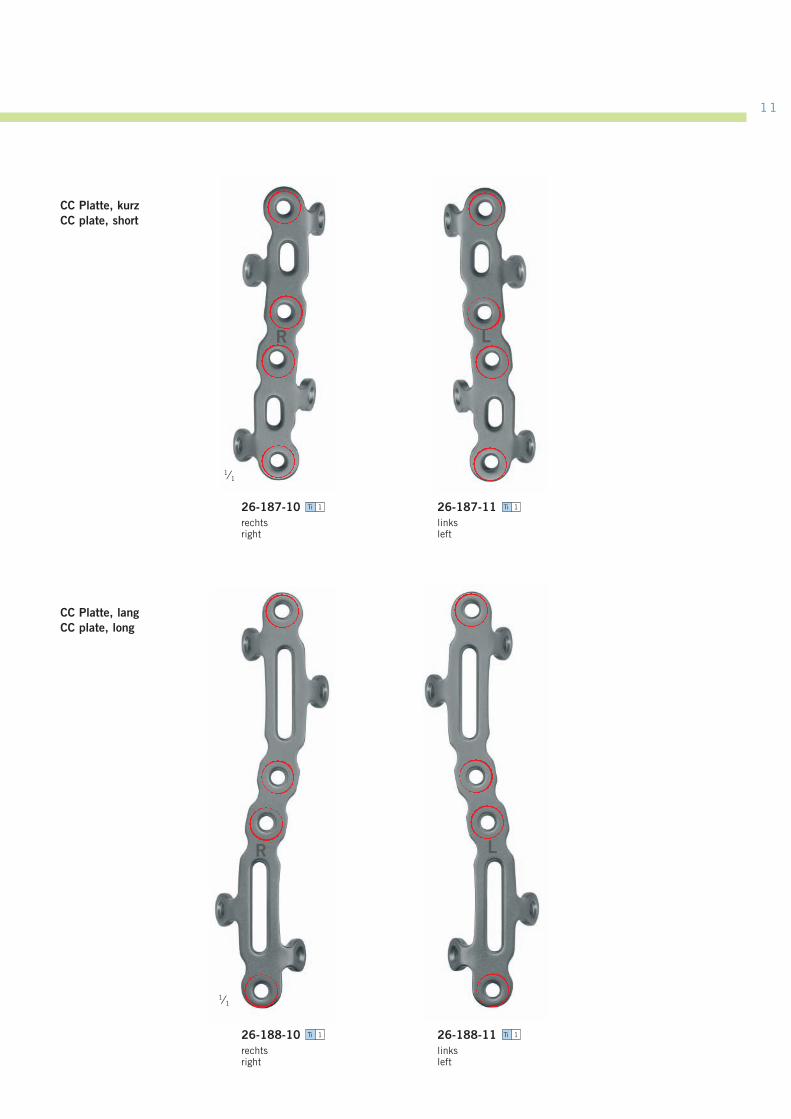
Fig.3: Bei Querbrüchen oder kurzen Schrägbrüchen kommt die
kurze CCP 26-187-10 (rechts) oder 26-187-11 (links) bevorzugt
zur Anwendung. Beim Vorliegen eines 3. Fragmentes und instabilen
dislozierten Frakturen kann die lange CCP 26-188-10 (rechts)
oder 26-188-11 (links) indiziert sein. Die Schraubenlöcher im
Plattenkörper können mit den winkelstabilen Schrauben 26-102-XX
(Ø 2,7 mm) oder 26-104-XX (Ø 3,5 mm) besetzt werden.
Fig. 3: For transverse fractures or short oblique fractures, the short
CCP 26-187-10 (right) or 26-187-11 (left) is preferable. If a third
fragment is involved or an unstable dislocated fracture needs treat-
ment, the long CCP 26-188-10 (right) or 26-188-11 (left) may be
indicated. The screw holes of the plate body can be filled with the
fixed-angle screws 26-102-XX (Ø 2.7 mm) or 26-104-XX (Ø 3.5 mm).
Fig.4a/b: Die Operationswunde wird nach Einlage einer Redon-
drainage schichtweise verschlossen.
Fig. 4 a/b: Following placement of a redon drain, the wound is
then closed layerwise.

