
| CE article | review | industry report
44
roots international magazine of endodontology 2 2014 issn 2193-4673 Vol. 10 • Issue 2/2014 | CE article Passive micro-volume management of sodium hypochlorite in endodontic treatment | review Instrument fracture removal revisited | industry report BT-Race: Biological and conservative root canal instrumentation with the final restoration in mind
Transcript of | CE article | review | industry report

rootsinternational magazine ofendodontology2
2014
i s sn 2193-4673 Vol. 10 • Issue 2/2014
| CE articlePassive micro-volumemanagement of sodium hypochloritein endodontic treatment
| reviewInstrument fracture removal revisited
| industry reportBT-Race: Biological and conservativeroot canal instrumentation with thefinal restoration in mind

Dental Tribune InternationalThe World’s Largest News and Educational Network in Dentistrywww.dental-tribune.com
DTMediamix_A4_engl_2014.pdf 1DTMediamix_A4_engl_2014.pdf 1 22.01.14 11:2422.01.14 11:24

I 03
editorial _ roots I
roots2_2014
_Mahatma Gandhi once said, “Live as if you were to die tomorrow; learn as if you were to live for-ever.” Learning, thus, is a never-ending process, more so in dentistry and particularly in endodontics.In this present era, knowledge is just a click away; however, the authenticity of such information is notalways reliable. Literature plays a vital role in the shaping of a dentist into a concept-driven clinician.Apart from textbooks and journals, various educational forums where knowledge and clinical skills are shared without barriers contribute to the field of dentistry. One such online forum is Roots, whichhas been passionately educating and motivating young general dentists and endodontists. It has welcomed all those who have a passion for endodontics into its fold.
The majority of the advancements in endodontics are technology driven. Complete dependence ongadgets, however, without application of basic concepts makes us technicians, not endodontists. Thesetools can only be useful adjuncts to good theoretical knowledge and clinical skills. What better placeto obtain the best of both, the latest in technological advancements and the training to use them toenhance your concept-driven clinical acumen, than dental meetings? Roots Summits have been heldin various parts of the world. The last one was held at Foz do Iguaçu in Brazil in 2012. This year’s RootsSummit will be held in Asia for the first time, in Mahabalipuram, a peaceful beach town near the south-ern city of Chennai in India. The organising committee has been working tirelessly to make this sum-mit a memorable one. An array of national and international speakers are working on presentations,including the complexities of the root canal, the management of separated instruments, and regener-ative endodontics, which are critical areas in today’s clinical scenario in endodontics. To add to this,there are more than a dozen pre-summit workshops to choose from for those who wish to gain first-hand experience. This will be a golden opportunity for all dentists from Asian countries and from far tomeet in India to further enhance their knowledge and skills in a positive way. To learn more about thetechnological advancements, there is no better place than the summit, where there will be a plethoraof dental companies showcasing the latest in the field of endodontics.
rootsmagazine has always been known for its superior quality, in its articles, illustrations and print.This issue too covers topics that will offer insights on instrument retrieval, pre-endodontic restora-tions, conservative root canal instrumentation and phototherapy, among others.
I wish to sign off with an invitation to every reader and member of the Roots community to attendRoots Summit 2014 and contribute to its success.
Yours faithfully,
Dr Sekar MahalaxmiHead of the Department of Conservative Dentistry and EndodonticsSRM University, College of Dentistry, Chennai, India
Dr Sekar Mahalaxmi
Dear Reader,

I editorial
03 Dear Reader| Dr Sekar Mahalaxmi
I CE article
06 Passive micro-volume management ofsodium hypochlorite in endodontic treatment| Dr Les Kalman
I review
10 Instrument fracture removal revisited| Drs Dominique Martin & Pierre Machtou
I industry report
20 BT-Race: Biological and conservative root canal instrumentation with the final restoration in mind| Drs Gilberto Debelian & Martin Trope
I case report
24 Managing coronal destruction| Dr Andreas Schult
I feature
28 Root canal therapy setting your teeth on edge?| Dr Peter Southerden
I research
30 Diclofenac, dexamethasone or laser phototherapy? Part I| Jan Tunér
I industry news
34 SIROLaser Factbook: Comprehensive information ondiode lasers| Sirona Dental
36 Planmeca and the University of Turku found Nordic Institute of Dental Education| Planmeca
I events
38 “Striving for perfection”— AAE holds 2014 Annual Session in Washington| AAE
40 International Events
I about the publisher
41 | submission guidelines42 | imprint
I content _ roots
page 24 page 36 page 38
page 6 page 10 page 20
Cover image: first mandibular premolar anatomical variation
by Ronald Ordinola Zapata
04 I roots2_2014

DDS_A3_2014.pdf 1DDS_A3_2014.pdf 1 20.03.14 15:2320.03.14 15:23

06 I
I CE article _ irrigation
_Abstract
The passive utilization and micro-volume man-agement of sodium hypochlorite as an endodontic irrigant has been illustrated with a laboratory demon-stration and several clinical cases. By limiting the vol-ume and pressure of sodium hypochlorite, the injuri-ous effects can be minimized while still benefitingfrom the ideal disinfecting characteristics. Furtherstudies are required to understand the behaviour of fluids, especially sodium hypochlorite, within thecontext of permeability, fluid mechanics and multi-phase fluid flow through porous media.
_Introduction
Endodontic treatment addresses the removal ofthe tooth’s internal pulp and micro-organisms,1
primarily due to infection and necrosis. Once properdiagnosis and prognosis has been established, thepatient has the option of maintaining the tooth’sform and function while the vitality becomes lost.Current endodontic treatment consists of utilizingrotary files to remove the pulpal tissue and shapethe internal dentin chamber of the tooth. Chemicals,in the form of gels and liquids, are then implementedto disinfect the canal(s) and eliminate bacteria.2 Thechemicals are then dried and the canal space filledwith either gutta-percha or resin to create a her-metic seal.
The chemicals employed to clean and disinfectthe intracanal space are vast and include file lubri-cants such as Prolube (DENTSPLY) and irrigants suchas QMix (DENTSPLY). During clinical endodontics, thecanal is filled with a cocktail of chemicals, as file lu-bricants and irrigants become a mixture.
Fig. 1_DENTSPLY Vortex rotary file
with sodium hypochlorite.
Fig. 2_ DENTSPLY Profile rotary file
with dyed sodium hypochlorite.
roots2_2014
Passive micro-volume manage-ment of sodium hypochlorite inendo dontic treatmentAuthor_ Dr Les Kalman, USA
This article qualifies for CE credit. To take the CE quiz, log on to
www.dtstudyclub.com. Click on ‘CE articles’ and search for this
edition of the magazine. If you are not registered with the site,
you will be asked to do so before taking the quiz. You may also
access the quiz by using the QR code.
_ce credit roots
Fig. 1 Fig. 2

I 07
CE article _ irrigation I
roots2_2014
Chlorhexidine gluconate (CHX) is an uncommonlyused irrigant3 with several desirable properties. Itprovides antimicrobial activity against certain aero-bic and anaerobic bacteria, exhibits no significantchanges in bacterial resistance in the oral microbialenvironment and has no injurious effect to the skin ormucosa4. In fact, CHX has a role as an oral rinse at the0.12 per cent concentration.4
Sodium hypochlorite (NaOCl) still remains themost commonly used chemical,2,3 due to its avail-ability, cost and effectiveness.2,5 Sodium hypochloriteis effective against broad-spectrum bacteria and hasthe ability to dissolve both vital and necrotic tissue.6
However, this irrigant is equally damaging to the pa-tient and has a history of injurious effects.5 Typicallythe NaOCl is delivered into the canal space with a sy-ringe dose of 2–10ml that is expelled under pressure.The ability of NaOCl to escape either through poorlysealed isolation or other means can cause seriousinjury to the patient.5
Injury from NaOCl is well established in the litera-ture3,5,6 and has been attributed to three main errors:poor handling, injection beyond the apical foramenand allergy.6 Poor handling injury can result in opera-tor and/or patient injury to the eye and/or skin.6 In-jection beyond the apical foramen can result in thefollowing:6
_immediate and severe pain,_edema to adjacent tissue edema,_edema to the lip, infraorbital region, and side of face,_intense bleeding from within the canal space,_skin and mucosa bleeding,_intestinal bleeding,_paraesthesia,_secondary infection.
Allergy from NaOCl is rare but has been reportedand may result in severe pain, a burning sensation,edema and transient paraesthesia.6
_Methodology
Although there is no universally accepted irriga-tion protocol regarding endodontic treatment,3 it isthe duty of the clinician to apply evidence-based den-tistry within clinical parameters to provide their pa-tients with the highest standard of care with minimalmorbidity. The use of NaOCl has numerous beneficialfactors that maximize treatment success; however, it is the application of the liquid that can cause injury.
Micro-volume management of NaOCl has beenproposed. The concept is based on the premise thatendodontic instruments have irregular surfaces, cru-cial for dentinal preparation, and that liquids exhibitsurface tension characteristics.7 By placing an instru-ment into a suitable container, the NaOCl will becarried within the surface texture of the instrument(Figs. 1 & 2). As the operator inserts the instrumentinto the canal (Fig. 3), the NaOCl is carried with it.Upon instrument movement, the NaOCl is releasedinto the canal space (Fig. 4). Surface tension and per-meability of porous media (dentin) will also increasethe ability of the liquid to percolate into the canal.7
This approach is radically different than currentphilosophies, as the NaOCl is introduced into thecanal space in a micro-volume amount without anypressure. The operator has control of the minimizedliquid while benefitting from its effectiveness.
The micro-volume management of sodium hypo -chlorite has been applied to numerous clinical cases.Post-operative obturation radiographs of completedclinical cases have been presented (Figs. 5–9).
Fig. 3_Micro-volume delivery of
sodium hypochlorite with rotary file.
Fig. 4_Sodium hypochlorite in block
with rotary file.
Fig. 3 Fig. 4

08 I
I CE article _ irrigation
_Discussion
The canal system inside a tooth is very complex.Although there is the presence of one or more canals,there also exist numerous micro tunnels, ribbons andsheets throughout the canal network.8 The canals arealso housed within a porous dentinal structure, forwhich the permeability has been distinguished.9 Al-though the elimination of the pulp is a relatively pre-dictable clinical procedure, the introduction of liquidsinto this complex micro-network porous develop-ment further complicates matters. If the clinician in-troduces liquids, then the successful removal of thoseliquids is key to clinical success. Concepts of multi-phase fluid flow through porous media and capillar-ies,10 permeability of porous media11 and surface ten-sion fluid mechanics7 must be recognized to validateand further advance canal irrigation.
Micro-volume management of NaOCl has beensuggested as a delivery modality to maximize its bac-tericidal effects yet minimizing its injurious effects.
Surface tension fluid mechanics and permeability7,10,11
suggest that the NaOCl can be carried within thesurface irregularities of endodontic instrumentationand deposited into the canal space and percolatewithin the complex network of the canal. The passivemanagement of the irrigant in micro-volume wouldgreatly reduce complications due to poor handling.CHX has been suggested as the larger volume, posi-tive pressure irrigant that may be delivered into thecanal space. CHX has favourable antibacterial char-acteristics but minimal injurious effects, if misman-agement of the irrigant has occurred. If positive pres-sure delivery of CHX is required, the operator shouldregulate the pressure and avoid the risk of injectionbeyond the apex. The use of EDTA (ethylenediamine -tetraacetic acid) could be employed after NaOCl, tominimize the formation of precipitates.2
The application of micro-volume management ofNaOCl suggests that the canal space can be effectivelycleaned in a conservative manner. Application of thisprinciple has been applied to clinical cases with little
Fig. 5_Radiograph of endodontic
treatment on tooth #47.
Fig. 6_Radiograph of endodontic
treatment on tooth #26.
Fig. 7_Radiograph of endodontic
treatment on tooth #16.
Fig. 8_Radiograph of endodontic
treatment on tooth #36.
roots2_2014
Fig. 5 Fig. 6
Fig. 7 Fig. 8

I 09
CE article _ irrigation I
roots2_2014
to no post-endodontic sensitivity. Obturation hasbeen completed with ThermaSeal and Thermafil(DENTSPLY). Even though there is evidence of sealerextrusion, the absence of post-operative symptomsand pathology suggests adequate volume for suffi-cient disinfection.
Further laboratory studies are required to under-stand permeability, fluid mechanics and multiphasefluid flow through porous media and their relation tothe micro-management of NaOCl. Additional clinicalinvestigations should be implemented to assess andvalidate the efficiency and efficacy of micro-volumemanagement of sodium hypochlorite on endodontictherapy.
_Conclusions
Introduction of lubricants and irrigants into thecanal complex is crucial for endodontic success. Theaction of fluids in the canal complex must be under-stood within the context of permeability, fluid me-chanics and multiphase fluid flow through porousmedia.
NaOCl has several advantages for its role as anendodontic irrigant, but its use must be exercisedwith caution in order to prevent injury. Applicationof NaOCl as a passive, micro-volume liquid has beenillustrated.
Further consideration is required to validate thetheory. The potential to minimize morbidity whilemaximizing clinical endodontic success seems prom-ising for both clinician and patient._
_References
1. Dang E. Comparison of sodium hypochlorite and chlorhexidine
gluconate: quality of current evidence. The Journal of Young
Investigators: An Undergraduate, Peer-Reviewed Science
Journal 2008:23(1):1–9.
2. Basrani BR, Manek S, Rana SNS, Fillery E. and Manzur A.
Interaction between sodium hypochlorite and chlorhexidine
gluconate. J Endod 2007;33: 966–969.
3. Dutner J, Mines P, and Anderson A. Irrigation trends among
American Association of Endodontists members: a web-based
survey. J Endod: 2011: 1–4.
4. 3M ESPE: Peridex™ Chlorhexidine Gluconate (0.12%) Oral
Rinse Fact Sheet: 2009.
5. Clarkson RM, and Moule AJ. Sodium hypochlorite and its
use as an endodontic irrigant. Australian Dental Journal
1998;43:(4):250–6.
6. Hülsmann H. & Hahn W. Complications during root canal
irrigation-literature review and case reports. International
Endodontic Journal: 2000;33:186–193.
7. Trefethen L. Surface tension in fluid mechanics. Encyclopae-
dia Britannica. (12ed.) Wiley:Chicago,1969;1–7.
8. West JD, Roane JB and Goering AC. Cleaning & shaping of the
root canal system. In Cohen S. and Burns RC. Pathways of the
Pulp. (6th ed.) Mosby: St. Louis,1994;179–218.
9. Trowbridge HO. and Kim S. Pulp development, structure &
function. In Cohen S. and Burns RC. Pathways of the Pulp. (6th
ed.) Mosby:St. Louis,1994;296–336.
10. Templeton CC. and Rushing SS. Jr. Oil-water displacements in
microscopic capillaries. Journal of Petroleum Technology.
1956;8:(9):211–214.
11. Crotti MA. Motion of Fluids in Oil and Gas Reservoirs.
Mosby:New York,1978;8–14.
Fig. 9_Radiograph of endodontic
treatment on tooth #16.
Dr Les Kalman, B.Sc. (Hon), DDS, graduated from the
University of Western Ontario with a doctor of dental surgery
degree in 1999. He then completed a GPR at the London
Health Sciences Centre. He has been involved in general
dentistry within private practice since 2000. He has served
as the chief of dentistry at the Strathroy-Middlesex General
hospital. In 2011, he transitioned to full-time academics as
an assistant professor at the Schulich School of Medicine and
Dentistry. Kalman’s research focuses on clinical innovations,
including the Virtual Facebow app. Kalman is also the director of the Dental Outreach
Community Services (DOCS) program, which provides free dentistry within the com-
munity. Kalman has authored articles ranging from paediatric impression to immedi-
ate implant surgery in both Canadian and American journals. He has been a product
evaluator for several companies, including GC America and Clinician’s Choice.
Kalman is the co-owner of Research Driven, a company that deals with intellectual
property development. Kalman is a member of the American Society for Forensic
Odontology, International Team for Implantology, Academy of Osseointegration,
American Academy of Implant Dentistry and the International Congress of Oral
Implantology. He has been recognized as an Academic Associate Fellow (AAID)
and Diplomate (ICOI). In his spare time, Kalman enjoys photography as an accredited
MotoGP photojournalist. He can be contacted at [email protected]
_about the author roots
Fig. 9

10 I
I review _ instrument fracture removal
_Introduction
The fracture of a root canal instrument during endodontic treatment is quite a common occurrence.The estimated risk of instrument fracture is between0.5 and 5per cent.1–6 It has been shown that the num-ber of instrument fractures has notably increasedwith the growing use of rotary instruments made ofnickel titanium (NiTi).2,4
Procedures to remove instrument fragments havebeen used for many years, but the introduction of op-eratory microscopes to clinical practice has led to acompletely new approach. The possibility of actuallyseeing the instrument allows a far more effective pro-cedure, which is further helped by the development ofinstruments specially designed for this purpose. Thesetechniques are now well documented, and studiesevaluating the possibilities of removing instrumentfragments have shown encouraging results.7–10 Themost common technique entails preparing straight-line access to the coronal part of the fragment usingGates Glidden drills, creating a staging platform witha modified Gates Glidden drill, and then using thin ultrasonic tips to retrieve the fragment from the canalwalls through ultrasonic vibration.11
Although this technique is very effective, it hassome disadvantages:
_It requires great skill from the operator, since theprocedure is done under high magnification. In ad-dition, it is difficult to trough around the fragmentwithout touching it. Especially in the case of an NiTibroken instrument, the fragment may fracture dur-ing the course of treatment if the ultrasonic tipcontacts the instrument too early or if not enoughspace is available around it.12
_Often, too much radicular dentine structure is re-moved, which is likely to weaken the root.13
_In order to improve visual control, the treatment is carried out without irrigation, potentially leadingto an increase in temperature of the periodontal tissue.14, 15 Work therefore must be interrupted reg-ularly to control heating and provide cooling.
_The procedure is fairly time consuming. The esti-mated time required for the treatment was shown tobe between 40 and 55 minutes.16
An alternative method is to remove the fragmentwith the micro-tube technique. Several variationsof this technique have been described, includingthe Masserann Micro Kit (MICRO-MEGA),17 the IRS(DENTSPLY Maillefer),18 and a micro-tube coupledwith a Hedstroem file.9 The use of tubes and cyano-acrylate glue (Cancellier Kit, SybronEndo) or com-posite self-curing resin19 are other methods to re-trieve the fragment.
The present technique is a combination of thetrephine drill technique using a new device, the EndoRescue Kit (Komet Dental), and the micro-tube tech-nique using dedicated needles and composite self-curing resin. The main goal of this technique is to bethe least destructive as possible for the tooth struc-ture. The aim of the present study was to assess thesuccess rate of this micro-endodontic removal tech-nique and compare the results with those of pub-lished studies.
Fig. 1_The Endo Rescue Kit (Komet).
roots2_2014
Instrument fractureremoval revisitedAuthors_ Drs Dominique Martin & Pierre Machtou, France
Fig. 1

I 11
review _ instrument fracture removal I
roots2_2014
_Materials and methods
This clinical endodontic studywas conducted in a specialist endo -dontic practice by one operator. Theinclusion criterion was a fractured in-strument located in a tooth referredfor endodontic retreatment. The casewas either specifically referred for in-strument removal or a fracture oc-curred during endodontic treatmentin the operator’s practice. The exclu-sion criterion related to the possibilityof safely accessing the fragment. When itwas not possible to create straight-line ac-cess to the coronal part of the fragment or whensuch access would have been too destructive to thetooth structure, the case was excluded from the studyand removal of the fragment not attempted. All caseswere treated according to the same procedure usingthe Endo Rescue Kit following the Masserann’s basicapproach, which involves removal of dentine aroundthe fragment with trephine drills. However, this newkit differs from the Masserann Micro Kit.20 The first in-strument is a special centring drill featuring a concaveactive surface (Fig. 1) whose diameter matches pre-cisely the size of the corresponding trephine (Fig. 2).The centring drill prepares the site for the subsequentuse of the trephine. Three trephine sizes are available.The smallest trephine has an external diameter of0.7mm (corresponding to a #2 Gates Glidden drill), thesize of the next one is 0.9mm (corresponding to a #3 Gates Glidden drill) and the last one is 1.1mm (cor-responding to a #4 Gates Glidden drill).
The following steps were followed in a strict se-quence:
1. Similar to the currently used techniques, straight-line access to the coronal portion of the fractured instrument has to be created. The goal of this step isto visualise the fractured instrument under the op-
erating microscope. A cylindro-conicalbur with a non-cutting tip (KometDental) was used to refine the accesscavity walls, followed by the use of ashort #4 Gates Glidden drill (KometDental) to relocate the canal orificeaway from the furcation. Direct ac-cess to the fragment was then created
with a #2, 3 or 4 Gates Glidden drill, de-pending on the diameter of the coronal part of thefragment and its location within the canal.
2. The centring drill, whose external diametermatches precisely the size of the previously usedGates Glidden drill, removes dentine around thefragment. Its concave active surface, when com-ing into contact with the fragment, allowed goodcentring of the preparation around the coronalpart of the fragment.
3. The corresponding trephine was placed in the areapreviously prepared with the centring drill to freethe fragment by removing the surrounding den-tine. The trephine was used in a handpiece at a lowspeed (300rpm) in an anti-clockwise rotation or byhand (Figs. 1 & 3).
4. When the fragment could not be removed with thetrephine alone, the Endo Rescue Kit was used incombination with a needle filled with a self-curingcomposite. A needle (Ultradent) with the same ex-ternal diameter as the trephine was filled with a self-curing composite core material and placed on to thefree portion of the fragment. Once the compositehad set, the needle was removed with an anti-clock-wise motion (Fig. 2). A radiograph was taken to con-firm that the instrument had been successfully re-moved. Complete removal of the fragment withoutcreating a perforation was defined as a success.
The distribution of fractured instruments amongdifferent root types (i.e. anterior teeth, premolars,buccal roots of maxillary molars, mesial roots ofmandibular molars, distal roots of mandibular molars,and palatal roots of maxillary molars) was recorded,as well as the anatomical location of the fractured in-struments (i.e. coronal part of the fragment in thecoronal third, middle third or apical third).
Fig. 2_Centring drill.
Fig. 3_Trephine.
Table 1_Success rate depending on
the type of tooth.
Fig. 4_Different sizes of centring
drill and trephine: the smallest has
an external diameter of 0.7mm
(corresponding to a #2 Gates Glidden
drill), the size of the next one is
0.9mm (corresponding to a #3 Gates
Glidden drill) and the last one is
1.1mm (corresponding to a #4 Gates
Glidden drill).
Incisors 1 1 0 100
Upper premolar 6 6 0 100
Lower premolar 0 0 0 0
Upper molar buccal root 8 7 3 70
Upper molar palatal root 1 1 0 100
Lower molar mesial root 13 11 4 73
Lower molar distal root 3 3 0 100
Teeth n Removed Not removed Success (%)
Fig. 2
Fig. 3
Fig. 4

12 I
I review _ instrument fracture removal
_Results
Success or failure rate
According to the inclusion criterion, 36 fragmentswere recorded within the 18-month period, involving32 teeth in 30 patients. Five instruments were ex-cluded because straight-line access to the fragmentwas deemed impossible. Therefore, no attempt wasmade to use the described technique. Thus, the tech-nique was used for 31 instruments, 29 of which wereremoved successfully. Of those, 19 were removed withthe trephine alone and ten with a needle filled withcomposite resin (Table 1). This resulted in a success rateof 93.5%. Two instruments (6.5%) further fracturedon attempted removal, leaving the most apical part inthe canal. No perforation of the root walls was noted.
Type of tooth and root
There were 24 instrument fragments found in 21molar teeth (75% of the sample). There were six pre-molars with six fragments (accounting for 21.4% ofthe teeth) and one incisor with one fragment (ac-counting for 3.6% of the teeth).
The two failures occurred in a mesial root of a mo-lar, one in a mesial root of a mandibular molar and onein a mesiobuccal root of a maxillary molar (Table 2).
Location of fragments in root canal
It is important to note that it was the location ofthe coronal part of the fragment that was recorded.All instruments that had fractured in the coronalthird (n = 5) were removed from the root canal. Allremoval failures (n = 2) occurred in situations inwhich only the head of the fragment was visible butthe main portion of the fragment was located be-yond a sharp curvature. In these two cases, the in-strument fractured again, leaving the most apicalpart in the canal.
Table 2_Success rate depending on
the level of the fragment.
Case 1: Fragment removal with the
ø 90 Endo Rescue Kit.
Fig. 5a_Pre-operative X-ray of tooth
#26 showing a fractured instrument
located in the middle part of a MB
curved root canal.
Fig. 5b_Trephine size 90
surrounding the fragment.
Figs. 5c–d_Fragment locked
inside the trephine and removed
from the canal.
Fig. 5e_Final X-ray.
roots2_2014
Coronal third 5 5 0 100
Middle third 18 16 2 89
Apical third 8 8 5 61
Position n Removed Not removed Success (%)
Fig. 5a
Fig. 5c Fig. 5eFig. 5d
Fig. 5b