PlattenPlates
26-186-10rechtsright
Ti 1 26-186-11linksleft
Ti 1
AC Platte, kurzAC plate, short
AC Platte, langAC plate, long
26-184-10rechtsright
Ti 1
BC PlatteBC plate
26-190-01 Ti 1
26-184-11linksleft
Ti 1
1⁄1
1⁄1
2,5 mm
R L
R L
20° 20°
40°
“Multidirectional“
1 Unit(s)Ti Titanium
11
CC Platte, kurzCC plate, short
CC Platte, langCC plate, long
1⁄1
26-188-11linksleft
Ti 1
26-187-10rechtsright
Ti 1 26-187-11linksleft
Ti 1
R L
R L
26-188-10rechtsright
Ti 1
1⁄1

ACPBroos P. et al.: Acromio-clavicular dislocations Type IIIEur. J. Trauma 2002; Vol. 28: 11 – 15
Henkel Th. et al.: Die Behandlung der frischen AC-Luxation Tossy III durch Band-naht und temporäre Fixation mit Klavikula-HakenplatteSwiss Surg. 1997; 3: 160 - 166
Hackenbruck W. et al.: Operative Behandlung der lateralen Klavikula-Fraktur mit derKlavikula-HakenplatteZ. Unfallchir. Vers. Med. 1994: Band 87, Heft 3
Bäthis H., et al.: Stand der Therapie der SchultereckgelenksverletzungUnfallchirurg 2001; 104: 955 - 960
Kilburger G.R.E.: Behandlungsergebnisse nach operativer Therapie von Frakturen und lateralen Luxationen der KlavikulaDissertation Universität Tübingen 2002
BCPKohler H. et al.: Oberarmkopffrakturen – Indikationen zur OsteosyntheseOP-Journal 2002; 18: 230 – 236
Wijgman A.J. et al.: Open reduction and internal fixation of 3 and 4 part fractures of the proximal part of the humerusJ.B.J.S. 2002: Vol. 84 A, 1919 – 1925
Vogt F. et al.: Internal fixation of proximal humeral fractures with the blade plate Osteosynthesis and Trauma Care 2002; 1: 8 – 12
Hessmann M.H. et al.: Die winkelstabile Plattenosteosynthese am proximalen HumerusAkt. Traumatologie 2003; 33: 2 – 6
Blum J. et al.: Behandlung proximaler metaphysärer Humerusfrakturen mit Verriegelungsmarknagelung und Spiralklinge – Erste Erfahrungen mit einem neuen ImplantatAkt. Traumatologie 2003; 33: 7 – 13
LiteraturübersichtLiterature
•
•
•
•
•
•
•
•
•
•
CCPSchwarz N. et al.: The treatment of the shaft fractures of the clavicleEur. J. Trauma 2001; 27: 211 – 217
Boestmann O. et al.: Complications of plate fixation in fresh displaced claviculafracturesJ. Trauma 1997: 43: 778 – 783
Schwarz N.: Verletzungen und Verletzungsfolgezustände des SchlüsselbeinsOP-Journal 2002; 18: 238 – 243
Krackhardt T. et al.: Oberarmkopffrakturen – Indikationen zur EndoprotheseOP-Journal 2002; 18: 238 – 243
Stahlenbrechner A. et al.: Instabile subkapitale OberarmfrakturenTrauma und Berufskrankheit 2001; 3: 5540 - 5543
Dittel K.-K., Rapp M.ISIS: Integrated Shoulder Implantation SetOsteo Trauma Care 2002; 10:205-207
•
•
•
•
•
•

1919

09.07 . 90-128-16-05 . Printed in Germany · Copyright by Gebrüder Martin GmbH & Co. KG · Alle Rechte vorbehalten · Technische Änderungen vorbehaltenWe reserve the right to make alterations · Cambios técnicos reservados · Sous réserve de modifications techniques · Ci riserviamo il diritto di modifiche tecniche
Gebrüder Martin GmbH & Co. KGA company of the KLS Martin GroupLudwigstaler Str. 132 · D-78532 TuttlingenPostfach 60 · D-78501 TuttlingenTel. +49 7461 706-0 · Fax +49 7461 [email protected] · www.klsmartin.com
KLS Martin Subsidiaries
KLS Martin France SARL 3, Rue Gambetta 68000 Colmar France Tel. +33 3 89 21 6601 Fax +33 3 89 23 6514 [email protected]
Martin Italia S.r.l.Via Paracelso, 18Palazzo Andromeda, Ingresso 2 20041 Agrate Brianza (Mi) ItalyTel. +39 039 605 6731 Fax +39 039 605 [email protected]
Martin Nederland/Marned B.V.Vissersstraat 9a1271 VE HuizenP.O. Box 2781270 AG HuizenThe NetherlandsTel. +31 35 523 45 38Fax +31 35 523 53 [email protected]
Nippon Martin K.K.6 Fl., 4-6-16 Hiranomachi541-0046 Chuo-ku,Osaka 541-0046JapanTel. +81 6 62 28 9075Fax +81 6 62 28 [email protected]
Orthosurgical Implants Inc. 12244 SW 130 Street Miami, Fl 33186USAOffice phone +1 305 969 45 45Office fax +1 305 969 45 46Toll free +1 888 305 45 [email protected] www.orthosurgical.com
KLS Martin L.P.11239-1 St. John`s Industrial Parkway SouthJacksonville, Fl 32246USAOffice phone +1 904 641 7746Office fax +1 904 641 7378Toll free +1 800 625 [email protected] www.klsmartinusa.com


