I 13
review _ instrument fracture removal I
roots2_2014
_Discussion
Success rate
The present study is a prospective evaluation ofcases referred to a specialist practice and treated under a dental operating microscope. The success rateof removal of the fractured instruments with the described technique was 93.5%.
A variety of different techniques and devices for removal of fractured instruments have been de-scribed in the endodontic literature.15 The majority ofthese publications involve descriptions of techniquesand case reports. To date, there have been only twodetailed investigations on the influence of differentfactors regarding success or failure of removal at-tempts using micro-endodontic techniques and adental operating microscope. In these two studies, thesuccess rate for the removal of fractured instrumentswas reported to be 87%9 and 95%,10 respectively. InSuter’s study, various techniques were used to removethe fragments. In Cujé’s study, the same procedurewas applied using ultrasonic files in all cases. The lossof dentine was not mentioned in either study. In thepresent study, taking into account the cases for whichno attempt at removal was made, the overall successrate was 80.5% and compared favourably withSuter’s study. For the 31 cases treated, the success ratewas similar to Cujé’s study. In the current protocol, thefocus was on the preservation of the tooth structure.
Decision-making
The general principle for removing a fractured in-strument is based on the fundamental principles andobjectives of root canal treatment. A fractured in-strument may be an obstacle to mechanical andchemical treatment of an infected root canal system.Bacteria and pulp tissue remaining in the root canalbecause of insufficient cleaning may have a negativeimpact on the treatment outcome.21 Moreover, theprognosis is likely to depend on the stage and degreeof canal preparation and disinfection at the time ofinstrument fracture and, therefore, on the extent towhich microbial control has been achieved.1, 2 The riskfactors associated with the presence of a fragmentare not clear. Recently, a systematic review and meta-analysis were performed to determine the outcomedifference between retained fractured instrumentcases and matched conventionally treated cases. Twocase–control studies were identified, covering 199cases. The risk difference of the combined data indi-cated that a retained fragment did not significantlyinfluence healing.22 The presence or absence of a pre-operative periradicular disease has been reported tobe the main predictive factor for outcome in suchcases.2,23 The risk–benefit ratio of the two therapeuticoptions, that is, either leaving the fragment in situ andcompleting the treatment by filling the accessibleparts of the canal, or trying to remove the fragmentso that the entire canal can be treated, should be care-fully assessed for each case.
Case 2: Fragment removal with the
ø 70 Endo Rescue Kit trephine.
Fig. 6a_Pre-operative X-ray of tooth
#25, featuring a long and narrow root
with a very thin fragment fractured at
the junction between the middle and
the apical third of the root.
Fig. 6b_Trephine size 70 surrounding
the fragment.
Fig. 6c_The fragment is removed
with the trephine, shaping and filling
are achieved.
Fig. 6d_Final X-ray showing a
minimally invasive procedure.
Fig. 6a Fig. 6b
Fig. 6c Fig. 6d

14 I
I review _ instrument fracture removal
Instrument removal itself represents a risk andthe decision to remove, or not to remove, a fragmentis a difficult one. Depending on the technique used,perforation of the root, ledge formation and trans-portation of the original canal may occur, as well asweakening of the affected root in case of excessiveremoval of dentine13 or fracture of an additional in-strument.8,9,23–25 Therefore, when no lesion is present,current knowledge leads us not to attempt a risky pro-cedure to remove the fragment. In this study, fivefragments were deeply fractured and not accessiblewith straight-line access. According to the previousrationale, no attempt was made to remove these frag-ments, since no apical lesion was present (Fig. 4). Twoof these fragments were bypassed and the endodon-tic treatment completed.
NiTi fractured instruments
The fracture of rotary NiTi instruments is charac-terised by certain distinctive features. The first char-acteristic is that, owing to the rotary movement ofthe instrument and penetration of the flutes intothe walls, the fragment is most frequently blockedin the dentine.23 The second characteristic of thesefractures is related to the instrument design. Mostrotary NiTi instruments have a taper greater than2%. Owing to this increased taper, the coronal partof the fragment is likely to be blocked in the canal,whereas the apical portion remains free. This partic-ular feature of NiTi instruments complicates the pri-mary procedure of removing the fragment, whichnormally entails passing an endodontic hand in-strument between the fragment and the canal walls,and guiding it along the fragment to regain patencyof the canal. In this case, a more invasive solution isrequired. This involves straightening the coronalcurve to gain access to the fragment at the expenseof the dentinal walls. Such techniques are still verycontroversial.
A frequent counter-argument is the fact that the root canal is weakened by the removal of dentineduring the procedure.26,27 This loss of tissue reducesthe fracture resistance of the root13,28,29 and may leadto complications, such as inadvertent perforation ofthe root.8 Ideally, the dentine should be preserved asmuch as possible and the extent of the root canalpreparation after the removal of the fragment shouldnot exceed that of a conventional preparation. Thetested technique is intended to overcome this limita-tion. Although the use of the Endo Rescue Kit involvesthe removal of an additional amount of dentine, thesmall diameter of the instruments keeps the damageto the root structure to a minimum, while creating access to the fragment.
Case 3: Fragment removal with
a needle and composite resin.
Fig. 7a_Pre-operative X-ray of tooth
#16. A fractured instrument is
located in the middle part of the
MB2 canal.
Figs. 7b & c_Relocation of the canal
orifice and centring of the preparation
after the pointer drill use.
Fig. 7d_The coronal portion of the
fragment is freed after the work of
the trephine.
Figs. 7e–h_The needle technique
with composite resin inside the lumen
is used to remove the fragment.
Figs. 7i_Final view of the
completed case.
roots2_2014
Fig. 7a Fig. 7b
Fig. 7c Fig. 7d
Fig. 7e Fig. 7f Fig. 7g

review _ instrument fracture removal I
Access to the fragment
As with all the techniques described, the decisivefactor for success was to gain direct access to thefragment. Given that the fragment is usually locatedbeyond the curve of the canal, it is essential tostraighten the coronal curve in order to create directaccess to the fragment and ensure an unobstructedview of it through the operative microscope. It isequally necessary to expose at least 1.5mm of thefragment with a trephine in order to be able to catchthe fragment with a needle filled with composite
resin. A dilemma exists in such situations because it has not been clearly shown that a retained frag-ment has any impact on the prognosis,2 but there is some evidence that removing tooth structureweakens the tooth. It must be carefully evaluatedand critically analysed to determine whether a re-moval attempt is necessary or indicated in each clin-ical case.23 In this study, after the preparation of thecoronal access and when no periapical lesion waspresent, it was decided not to attempt to remove thefragment, as it was not visible under the operatingmicroscope.
Biological &Conservative
FKG Dentaire SAwww.fkg.ch
AD
Fig. 7h Fig. 7i

16 I
I review _ instrument fracture removal
The second step was to prepare a staging plat-form around the fragment. By investigating differenttechniques for preparation of a staging platform,Iqbal et al. found it was increasingly difficult to pre-pare a platform with a centred fragment owing to theincreasing distance between the fractured instru-ment and the maximum curvature of the root canal.4
The modified Gates Glidden drill described in Ruddle’stechnique is a helpful instrument for preparing thestaging platform but it does not allow centring ofthe fragment.
The design of the centring drill in the Endo RescueKit follows the same concept but was modified tohave a tapered concave active portion. The outerblades cut into the dentine surrounding the fragment,and the concave tapered area that encounters thecoronal part of the fragment allows centring of thepreparation by advancing the drill apically. This can becarried out by removing a minimum amount of den-tine according to the size of the drill, while working inthe centre of the canal (Fig. 8).
The micro-tube technique
The first device to use micro-tubes was theMasserann Micro Kit. This well-known kit is designedto remove all metallic objects from the root canal andconsists of a variety of trephines of different sizes andan extractor to grasp the fragment and remove it.17
The extraction method is easier to use than the ultra-sonic technique, but it has some disadvantages aswell. The trephines are too large compared with thesize of the fragments that are usually found in theroot canal. The smallest available diameter is 1.1mm,whereas the diameter of the extractor is 1.2mm, whichmeans that it has to be used with a trephine of thesame diameter. Depending on the position of the frag-ment in the root, a large quantity of dentine mighthave to be removed, which is likely to weaken the root.
Some improvement to the Masserann’s extractorwas made with the introduction of the IRS. However,in the described technique,18 access to the fragmentwas accomplished with ultrasonic tips. The use of ultrasonic tips to disengage the fragment results in an over-enlarged access compared with the size ofthe IRS extractor. This reduces the interest to usesmaller extractors, which are fragile and may deform.
Compared with the Masserann Micro Kit, theEndo Rescue Kit has a number of special features. The first feature is a centring drill with the same di-ameter as the trephine. Owing to its active concavetip, the outer blades trough around the fragment,and allow centring of the preparation. The secondfeature is the miniaturisation of the trephines. Threetrephines are available: the smallest trephine has an external diameter of 0.7mm (internal diameter of 0.4mm), the size of the next one is 0.9 mm (inter-nal diameter of 0.5mm), and the last one is 1.1mm(internal diameter of 0.7mm). Compared with theMasserann’s trephines, the sizes are considerablysmaller. The largest size trephine drill in the EndoRescue Kit corresponds to the smallest size in theMasserann Micro Kit. The trephines are designed tobe used with an anti-clockwise motion in order tohave an unscrewing effect on the fragment. This fea-ture is particularly useful for NiTi rotary fragments,which are usually screwed into the dentine. Whenthe fragment is short (less than 3mm), it is oftenpulled out of the canal with the trephine drill. In thisinstance, it is trapped by the dentinal chips inside thelumen of the trephine. When the fragment is longerthan 3mm or when the tip is located beyond the cur-vature, the action of the trephine should be stoppedbefore grinding the fragment with the active part of the trephine. The direction of rotation must beconsidered too, depending on the type of fracturedinstrument. Rotary instruments used for obturation,such as Lentulo spirals or McSpadden compactors,
Case 4: No removal attempt.
Figs. 8a & b_Fragment located
apically beyond the canal curvature
of tooth # 26 without radiographic
signs.
roots2_2014
Fig. 8a Fig. 8b

P R O F E S S I O N A L M E D I C A L C O U T U R E
E X P E R I E N C E O U R E N T I R E C O L L E C T I O N O N L I N E
WWW.CROIXTURE.COM
Croixture_A4_2013.pdf 1Croixture_A4_2013.pdf 1 04.07.14 11:2104.07.14 11:21

or shaping instruments that work in a reciprocatingmotion, should be disengaged with a clockwise mo-tion because their helix angle is reversed.
The micro-tube coupled with the Hedstroem filetechnique9 is another way to create an extractor thatis more adaptable to the clinical situation using dif-ferent size tubes and files.
Using tubes and glue is also advocated to graspthe fragment with cyanoacrylate glue (CancellierKit) or composite self-curing resin.19 Needles of dif-ferent diameters may be used to match the size ofthe broken instrument. This can only occur if thecoronal part of the fragment has been freed fromthe dentinal walls. This technique is predictable butthree problems have been reported. The first is that,to ensure that the cavity is clean and dry, the cavitymust be rinsed with pure alcohol and be perfectlydry before using the needle filled with compositeresin. The second is that the operator must ensurethat the needle is filled with resin in order to sur-round the fragment. The third is that the operatormust ensure that the resin does not overflow fromthe needle and remains inside the root canal. Theseproblems can be easily overcome however. The com-posite resin was injected into the needle. The hub ofthe needle was then plugged with wax until the resinemerged from the tip. The tip was wiped with gauzeto ensure that there was no resin on the outer wallsof the needle. In this way, the resin can surround thefragment without any overflow. In the study, thistechnique was performed using a needle of thesame diameter as the trephine for 12 of the 29 frag-ments. Ten of the 12 fragments were removed with-out leaving any composite resin to potentially blockthe root canal. Two failures occurred because thefragments were further fractured, leaving the mostapical part in the canal and the coronal part embed-ded in the resin.
_Conclusion
Several techniques for removing fractured in-struments have been described. Any procedure forremoving fractured instruments should seek to avoiddamage to the root structure, and should be pre-dictable. The removal technique investigated in thepresent study, based on the use of a micro-tube andpreparation of a staging platform by means of newcentring drills, was shown to be effective for the re-moval of fractured instruments. Although no tech-nique can claim to be universal, the technique de-scribed in the study proposes a removal solution wellsuited to fractured NiTi rotary instruments and offersan alternative to the ultrasonic tips technique. Likeany endodontic technique, the Endo Rescue Kit is atechnique-sensitive approach and requires clinicalexperience to be used successfully. However, thispreliminary study reported few cases and thereforefurther studies must be conducted to corroboratethese results. The location of the instrument withinthe root canal, the angle of curvature of the affectedroot and the location of the broken instrument in re-lation to the root curvature appear to be decisive fac-tors for the outcome of the removal technique._
Editorial note: A complete list of references is available
from the publisher.
Fig. 8c_Cleaning, shaping and filling
of the root canal system.
Fig. 8d_One year recall: tooth is
symptomless.
Dr Dominique Martin
21 rue Fabre d’Églantine
75012 Paris
France
_contact roots
Fig. 8dFig. 8c
18 I
I review _ instrument fracture removal
roots2_2014

6 Months Clinical Masters Programin Advanced Implant Aesthetics17 July 2014 to 22 November 2014, a total of 12 days of intensive live training
with the Masters in Como (IT), Barcelona (ES), Munich (DE)
Live surgery and hands-on with the masters in their own institutes plus online mentoring and on-demand learning at your own pace and location.
Tribune America LLC is the ADA CERP provider. ADA CERP is a service of the American Dental Association to assist dental professionals
in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors,
nor does it imply acceptance of credit hours by boards of dentistry.
Learn from the Masters of Advanced Implant Aesthetics:
Collaborate on your cases
and access hours of
premium video training
and live webinars
University of the Pacific
you will receive a
certificate from the
University of the Pacific
Latest iPad with courses
all registrants receive
an iPad preloaded with
premium dental courses
17 July 2014 to 22 November 2014a total of 12 days in Como (IT), Barcelona (ES), Munich (DE)
Curriculum fee: € 11,900
Registration information:
contact us at tel.: +49 341 48474 302
email: [email protected]
Details on www.TribuneCME.com
ADA CERPC.E. CREDITS100
TribuneCME_A4_advanced_allgemein_2014.pdf 1TribuneCME_A4_advanced_allgemein_2014.pdf 1 05.03.14 14:4305.03.14 14:43

20 I
I industry report _ instrumentation
_Intra-canal microbesare the cause of endodon-tic disease.1–3 The removal of microbes from the rootcanal system during treatment and the prevention ofmicrobes entering the canals determines whethertreatment will be successful.4,5
Root canal instrumentation is one of the majortools with which to ensure the long-term success ofroot canal therapy.6,7 The aim is to mechanically dis-rupt as much biofilm as possible so that, with the addition of irrigants and/or intra-canal medicaments,
a very low microbial count can consistently be achievedbefore root canal filling. Furthermore, the aim of rootcanal instrumentation is to achieve the microbial re-duction goals mentioned above without unnecessar-ily weakening the root by over-instrumentation, thatis, the reduction of the dentinal wall thickness. Preser-vation of native tooth structure, especially in the cer-vical region of the tooth, has been demonstrated tocorrespond to better long-term survivability from aloading and restorative standpoint. It is well estab-lished that the root decreases in its resistance to frac-ture as the remaining dentine thickness decreases.8
_What is the ideal root canal instrumentation size?
The file alone does not remove the maximumamount of biofilm but works in synergy with irriga-tion. What then is the ideal instrumentation size toachieve the desired goal of biofilm elimination? In order to answer this question, we need to analyseanatomical studies, and evaluate whether and how itis possible to remove biofilm from these canals.
Fig. 1_Median canal diameters.
Fig. 2_Benefits of BT-Race files.
roots2_2014
BT-Race: Biological and conservativeroot canal instrumentation with the final restoration in mindAuthors_ Dr Gilberto Debelian, Norway, & Dr Martin Trope, USA
Patented new screwing-in design
Triangular cross section
Electro-polished
Fig. 1
Fig. 2

I 21
industry report _ instrumentation I
roots2_2014
A review of anatomical studies demonstratesstriking consistency regarding instrumentation size.Figure 1 summarises the anatomical aims for amandibular molar. Consider the mesiobuccal andmesiolingual canals at the 1mm measurement fromthe apical foramen, which corresponds most closelyto the dentinocemental junction. In the mesiodistaldirection, the diameters are 0.21mm and 0.28mm, respectively. Thus, finishing at a #25 file would appearto be sufficient when viewed on a periapical radi-ograph, since the mesiodistal direction is what we seeon the radiograph. However, if we look in the bucco -lingual direction, the correct sizes are between #35and #40 files. For the distal canal, a #35 file would ap-pear adequate on the radiograph (mesiodistal view)but the correct size would be a #50 file. Thus, if wewant to clean in three dimensions, we need to instru-ment in the buccolingual dimension also.
Furthermore, if we look at the measurements at 2 and 5mm from the end of the root, it is apparent that a 0.04 taper is all that is needed to contact thewalls in these areas further from the apex if we do, infact, instrument to the apical sizes required (a #35 or40 file mesially and a #50 file distally). Using taperslarger than 0.04 is not required to remove microbesand unnecessarily weakens the root. Anatomicalstudies on all roots follow this basic biological rule,that is, size 35 or 40 for the smaller canals and size 50for the larger canals.9–11
_What is the ideal shape of an instrumented canal?
Adequate biological sizes with minimal taper withthe least number of files will ensure the ideal shape.Thus, in order to achieve the aims stated above, thatis, maximal biofilm disruption with minimal weaken-ing of the root, we should aim for apical sizes 35, 40or 50 with no more than a 0.04 taper.9–11 These bio-logical sizes with an adequate irrigation protocol willensure a consistently low microbial count for maxi-mal success.
_The BT-Race system, biological andconservative
BT-Race files (FKG Dentaire; Fig. 2) are sterilised in individual blisters so that sterility is ensured forevery file. The biological sizes mentioned above can beachieved every time with three files once a glide pathhas been achieved. The system is designed such thatthese sizes can be attained with minimal removal ofcoronal dentine to maintain the strength of the root.The files have a non-screw-in design and triangularcross-section to increase flexibility and cutting effi-ciency, and are electropolished to decrease the effectsof torsional and cyclic fatigue.
Booster Tip
The Booster Tip (BT) is the key feature of these filesand allows them to follow curvatures in canals with-out undue stress on the file or the root. The tip startsas a non-cutting tip from the 0.0–0.15mm file diam-eter, and the cutting edges start from the 0.15mmfile diameter and upwards. This allows these files tofollow a canal safely, even one with a very narrow di-ameter. Thus, the BT2 file (Figs. 3 & 4a–c), for example,which is a non-tapered file with a cutting size of0.35mm, can still easily advance into the canal pre-pared by the glide path file, which is 0.15mm in di-ameter.
Fig. 3_Localisation of the cutting
point in the BT and normal tips.
Figs. 4a–c_Efficiency of the normal
tip and the BT in the canal (a & b).
Path of the tip with guide (c).
BT tip
Normal tip
0.15 mm 0.35 mm
0.35 mm
BT ti
p
Norm
al ti
p
ISO 35 ISO 35
ISO 15 ISO 15
BT ti
p
Fig. 3
Fig. 4a Fig. 4b Fig. 4c

22 I
I industry report _ instrumentation
The BT allows a file of any diameter to follow theshape of a canal that has been prepared with a #15glide path stainless-steel file. However, the sequenceof three files (Fig. 5) is designed to relieve undue stresson the root and files, while instrumenting the canal tothe correct biological sizes.
_Essential aspects for the successful application of the BT-Race sequence
1. Glide path
In order to guarantee minimal file breakage, a 15.02glide path is essential. Hand files can usually achievethis aim. However, if a #6 or #10 file is extremely diffi-cult to take to working length, then ScoutRace files allow one to achieve a glide path more quickly.
2. Speed of 800–1,000 rpm
A high speed reduces the risk of breakage due totorsional fatigue. Since these files are for use with in-dividual patients only, the risk of breakage due to
cyclic fatigue is also reduced. Thus, by using a highspeed and limiting file use to one patient, we can limitthe risk of file breakage.
_BT-Race sequence
BT1 (a 10.06 file)
This file establishes the final glide path and deter-mines the coronal diameter. In any canal in which a15.02 glide path has been achieved, the file will con-tact mainly the coronal third of the canal. At 12mmfrom the working length, the diameter will be 0.82mm.These files have no BT, since the tip diameter is already0.10mm and smaller than the glide path establishedwith a 15.02 K-file.
BT2 (a parallel #35 file with a BT)
The BT2 file is used to prepare the apical third of the canal. The file is extremely flexible owing to itsnon-tapered design, yet penetrates into the narrowcanal easily and efficiently owing to the BT.
Fig. 5_BT-Race sequence.
Fig. 6_BT-Race XL for finishes at
sizes 40 and 50.
roots2_2014
BT 1 – 10/0.06 Scouting
BT 2 – 35/0.00 Apical
BT 3 – 35/0.04
BT 40 – 40/0.04
BT 50 – 50/0.04
Shaping
Fig. 5
Fig. 6

I 23
industry report _ instrumentation I
roots2_2014
BT3 (a 35.04 file with a BT)
This file is used to join the coronal and apical thirdsprepared with the BT1 and BT2 files, thus creating a35.04 final shape that allows maximal irrigation anda tight cone fit. The file is able to go to working lengthwith minimal stress, since the coronal third has beencleared with the BT1 file and the apical third with theBT2 file.
Importantly, the maximum diameter at the 12mmlevel in the canal is 0.83mm. Thus, the removal ofcoronal dentine is minimal, allowing for the strongestroot possible after restoration.
BT-Race XL: BT 40 (a 40.04 file) and BT 50 (a 50.04 file),
600–800 rpm
These two instruments (Fig. 6) enable finishes atISO #40 and 50 when larger adequate apical sizes arerequired. If apical preparations even larger than size50 are required, the Race range of instruments is recommended in the required sizes, preferably with asmall taper of 0.02.
_Conclusion
With this unique file system, all canals can be con-servatively instrumented to the correct biologicalsizes, while maintaining maximum cervical toothstructure. The BT ensures that the original canal shapeis maintained, thus keeping even the larger files cen-
tred in the canal. With this centring, in addition to theminimal taper required to achieve these biologicalsizes, the canal is maximally cleaned without weak-ening or stressing the root._
Editorial note: A complete list of references is available
from the publisher.
Figs. 7–10_Example cases. Note
that these cases fulfil the objective
of biological apical sizes with conser-
vative removal of coronal dentine.
Thus, they have a high probability of
endodontic success and survivability.
Dr Gilberto Debelian (Oslo, Norway)Dr Debelian received his DMD degree from the University of São Paulo, Brazil, in 1987. He completed his specialisation in Endodontics at the University of Pennsylvania, Philadelphia, USA,in 1991. He completed his PhD studies at the University of Oslo in1997. He is an adjunct visiting professor in the postgraduate pro-grammes in Endodontics at the University of North Carolina at
Chapel Hill and the University of Pennsylvania. Dr Debelian maintains a private specialist endodontics practice in Bekkestua, Norway.
Dr Martin Trope (Philadelphia, USA)Dr Trope received his BDS degree in dentistry from University in Jo-hannesburg, South Africa, in 1976. In 1980 he moved to Philadel-phia to specialize in Endodontics at the University of Pennsylvania.After graduating as an Endodontist he continued at the University of Pennsylvania as a faculty member until 1989 when he becameChair of Endodontology at Temple University, School of Dentistry.
Dr Trope is now Clinical Professor, Department of Endodontics, School of Dental Medi-cine, University of Pennsylvania. He is also in private practice in Philadelphia, USA.
_about the authors roots
BT RaceBiological treatment with Booster tip
SymptomaticPulpitis
36
MB and ML: BT3D: BT4
Obturation:Total Fill BC sealer
Courtesy: Dr. Johan Ulstad, Norway
BT RaceBiological treatment with Booster tip
SymptomaticPulpitis
MB and ML: BT3D: BT4
Obturation:Total Fill BC sealer
Courtesy: Dr. Gilberto Debelian, Norway
BT RaceBiological treatment with Booster tip
SymptomaticPulpitis tooth
16 and 17
MB1 and MB2: BT3DB: BT4P: BT5
Obturation:Total Fill BC sealer
Courtesy: Dr. Gilberto Debelian, Norway
BT RaceBiological treatment with Booster tip
SymptomaticPulpitis
16
MB1 and MB2: BT3DB: BT4P: BT5
Obturation:Total Fill BC sealer
Courtesy: Dr. Gilberto Debelian, Norway
Fig. 7
Fig. 9
Fig. 8
Fig. 10
24 I
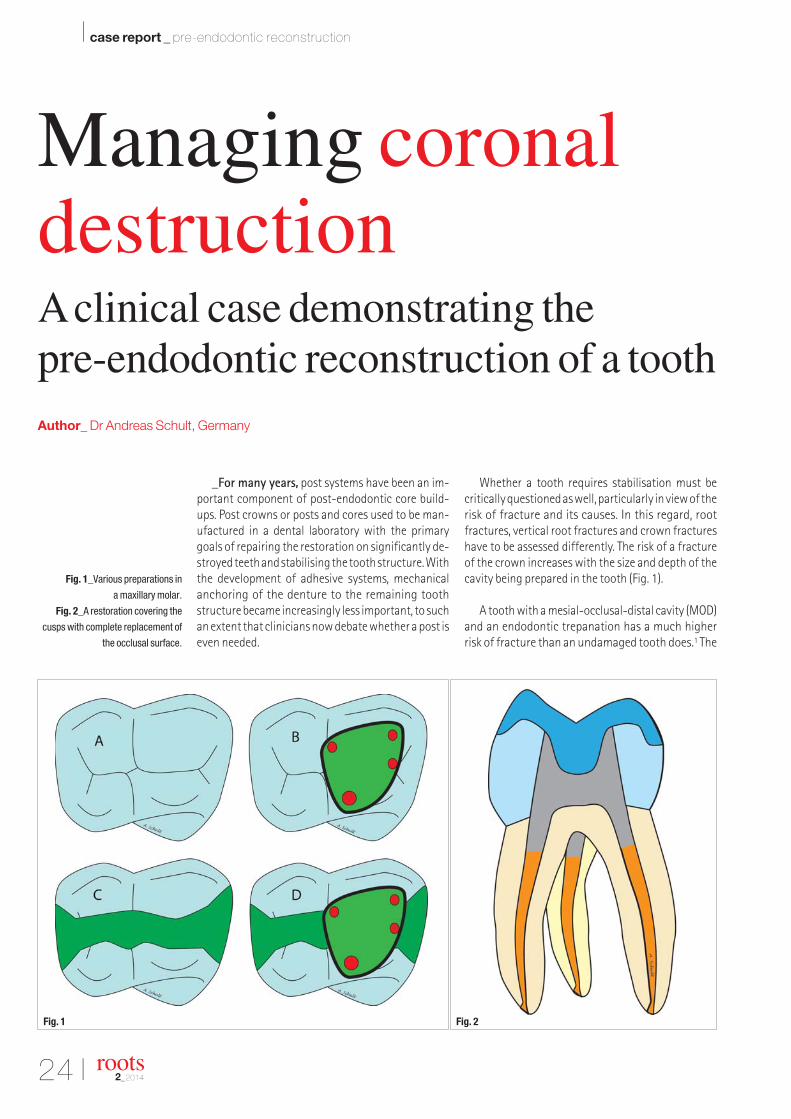
_For many years, post systems have been an im-portant component of post-endodontic core build-ups. Post crowns or posts and cores used to be man-ufactured in a dental laboratory with the primarygoals of repairing the restoration on significantly de-stroyed teeth and stabilising the tooth structure. Withthe development of adhesive systems, mechanicalanchoring of the denture to the remaining toothstructure became increasingly less important, to suchan extent that clinicians now debate whether a post iseven needed.
Whether a tooth requires stabilisation must becritically questioned as well, particularly in view of therisk of fracture and its causes. In this regard, rootfractures, vertical root fractures and crown fractureshave to be assessed differently. The risk of a fractureof the crown increases with the size and depth of thecavity being prepared in the tooth (Fig. 1).
A tooth with a mesial-occlusal-distal cavity (MOD)and an endodontic trepanation has a much higherrisk of fracture than an undamaged tooth does.1 The
Fig. 1_Various preparations in
a maxillary molar.
Fig. 2_A restoration covering the
cusps with complete replacement of
the occlusal surface.
roots2_2014
Managing coronaldestructionA clinical case demonstrating the pre-endodontic reconstruction of a toothAuthor_ Dr Andreas Schult, Germany
I case report _ pre-endodontic reconstruction
Fig. 1 Fig. 2

I 25
case report _ pre-endodontic reconstruction I
roots2_2014
risk of a cusp fracture can be significantly reducedthrough a preparation covering the cusps for endo -dontically treated teeth with an MOD cavity (Fig. 2).2,3
Vertical root fractures differ from fractures in thearea of the crown. Lost endodontically treated teethowing to a vertical fracture are often treated with apost. The difference in the elastic modulus betweenthe hard tooth structure and post material has beensuggested as a cause of a vertical fracture. It can thusbe concluded that post treatment and root canal treat-ment are the primary reasons for a vertical fracture.4
Preparation that preserves hard tooth substance isconsidered to be a superior solution for preventingfractures. In addition, the fracture resistance in thecoronal area is stabilised through adhesive build-upmaterials and restorations that cover the cusps. Thepost and the dentine should have a similar elasticmodulus in order to reduce the risk of a vertical rootfracture. The decision whether to use a post in the caseof an endodontic build-up critically depends on thedegree of destruction of the tooth: the more hardtooth tissue present, the less the need for a post.
The diagram in Figure 3 shows three different degrees of destruction of an anterior tooth. In thecase of a coronally intact but root-filled anterior root,an adhesive restoration is sufficient. When treatingteeth with damage to the hard tissue and for whicha crown is planned, the remaining core height andwidth to be enclosed by the crown play a decisive role(ferrule effect). If the ferrule is more than 2mm wide,a build-up secured with an adhesive is sufficient. If itis narrower than 2mm, the use of a glass fibre post isindicated.
_Clinical case
A busy sales representative came to our practicewith tooth 12 broken. Owing to time constraints, weonly had one hour available for the reconstruction ofthe crown. The fracture line ran circumferentially atthe level of the gingiva (Fig. 4). A root canal treatmenthad been performed on this tooth by another dentistthree months before.
Initially, the patient requested preservation of thetooth but, after discussion, he said that he was notable to invest time in undergoing systematic toothtreatment. The clinical findings showed a retainedroot. The degree of tooth mobility was Grade 0–I andthe probing depth was 1–2mm around the tooth. X-ray images showed a root filling up to approximately
Fig. 3_Various degrees of destruction
of a root-filled anterior tooth.
Fig. 4_Clinical baseline findings:
tooth 12 showed a coronal fracture
circumferentially at the level of the
gingiva.
Fig. 5_Radiological baseline
findings: intra-radicular radiopacity
and apical radiolucency.
Fig. 4 Fig. 5
Fig. 3

26 I
I case report _ pre-endodontic reconstruction
3mm before the radiological apex, as well as apicalradiolucency (Fig. 5).
We diagnosed chronic apical periodontitis in tooth12. The apical radiolucency should be subsequentlyobserved and, if necessary, root canal treatmentshould be revised prior to placing a crown.
Being able to position a rubber dam clamp is a basic prerequisite for endodontic treatment and forpre-endodontic reconstruction. If a clamp cannot bepositioned, surgical crown lengthening is indicated,if applicable (Fig. 6). The retained root was cleared ofremaining tissue, caries and plaque. Then the optimalpost diameter was determined using a stencil. A sizeof 1.5mm was selected.
Since there was only a small amount of remainingtooth substance, the post cavity was prepared to adepth of 6mm and thoroughly rinsed. The canal andremaining exposed dentine were conditioned with35% phosphoric acid for 15 seconds and then rinsedwith a multifunctional syringe for 15 seconds (Fig. 7).
Excess fluid was suctioned off with a micro-suc-tion device. The pre-bond was applied using an appli-cation tip and worked into the surface for 15 seconds.
The micro-suction device was again utilised to re-move any excess.
In order to prepare the bonding material, Bond Aand B were mixed in equal portions for 5 seconds andmassaged into the dentine surface for 20 seconds(Fig. 8). Then they were blown to a thin layer and lightcured for 10 seconds. The tooth was built up with thedual-curing core build-up material LuxaCore Z-Dual(DMG Dental; Fig. 9) and the post cavity was filled withLuxaCore Z-Dual. The LuxaPost post (DMG Dental) waspositioned and the material was light activated (Fig. 10).
The crown was built up in small increments, acti-vated, and contoured and polished with diamondgrinding tools (Figs. 11 & 12)._
Editorial note: A complete list of references is available from
the publisher.
Fig. 6_Isolation of the working
field with a rubber dam and
preparation of the post bed.
Fig. 7_Conditioning of the cavity
with 35 % phosphoric acid.
Fig. 8_Working in the freshly
mixed adhesive for 20 seconds.
Fig. 9_Filling the post cavity
with LuxaCore Z-Dual.
Fig. 10_Insertion of the selected
root post, which was previously
covered with LuxaCore Z-Dual.
Fig. 11_Incremental build-up
of the crown.
Fig. 12_Finished build-up of tooth 12
after contouring and polishing.
roots2_2014
Dr Andreas Schult is a dentist in a joint practice inBad Bramstedt in Germany. He can be contacted [email protected]
_contact roots
Fig. 6
Fig. 9 Fig. 10 Fig. 11 Fig. 12
Fig. 7 Fig. 8

A billion smiles welcome the world of dentistry
FDI 2014 · New Delhi · IndiaGreater Noida (UP)
Annual World Dental Congress11-14 September 2014
www.fdi2014.org.inwww.fdiworldental.org
Standard chargesfor registrations ends
31 July 2014
FDI_LateRegistr_A4.pdf 1FDI_LateRegistr_A4.pdf 1 06.01.14 10:5306.01.14 10:53

28 I
I feature _ case report from Bristol Zoo
_Every endodontic treatment is different. How-ever, if you as a dentist have only half an hour beforerisking your life, if your patient weighs about 22 stone(139.71kg) and if his canines are 14cm long, you areliterally in the lion’s den.
Root canals come in all shapes and sizes. There aremultiple canals, hidden accessory canals or evenhorizontal branches. And sometimes root canalsare just unusually long. In the case of my mostprominent patient so far, the root canal was 9cmlong to be precise. It was a fine male specimen ofPanthera leo persica, an Asiatic lion. When I re-ceived a call from Bristol Zoo to say that theyhad an adult lion with an apparent tooth prob-lem, I was rather intrigued to say the least.
It turned out that the patient was a 17-year-old Asiatic lion named Kamal. The zoo’s veterinarysurgeon informed me that the animal was suffer-ing from a fractured canine tooth and was unable tochew on bones. After our first conversation, we neededto come up with a special treatment plan. Leaving theinfected tooth untreated would have meant a painful
deterioration in his condition, which would ultimatelylead to an infection in his mandible, making life evenmore difficult for the poor animal.
As a veterinary dentist, I have worked on thou-sands of cats and dogs during my 28 years in prac-tice. In terms of anatomy, the canine was very simi-lar to that of my regular patients; it was just scaledup in proportion. Radiographic examination (Figs. 1a& b) showed evidence of an infection around the rootapex. Root canal therapy was indicated. Before ourpatient was ready to undergo surgery, we had to or-der extra-long endodontic files from the US thatwould fit into a 9cm-long root canal. The only filesfit for the purpose are so-called “Tiger Files”. TheseHedstrom files are 12cm long.
_Operating in less than 2 hours
One of the challenges we faced was the time constraints we would be working under; the wholeprocedure had to be done as efficiently as possible.
Figs. 1a & b_A radiograph showing
the root canal.
Fig. 2_GuttaFlow 2 set.
roots2_2014
Root canal therapy settingyour teeth on edge?Author_ Dr Peter Southerden, UK
Fig. 1a Fig. 1b
Fig. 2

I 29
feature _ case report from Bristol Zoo I
roots2_2014
Owing to his age and the fact that the lion wasanaesthetised in field conditions (not in a hospital),we did not want the lion to be anaesthetised for toolong. We thus had to come prepared. In advance, myteam and I had to obtain the correct equipment forsuch a special treatment. The Swiss dental specialistColtène/Whaledent provided us with a fast-flowingfilling system (GuttaFlow 2), which helped us tremen-dously in keeping down the treatment time. In thiscase, we definitely had to reduce “chair time”, if youknow what I mean.
The operation was performed on-site at BristolZoo. After the lion was anaesthetised and placed onthe operating table, we had to perform the treatmentquickly. Dispensing with a dental dam owing to thespecial circumstances, I started to clean and shapethe canal with the Hedstrom files. Their effectivenessin terms of swift dentine removal was a great bene-fit to us. Irrigating the canal did not prove to be easyeither. The main cleaning agent was a sodiumhypochlorite solution with a concentration of 5%. A feline urinary catheter was used for flushing.
After all necrotic pulp tissue and dentine shav-ings had been successfully removed, the canal hadto be obturated with a reliable permanent filling. Itgoes without saying that the average masticatoryforce in lions is considerably larger than it is in hu-man beings. We placed a single master gutta-perchapoint with the help of a plugger. The master pointwas 60mm long and covered with GuttaFlow 2. Thisnew filling system combines cold free-flow gutta-percha and a sealer to create a fast-flowing fillingmaterial that is easy to handle and provides a reli-able barrier against bacteria and liquids re-enteringthe root canal. Its working time is approximately10–15 minutes. After placing the gutta-percha inthe canal from the syringe, it was carried into thecanal using the Hedstroem files. Even in these un-usual working conditions, handling was easy andthe application of the material really straightfor-ward. The short working and curing times helped usto establish a safe seal for the canal within minutes.After the successful obturation of the canal, the final restoration was created with a layer of glassionomer and a normal nano-hybrid composite. Ittook us less than 2 hours to complete the whole pro-cedure.
_Conclusion
The needs of a very large feline patient are notthat different to those of a human patient. The key toa successful endodontic treatment is the effectiveand complete removal of any infected tissue, as wellas quick and safe obturation of the canal. New, inno-vative filling systems have excellent flow properties.
They are easy to handle and help to speed up treat-ment sessions. Two-in-one products, moreover,combine sealer and gutta-percha in powder form toguarantee a tight seal of the root canal for optimumprotection against reinfection. And reduced chairtime is a big bonus to the dentist, whether treatingchildren, patients with dental fear, or lions._
Fig. 3_Filling the root canal with
GuttaFlow 2.
Fig. 4_Radiographic control.
Fig. 3
Fig. 4
Dr Peter Southerden
is a recognised European
Veterinary Dental Specialist.
He is the founder of the
Eastcott Veterinary Clinic
and Hospital in Swindon
in South West England,
where he sees referred
dentistry, and oral and maxillofacial surgery cases.
He is a regular presenter at both UK and international
veterinary conferences.
_about the author roots

30 I
_Introduction
In the May 2013 edition of Photomedicine andLaser Surgery, the editorial written by Prof. Tina Karuis titled “Is it time to consider photobiomodulation asa drug equivalent?” Well, is it? Let us have a look andsee what the literature has to say about two very pop-ular drugs:
NSAIDs (non-steroidal anti-inflammatory drugs)are the best sold pharmaceuticals ever. The short-term effects on pain and inflammation are obviousand valuable. The long-term effects, however, havebeen questioned and this is especially valid consider-ing the many side effects of NSAIDs. Millions of pa-tients are on long-term medication with NSAIDs, andeven lifelong. Indeed, many persons die from theirmedication. So an alternative option is required. I be-lieve it is already available: laser phototherapy! First,let us have a look at the strength of the scientific evi-dence for NSAIDs as such, and long term use of thesein particular:
The meta-analysis by Bjordal1 on the effect ofNSAIDs on knee osteoarthritis pain appears to be-come important for the recognition and future devel-opment of LPT. Let us read the abstract: The researchgroup summarises that non-steroidal anti-inflam-
matory drugs (NSAIDs), including cyclo-oxygenase-2inhibitors (coxibs), reduce short-term pain associatedwith knee osteoarthritis only slightly better thanplacebo, and long-term use of these agents should beavoided. Up for analysis were 23 placebo-controlledtrials involving 10,845 patients, 7,767 of whom re-ceived NSAID therapy and 3,078 placebo therapy. Allin all 21 of the NSAID-studies were funded by thepharmaceutical industry, and the results of 13 ofthese studies were inflated by patient selection bias asprevious NSAID-users were excluded if they had notpreviously responded favourably to NSAID. Such anexclusion criterion for non-responders has neverbeen seen in any controlled trial of LPT or other non-pharmacological therapies of osteoarthritis. In the re-maining ten unbiased NSAID-trials, the differencefrom placebo was only 5.9 mm on a 100 mm painscale.
This is far less than established data on differencesthat are considered minimally perceptible (9 mm) orclinically relevant (12 mm) for knee osteoarthritis pa-tients. In addition, none of the trials found any effectsbeyond 13 weeks. This bleak support for long term useof NSAIDs is an excellent support for non-pharma-ceutical methods, such as LPT. Diclofenac is one of thebest-selling NSAIDs. Several investigators have com-pared the effect of LPT and diclofenac.
roots2_2014
Diclofenac, dexamethasoneor laser phototherapy?Part I
Author_Jan Tunér, Sweden
[PICTURE: ©ROBERT KNESCHKE]
I research _ phototherapy

I 31
research _ phototherapy I
roots2_2014
The aim of a study by Marcos2 was to evaluate theshort-term effects of LPT or sodium diclofenactreatments on biochemical markers and biome-chanical properties of inflamed Achilles tendons.Wistar rats Achilles tendons (n = 6/group) were in-jected with saline (control) or collagenase at peri-tendinous area of Achilles tendons. After one houranimals were treated with two different doses of LPT(810 nm, 1 and 3 J) at the sites of the injections, orwith intramuscular sodium diclofenac. Regardingbiochemical analyses, LPT significantly decreasedCOX-2, TNF-alpha, MMP-3, MMP-9, and MMP-13gene expression, as well as PGE2 production whencompared to collagenase group. Interestingly, di-clofenac treatment only decreased PGE2 levels. Bio-mechanical properties were preserved in the laser-treated groups when compared to collagenase anddiclofenac groups.
Ramos3 investigated the effects of LPT (810 nm) inrat-induced skeletal muscle strain. Male rats wereanaesthetised with halothane prior to the inductionof muscle strain. Previous studies have determinedthat a force equal to 130 % of the body weight corre-sponds to approximately 80 % of the ultimate ruptureforce of the muscle tendon unit. In all animals, theright leg received a controlled strain injury while theleft leg served as control. A small weight correspon-ding to 150 % of the total body weight was attachedto the right leg in an appropriate apparatus and left toinduce muscle strain twice for 20 minutes with three-minute intervals. Walking index, C-reactive protein,creatine kinase, vascular extravasation and histolog-ical analysis of the tibial muscle were performed aftersix, twelve and 24 hours of lesion induction. LPT in anenergy-dependent manner markedly or even com-pletely reduced the Walking Index, leading to a betterquality of movement. C-reactive protein production
was completely inhibited by laser treatment, evenmore than observed with Sodium diclofenac inhibi-tion (positive control). Creative Kinase activity wasalso significantly reduced by laser irradiations. In con-clusion, LPT operating in 810 nm markedly reduced in-flammation and muscle damage after experimentalmuscle strain, leading to a highly significant en-hancement of walking activity.
The aim of the study by de Almeida4 was to analysethe effects of sodium diclofenac (topical application),cryotherapy, and LPT on pro-inflammatory cytokinelevels after a controlled model of muscle injury. For such, we performed a single trauma in the tibialisanterior muscle of rats. After one hour, animals were treated with sodium diclofenac (11.6 mg/g of solution), cryotherapy (20 min), or LPT (904 nm; superpulsed; 700 Hz; 60 mW mean output power;
[PICTURE: ©INESBAZDAR]

32 I
I research _ phototherapy
1.67 W/cm2; 1, 3, 6 or 9 J; 17, 50, 100 or 150 s). As-sessment of interleukin-1 and interleukin-6 (IL-1 andIL-6) and tumour necrosis factor-alpha levels wasperformed at six hours after trauma employing en-zyme-linked immunosorbent assay method. LPT with1 J dose significantly decreased IL-1, IL-6, and TNF-al-pha levels compared to non-treated injured group aswell as diclofenac and cryotherapy groups. On theother hand, treatment with diclofenac and cryother-apy does not decrease pro-inflammatory cytokinelevels compared to the non-treated injured group.Therefore, the authors conclude that 904 nm LPT with1 J dose has better effects than topical application ofdiclofenac or cryotherapy in acute inflammatoryphase after muscle trauma.
The purpose of a study by Albertini5 was to inves-tigate the effect of LPT on the acute inflammatoryprocess. Male rats were used. Paw oedema was in-duced by a sub-plantar injection of carrageenan, thepaw volume was measured before and one, two, threeand four hours after the injection, using a hy-droplethysmometer. To investigate the action mech-anism of the GaAlAs laser on inflammatory oedema,parallel studies were performed using adrenalec-tomised rats or rats treated with sodium diclofenac.Different laser irradiation protocols were employedfor specific energy densities (EDs), exposure times andrepetition rates. The rats were irradiated with laser for80 s each hour. The EDs that produced an anti-in-flammatory effect were 1 and 2.5 J/cm2, reducing theoedema by 27 % and 45.4 %, respectively. The ED of2.5 J/cm2 produced anti-inflammatory effects similarto those produced by the cyclooxigenase inhibitorsodium diclofenac at a dose of 1 mg/kg. In adrenalec-tomised animals, the laser irradiation failed to inhibitthe oedema. These results suggest that LPT possiblyexerts its anti-inflammatory effects by stimulatingthe release of adrenal corticosteroid hormones.
The aim of a work by Meneguzzo6 was to investi-gate the effects of infrared 810 nm on the acute in-flammatory process by the irradiation of lymphnodes, using the classical model of carrageenan-in-duced rat paw oedema. Thirty mice were randomly di-vided into five groups. The inflammatory inductionwas performed in all groups by a sub-plantar injectionof carrageenan (1 mg/paw). The paw volume wasmeasured before and 1, 2, 3, 4 and 6 hours after theinjection using a plethysmometer. Myeloperoxidase(MPO) activity was analysed as a specific marker ofneutrophil accumulation at the inflammatory site.The control group did not receive any treatment (GC);GD group received sodium diclofenac (1mg/kg) 30minutes before the carrageenan injection; GP groupreceived laser irradiation directly on the paw (1 Joule,100 mW, 10 sec) one and two hours after the car-rageenan injection; GLY group received laser irradia-tion (1 Joule, 100 mW, 10 sec) on the inguinal lymphnodes; GP+LY group received laser irradiation on bothpaw and lymph nodes one and two hours after thecarrageenan injection. MPO activity was similar in thesodium diclofenac as well as in the GP and GLY groups,but significantly lower than the GC and GP + LYgroups. Paw oedema was significantly inhibited in GPand GD groups when compared to the other groups.Interestingly, the GP+LY groups presented the biggestoedema, even bigger than in the control group. LPTshowed an anti-inflammatory effect when the irradi-ation was performed on the site of lesion or at the cor-related lymph nodes, but showed a pro-inflammatoryeffect when both paw and lymph nodes were irradi-ated during the acute inflammatory process.
The aim of a study by Barretto23 was to investigatethe analgesic and anti-inflammatory activity of LPTon the nociceptive behavioural as well as histomor-phological aspects induced by injection of formalinand carrageenan into the rat temporomandibularjoint. The 2.5 % formalin injection (FRG group) in-duced behavioural responses characterized by rub-bing the orofacial region and flinching the headquickly, which were quantified for 45 min. The pre-treatment with systemic administration of diclofenacsodium-DFN group (10 mg/kg i.p.) or irradiation withinfrared LPT (LST group, 780 nm, 70 mW, 30 s, 2.1 J,52.5 J/cm2), significantly reduced the formalin- induced nociceptive responses. The 1 % carrageenaninjection (CRG group) induced inflammatory re-sponses over the time-course of the study (24 h, threeand seven days) characterised by the presence of intense inflammatory infiltrate rich in neutrophils,scanty areas of liquefactive necrosis and intense in-terstitial oedema, extensive haemorrhagic areas, andenlargement of the joint space on the region. The DFNand LST groups showed an intensity of inflammatoryresponse that was significantly lower than in CRGgroup over the time-course of the study, especially in
roots2_2014
[PICTURE: ©RACORN]

I 33
research _ phototherapy I
roots2_2014
the LST group, which showed exuberant granulationtissue with intense vascularization, and deposition ofnewly formed collagen fibres (three and seven days).
The aim of a study by de Almeida7 was to analysethe effects of sodium diclofenac (topical application)and LPT on morphological aspects and gene expres-sion of biochemical inflammatory markers. The re-searchers performed a single trauma in the tibialis an-terior muscle of rats. After one hour, animals weretreated with sodium diclofenac (11.6 mg/g of solu-tion) or LPT (810 nm; continuous mode; 100 mW; 1, 3or 9 J; 10, 30 or 90 s). Histological analysis and quan-tification of gene expression (real-time polymerasechain reaction-RT-PCR) of cyclooxygenase 1 and 2(COX-1 and COX-2) and tumour necrosis factor-alpha(TNF-alpha) were performed at six, twelve and 24 h af-ter trauma. LPT with all doses improved morphologi-cal aspects of muscle tissue, showing better resultsthan injury and diclofenac groups. All LPT doses alsodecreased COX-2 compared to injury group and to di-clofenac group at 24 h after trauma. In addition, LPTdecreased TNF-alpha compared both to injury and di-clofenac groups. LPT mainly with dose of 9 J is betterthan topical application of diclofenac in acute in-flammation after muscle trauma.
Yet another study by Marcos8 investigated if asafer treatment such as LPT could reduce tendinitisinflammation, and whether a possible pathway couldbe through inhibition of either of the two-cyclooxy-genase (COX) isoforms in inflammation. Wistar rats(six animals per group) were injected with saline (con-trol) or collagenase in their Achilles tendons. Thenthey were treated with three different doses of IR LPT(810 nm; 100 mW; 10 s, 30 s and 60 s; 3.57 W/cm2; 1 J,3 J, 6 J) at the sites of the injections, or intramusculardiclofenac, a nonselective COX inhibitor/NSAID. Itwas found that LPT dose of 3 J significantly reducedinflammation through less COX-2-derived gene ex-pression and PGE2 production, and less oedema for-mation compared to non-irradiated controls. Di-clofenac controls exhibited significantly lower PGE2cytokine levels at 6 h than collagenase control, butCOX isoform 1-derived gene expression and cytokinePGE2 levels were not affected by treatments. As LPTseems to act on inflammation through a selective in-hibition of the COX-2 isoform in collagenase-inducedtendinitis, LPT may have the potential to become anew and safer non-drug alternative to coxibs.
The aim of the study by de Paiva Carvalho9 was toevaluate the effect of single and combined therapies(LPT, topical application of diclofenac and intramus-cular diclofenac) on functional and biochemical as-pects in an experimental model of controlled musclestrain in rats. Muscle strain was induced by overload-ing tibialis anterior muscle of rats. Injured groups re-
ceived either no treatment, or a single treatment withtopical or intramuscular diclofenac (TD and ID), or LPT(3 J, 810 nm, 100 mW) 1 h after injury. Walking trackanalysis was the functional outcome and biochemi-cal analyses included mRNA expression of COX-1 andCOX-2 and blood levels of prostaglandin E2 (PGE2). Alltreatments significantly decreased COX-1 and COX-2gene expression compared to the injury group. How-ever, LPT showed better effects than TD and ID re-garding PGE2 levels and walking track analysis. Theauthor concludes that LPT has more efficacy thantopical and intramuscular diclofenac in treatment ofmuscle strain injury in acute stage.
Crystalopathies are inflammatory pathologiescaused by cellular reactions to the deposition of crys-tals in the joints. The anti-inflammatory effect of He-Ne laser and that of the non-steroidal anti-inflam-matory drugs (NSAIDs) diclofenac, meloxicam, cele-coxib, and rofecoxib was studied in acute and chronicarthritis produced by hydroxyapatite and calcium py-rophosphate in rats. The presence of the markers fib-rinogen, L-citrulline, nitric oxide, and nitrotyrosinewas determined. In the study by Rubio10, crystals wereinjected into the posterior limb joints of the rats. Adose of 8 J/cm2 of energy from a HeNe laser was ap-plied for three days in some groups and for five daysin other groups. The levels of some of the biomarkerswere determined by spectrophotometry, and that ofnitrotyrosine was determined by ELISA. In arthriticrats, the fibrinogen, L-citrulline, nitric oxide, and ni-trotyrosine levels increased in comparison to controlsand to the laser-treated arthritic groups. When com-paring fibrinogen from arthritic rats with disease in-duced by hydroxyapatite to healthy and arthritic ratstreated with NSAIDs, the He-Ne laser decreased lev-els to values similar to those seen in controls. Inflam-matory and oxidative stress markers in experimentalcrystalopathy are positively modified by photobios-timulation._
Editorial note: To be continued with further studies on
the effectiveness of diclofenac and LPT and conclusion
in roots 3/2014. An list of references is available from the
author.
Jan Tunér
Spjutvagen 11
772 32 Grängesberg
Sweden
_contact roots
I industry news _ Sirona
_Sirona reports on the wide range of applica-tions of diode lasers in a special edition of the Eng-lish-language “Laser – International Magazine ofLaser Dentistry.” The "SIROLaser Factbook—Clinicalarticles about SIROLaser Advance and Xtend appli-cations" includes research by well-known experts aswell as informative field reports from experiencedusers of laser technology.
Compact and informative: Sixty pages full of solidexpertise and practical applications await the read-ers of English texts collected by Sirona in “SIROLaserFactbook—Clinical articles about SIROLaser Advanceand Xtend applications.” Academic articles and real-life user reports by well-known experts provide in-formation on the many uses and treatment optionsof diode lasers with a wavelength of 970nm. Inter-esting facts and figures, study results, documentedcase studies with descriptive pictures, and recom-mendations for further reading complete the com-pendium.
“Anyone with an interest in laser dentistry shouldread the SIROLaser Factbook,” says Ingo Höver, prod-uct manager at Sirona. The book is especially meantfor beginners, says the laser specialist. “However, ex-perienced users will also find it worth reading. I amsure that they will be surprised to learn the many pos-sibilities of diode lasers and the range of applicationsthat are open to them with models like the SIROLaserAdvance or SIROLaser Xtend.”
_Routine and less common aspects ofdental treatment
The 970 nm diode laser discussed in the SIROLaserFactbook covers a variety of dental indications, saysco-publisher and co-author Prof. Andreas Braunfrom the Center for Dental and Oral Medicine of theUniversity of Marburg. These include incision/exci-sion associated with gingivectomy, gingivoplasty,implant exposure, and removal of abnormal tissueand reducing bacteria as a supporting measure inperiodontal, peri-implant or endodontic proceduresas well as adjunctive therapy in the treatment ofaphthous ulcers. “The selected articles cover bothroutine and less common aspects of dental treat-ment with a particular focus on new treatmentstrategies combined with conventional techniques,”says Prof. Braun.
Fig. 1_Compact information on
lasers: SIROLaser Factbook.
SIROLaser Factbook: Comprehensive informationon diode lasers
34 I roots2_2014

I 35roots2_2014
“There are few instruments that symbolizemodernity and innovation in dentistry more than thelaser,” says Prof. Roland Frankenberger. Laser appli-cations in dentistry are now scientifically estab-lished. The President of the German Society forRestorative Dentistry (DGZ) writes in his foreword, “I am especially pleased that a variety of interestingaspects of routine work are examined and lasertreatment is conveyed objectively, but with enthusi-asm.” Prof. Braun hopes, “Perhaps new recommen-dations for day-to-day practice will result from thetreatment procedures described.”
_Relaxed dentists and relaxed patients
Sirona, global innovation leader for dental equip-ment, has two laser models in its product portfoliothat set new standards: SIROLaser Xtend with an up-grade option for beginners and SIROLaser Advancefor experts. The lasers stand for safe, precise proce-dures, gentle, pain-free treatment, lasting product
quality, and top design. The SIROLaser Advance andSIROLaser Xtend ensure relaxed dentists and relaxedpatients. More information for dentists and the com-pendium “SIROLaser Factbook – Clinical articles aboutSIROLaser Advance and Xtend applications” are avail-able for download at www.sirona.de._
Fig. 2_SIROLaser Advance and Xtend
– two models for safe, precise,
pain-free treatment.
Sirona Dental GmbH
Sirona Straße 1
5071 Wals bei Salzburg
Austria
www.sirona.com
_contact roots
industry news _ Sirona I

Planmeca Oy
Asentajankatu 6
00880 Helsinki
Finland
www.planmeca.com
_contact roots
36 I
I industry news _ Planmeca
_Dental technology company Planmeca and theUniversity of Turku have founded a joint venture com-pany, the Nordic Institute of Dental Education. The in-stitute will offer high-quality continuing educationcourses to dental professionals.
The objective is to export and share Nordic ex-pertise in digital dentistry on the basis of theacademic knowledge of the University ofTurku and the technologies developed byPlanmeca, as well as their global dentalnetworks.
The courses will be held at the Univer-sity of Turku and at Planmeca’s head-quarters in Helsinki from autumn2014. The course topics cover rap-idly evolving dental technologiesand their application in moderndentistry, including 3-D imag-ing, prosthodontics, endodon-tics, biomaterials science, or-thodontics and CAD/CAM tech-nologies.
The University of Turku awards ECTScredits (a standard for higher educationin Europe) and course certificates to thestudents. The joint venture companycomplements Planmeca’s broad rangeof training activities and collaborationwith universities around the world.
The University of Turku is an activeparticipant in the export of education.“We have now established a partnershipwith one of the world’s leading compa-nies in dental technology. Together withPlanmeca we are a strong educationprovider globally,” stated Prof. KalervoVäänänen, Rector of the University ofTurku._
Fig. 1_The objective of the new
institute is to export and share Nordic
expertise in digital dentistry on the
basis of academic knowledge and
technologies. (Photo: Planmeca)
roots2_2014
Planmeca and the University
of Turku found Nordic Institute
of Dental Education

Y education everywhere and anytime
Y live and interactive webinars
Y more than 500 archived courses
Y a focused discussion forum
Y free membership
Y no travel costs
Y no time away from the practice
Y interaction with colleagues and experts across the globe
Y a growing database of scientific articles and case reports
Y ADA CERP-recognized credit administration
ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providersof continuing dental education.ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry.
www.DTStudyClub.com
Register for
FREE!
DTSC_A4_EN.pdf 1DTSC_A4_EN.pdf 1 05.02.14 11:1405.02.14 11:14

38 I
I meetings _ AAE
_Endodontists from around the worldand acrossthe country gathered at the Gaylord National resortjust outside Washington, D.C., for the 2014 AAE An-nual Session. From lectures to hands-on workshopsto formal and informal social gatherings, the meeting,held from April 30 to May 3, offered a wide range ofopportunities for attendees.
James Bradley, author of the New York Times best-seller “Flags of Our Fathers,” gave the keynote address.Bradley, whose book follows the lives of the five USMarines and one US Navy Corpsman who wouldeventually be made famous by Joe Rosenthal’s lauded
photograph of the flag raising at Iwo Jima, offered aninspirational message to those in attendance: Noth-ing is impossible.
The exhibit hall featured products and servicesfrom several hundred companies, as well as variouseducational opportunities.
A “Corporate Workshop and Lecture” series waspresented on the show floor. Some of the highlightsincluded “Surgical Applications of Bioceramics,” spon-sored by Brasseler USA, presented by Dr Ali Nasseh;“The Rationale and Use of Electronic Apex Locators,”sponsored by J. Morita USA, presented by Dr L. StephenBuchanan; and “Sound Science: Multisonic Ultra-cleaning,” sponsored by Sonendo Inc., presented byDr. Mehrzad Khakpour.
A number of companies used the meeting as an occasion to launch new products.
Sonendo unveiled its new GentleWave System uti-lizing patented Multisonic Ultracleaning technologythat is designed to quickly, easily and safely loosen andremove pulp tissue, debris, decay and bacteria withinminutes. The system is designed to clean the entirecanal system, automatically and simultaneously.
roots2_2014
“Striving for perfection”—AAE holds 2014 AnnualSession in WashingtonAuthor_ Fred Michmershuizen, DTA
Fig. 3_Meeting attendees try
new endodontic technology
available from Sonendo Inc.
Fig. 4_Dr Manor Haas demonstrates
the use of a surgical operating
microscope at the Zeiss booth.
Fig. 1_ Meeting participants work
with apex locators during a hands-on
workshop, „The Rationale and Use of
Electronic Apex Locators,” presented
by Dr L. Stephen Buchanan.
Fig. 2_AAE President Gary Hartwell
welcomes meeting attendees to the
2014 AAE Annual Session.
Fig. 1 Fig. 2
Fig. 3 Fig. 4

I 39
meetings _ AAE I
roots2_2014
Bjarne Bergheim, president and CEO of Sonendo,has been directly involved in the development of theGentleWave since its early inception. “Very soon, en-dodontists performing root canal therapy will havethe ability to provide an ultraclean environment fortheir patients in a more comprehensive, efficient andpredictable way,” he said. “We remain focused on cre-ating a new standard of care for the patient as well asimproving the clinical quality and business perform-ance of doctors performing root canal therapy.”
DENTSPLY Tulsa Dental Specialties launched Pro-Taper Gold rotary files, featuring what it calls “thesame efficient, variable tapered shapes and pre-dictable performance that clinicians have knownand trusted from ProTaper Universal, with increasedflexibility.”
According to DENTSPLY Tulsa, ProTaper Gold’sproprietary advanced metallurgy creates a differenceclinicians can see and feel. ProTaper Gold files havethe same geometry as ProTaper Universal, but with anincrease in flexibility. This is especially important inthe finishing files, which must navigate challengingcurves in the apical region of the canal, the companysays. The files also feature a shorter, 11-mm handlefor improved accessibility to teeth.
Brasseler introduced its ESX Rotary File. Designedwith several performance-enhancing patented fea-tures, ESX Rotary Files are designed for a powerfulyet minimally invasive performance, maximizing thelong-term success of the treated tooth, the companysays.
J. Morita unveiled its Root ZX II OTR Module, a new,low-speed handpiece for its popular apex locator.According to the company, the new OTR Module safelyand efficiently prepares canals while simultaneouslytaking measurements.
Several companies exhibited at the AAE meetingfor the first time. Among them: Edge Endo, whose“biker chicks” and rock ’n’ roll-themed booth had at-tendees looking twice; Avalon Biomed, with its newGrey MTA bioactive root and pulp treatment material;and Rapid City, S.D.-based Mounce Endo, offering itsown MounceFiles, plus a full range of supplies fromMani, Aseptico, San Diego Swiss Ultrasonics andMetaBiomed.
The 2015 AAE meeting is scheduled for May 6 to 9in Seattle._
Photos: Fred Michmershuizen
Fig. 5_Dr Rich Mounce (left) and
Dr C. John Munce.
Fig. 6_Dr Mehrzad Khakpour
presents „Sound Science: Multisonic
Ultracleaning,” one of several „To the
Point” lectures offered on the exhibit
hall floor.
Fig. 7_James Bradley, author
of the New York Times bestseller
„Flags of Our Fathers,” offers the
keynote address.
Fig. 8_Dr Allen Ali Nasseh offers
a presentation on endodontic files
in the „To the Point” educational
theater on the exhibit hall floor.
Fig. 5 Fig. 6
Fig. 7 Fig. 8

2014
18th World Congress on Dental Traumatology
19–21 June 2014Istanbul, Turkeywww.iadt-dentaltrauma.org/2014conference/index.html
2014 AAE/AAP/ACP Join Symposium
Teeth for a life time: Interdisciplinary Evidence
for Clinical Success
19–20 July 2014Chicago, USAwww.perio.org/meetings/joint-symposium2014.htm
Scand Endo Reykjavik 2014
21–23 August 2014 Reykjavik, Iceland
FDI Annual World Dental Congress
17–19 June 2014Dubai, UAEwww.apdentalcongress.org
Italian Academy of Endodontics (AIE)
22nd National Congress
2–4 October 2014Montecatini Terme, Italywww.accademiaitalianaendodonzia.it
155th ADA Annual Session
9–12 October 2014San Antonio, USAwww.ada.org
Digital Dentistry Show
16–18 October 2014At the International Expodental Milano, Italywww.digitaldentistryshow.com
ROOTS Summit
7–9 November 2014Chennai, Indiawww.rootssummit2014.com
BES: 2014 Regional Meeting
14–15 November 2014 Manchester, UKwww.britishendodonticsociety.org.uk
ADF Meeting
25–29 November 2014Paris, Francewww.adf.asso.fr
Great New York Dental Meeting
28 November–3 December 2014New York, USAwww.gnydm.com
Austrian Society of Endodontology Annual
Meeting & PENN ENDO Global Symposium
4–6 December 2014Vienna, Austriawww.pennglobalvienna2014.at/
International Events
40 I
I events _ meetings
roots2_2014

submission guidelines:Please note that all the textual components of your submissionmust be combined into one MS Word document. Please do not submit multiple files for each of these items:
_the complete article;_all the image (tables, charts, photographs, etc.) captions;_the complete list of sources consulted; and_the author or contact information (biographical sketch, mailingaddress, e-mail address, etc.).
In addition, images must not be embedded into the MS Word document. All images must be submitted separately, and detailsabout such submission follow below under image requirements.
Text length
Article lengths can vary greatly—from 1,500 to 5,500 words— depending on the subject matter. Our approach is that if you need more or less words to do the topic justice, then please makethe article as long or as short as necessary.
We can run an unusually long article in multiple parts, but thisusually entails a topic for which each part can stand alone be-cause it contains so much information.
In short, we do not want to limit you in terms of article length, so please use the word count above as a general guideline and ifyou have specific questions, please do not hesitate to contact us.
Text formatting
We also ask that you forego any special formatting beyond theuse of italics and boldface. If you would like to emphasise certainwords within the text, please only use italics (do not use underli-ning or a larger font size). Boldface is reserved for article headers.Please do not use underlining.
Please use single spacing and make sure that the text is left jus -tified. Please do not centre text on the page. Do not indent para-graphs, rather place a blank line between paragraphs. Please donot add tab stops.
Should you require a special layout, please let the word processingprogramme you are using help you do this formatting automati-cally. Similarly, should you need to make a list, or add footnotes or endnotes, please let the word processing programme do it foryou automatically. There are menus in every programme that willenable you to do so. The fact is that no matter how carefully done,errors can creep in when you try to number footnotes yourself.
Any formatting contrary to stated above will require us to removesuch formatting before layout, which is very time-consuming.Please consider this when formatting your document.
Image requirements
Please number images consecutively throughout the article by using a new number for each image. If it is imperative that certain images are grouped together, then use lowercase lettersto designate these in a group (for example, 2a, 2b, 2c).
Please place image references in your article wherever they are appropriate, whether in the middle or at the end of a sentence.If you do not directly refer to the image, place the reference at the end of the sentence to which it relates enclosed withinbrackets and before the period.
In addition, please note:
_We require images in TIF or JPEG format._These images must be no smaller than 6 x 6 cm in size at 300 DPI._These image files must be no smaller than 80 KB in size (or theywill print the size of a postage stamp!).
Larger image files are always better, and those approximately the size of 1 MB are best. Thus, do not size large image files downto meet our requirements but send us the largest files available.(The larger the starting image is in terms of bytes, the more lee-way the designer has for resizing the image in order to fill up morespace should there be room available.)
Also, please remember that images must not be embedded intothe body of the article submitted. Images must be submitted separately to the textual submission.
You may submit images via e-mail, via our FTP server or post a CD containing your images directly to us (please contact us for the mailing address, as this will depend upon the country fromwhich you will be mailing).
Please also send us a head shot of yourself that is in accordancewith the requirements stated above so that it can be printed withyour article.
Abstracts
An abstract of your article is not required.
Author or contact information
The author’s contact information and a head shot of the authorare included at the end of every article. Please note the exact information you would like to appear in this section and for-mat it according to the requirements stated above. A short biographical sketch may precede the contact information if you provide us with the necessary information (60 words or less).
Questions?
Magda Wojtkiewicz (Managing Editor)[email protected]
about the publisher _ submission guidelines I
I 41roots2_2014

rootsinternational magazine of endodontology
I about the publisher _ imprint
Copyright Regulations
_roots international magazine of endodontology is published by Oemus Media AG and will appear in 2014 with one issue every quarter. The magazine and all articles and illustrations therein are protected by copyright. Any utilisation without the prior consent of editor and publisher is inadmissible and liableto prosecution. This applies in particular to duplicate copies, translations, microfilms, and storage and processing in electronic systems.
Reproductions, including extracts, may only be made with the permission of the publisher. Given no statement to the contrary, any submissions to theeditorial department are understood to be in agreement with a full or partial publishing of said submission. The editorial department reserves the right tocheck all submitted articles for formal errors and factual authority, and to make amendments if necessary. No responsibility shall be taken for unsolicitedbooks and manuscripts. Articles bearing symbols other than that of the editorial department, or which are distinguished by the name of the author, representthe opinion of the afore-mentioned, and do not have to comply with the views of Oemus Media AG.Responsibility for such articles shall be borne by the author.Responsibility for advertisements and other specially labeled items shall not be borne by the editorial department. Likewise, no responsibility shall be assumedfor information published about associations, companies and commercial markets. All cases of consequential liability arising from inaccurate or faulty representation are excluded. General terms and conditions apply, legal venue is Leipzig, Germany.
PublisherTorsten R. Oemus [email protected]
CEOIngolf Dö[email protected]
Members of the BoardJürgen [email protected]
Lutz V. [email protected]
Managing EditorMagda [email protected]
Executive ProducerGernot [email protected]
Designer Josephine [email protected]
Copy EditorsSabrina RaaffHans Motschmann
Published byOemus Media AGHolbeinstraße 2904229 Leipzig, GermanyTel.: +49 341 48474-0Fax: +49 341 [email protected]
Printed bySilber Druck oHGAm Waldstrauch 134266 Niestetal, Germany
Editorial BoardFernando Goldberg, ArgentinaMarkus Haapasalo, CanadaKen Serota, CanadaClemens Bargholz, GermanyMichael Baumann, GermanyBenjamin Briseno, GermanyAsgeir Sigurdsson, IcelandAdam Stabholz, IsraelHeike Steffen, GermanyGary Cheung, Hong KongUnni Endal, NorwayRoman Borczyk, PolandBartosz Cerkaski, PolandEsteban Brau, SpainJosé Pumarola, SpainKishor Gulabivala, United KingdomWilliam P. Saunders, United KingdomFred Barnett, USAL. Stephan Buchanan, USAJo Dovgan, USAVladimir Gorokhovsky, USAJames Gutmann, USABen Johnson, USAKenneth Koch, USASergio Kuttler, USAJohn Nusstein, USAOve Peters, USAJorge Vera, Mexico
Magda Wojtkiewicz, Managing Editor
42 I roots2_2014

rootsinternational magazine of endodontology
I would like to subscribe to roots for € 44 includingshipping and VAT for German customers, € 46 includingshipping and VAT for customers outside Germany, unlessa written cancellation is sent within 14 days of thereceipt of the trial subscription. The subscription willbe renewed automatically every year until a writtencancellation is sent to OEMUS MEDIA AG, Holbeinstr. 29,04229 Leipzig, Germany, six weeks prior to the renew-al date.
Last Name, First Name
Company
Street
ZIP/City/Country
E-mail Signature
Signature
OEMUS MEDIA AGHolbeinstraße 29, 04229 Leipzig, Germany, Tel.: +49 341 48474-0, Fax: +49 341 48474-290, E-mail: [email protected]
Reply via Fax to +49 341 48474-290 to OEMUS MEDIA AG or via E-mail to [email protected]
Notice of revocation: I am able to revoke the subscription within 14 days after my order by sen-ding a written cancellation to OEMUS MEDIA AG, Holbeinstr. 29, 04229 Leipzig, Germany.
root
s 2/1
4
Subscribe now!
You can also subscribe via www.oemus.com/abo
roots_Abo_A4_engl.pdf 1roots_Abo_A4_engl.pdf 1 04.07.14 11:2104.07.14 11:21

Planmeca Oy Asentajankatu 6, 00880 Helsinki, Finland. Tel. +358 20 7795 500, fax +358 20 7795 555, [email protected]
Find more info and your local dealer www.planmeca.com
• Extremely high resolution with 75 μm voxel size
• Noise-free images with intelligent Planmeca AINO™ lter
• rtefact-free images with e cient Planmeca ARA™ algorithm
Planmeca ProMax® 3DEndodontic imaging mode – a new era in precision
l a l e ma nCBCT imaging with an even lower patient dose than panoramic imaging.
Adult female, FOV Ø200 x 180 mm E ective dose 14.7 μSv Planmeca ProMax® 3D Mid
Create your virtual patientA world rst One imaging unit, three types of 3D data. All in one software.
CBCT + 3D model scan + 3D face photo
Other unique features in Planmeca ProMax® 3D family units
Planmeca_A4_roots214.pdf 1Planmeca_A4_roots214.pdf 1 04.04.14 13:3904.04.14 13:39


















