







Languages
Pages
Legal

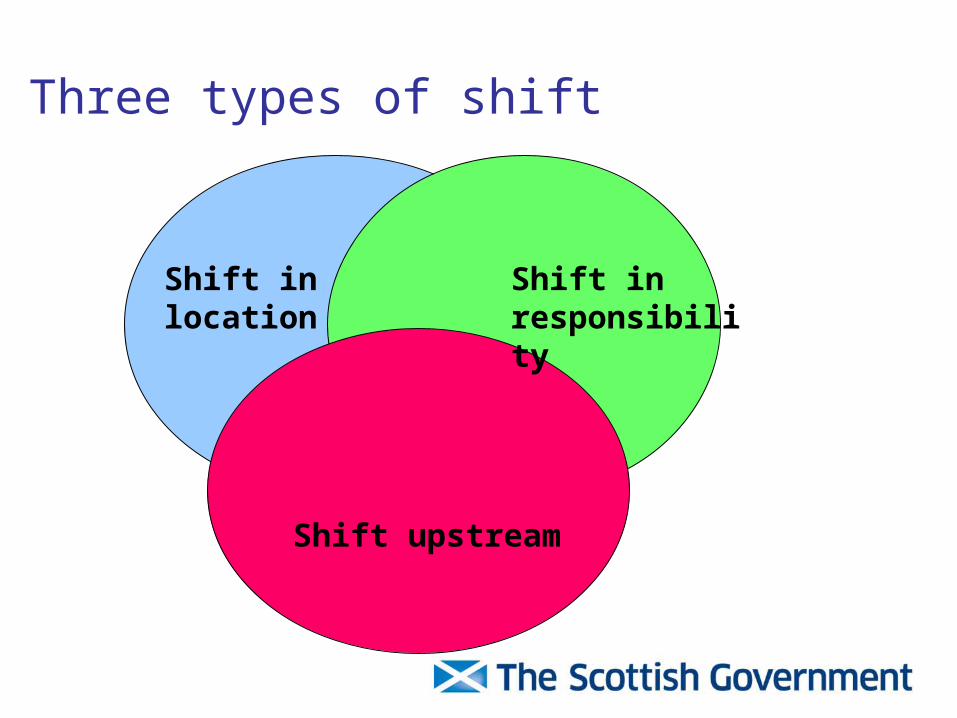
Three types of shift
Shift in responsibility
Shift upstream
Shift in location
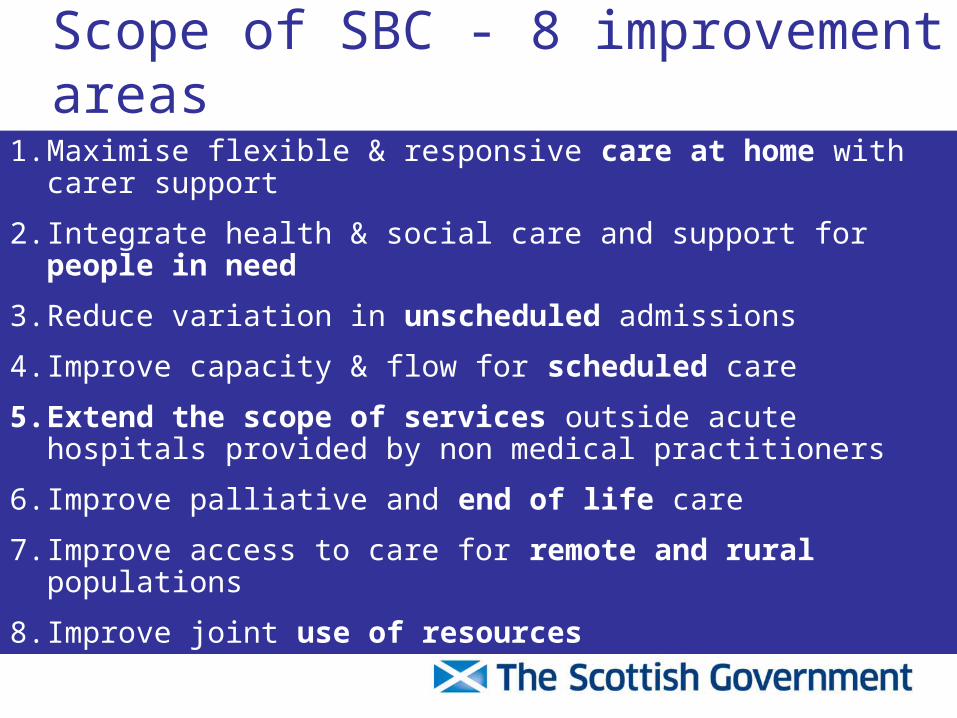
Scope of SBC - 8 improvement areas
1. Maximise flexible & responsive care at home with carer support
2. Integrate health & social care and support for people in need
3. Reduce variation in unscheduled admissions
4. Improve capacity & flow for scheduled care
5. Extend the scope of services outside acute hospitals provided by non medical practitioners
6. Improve palliative and end of life care
7. Improve access to care for remote and rural populations
8. Improve joint use of resources
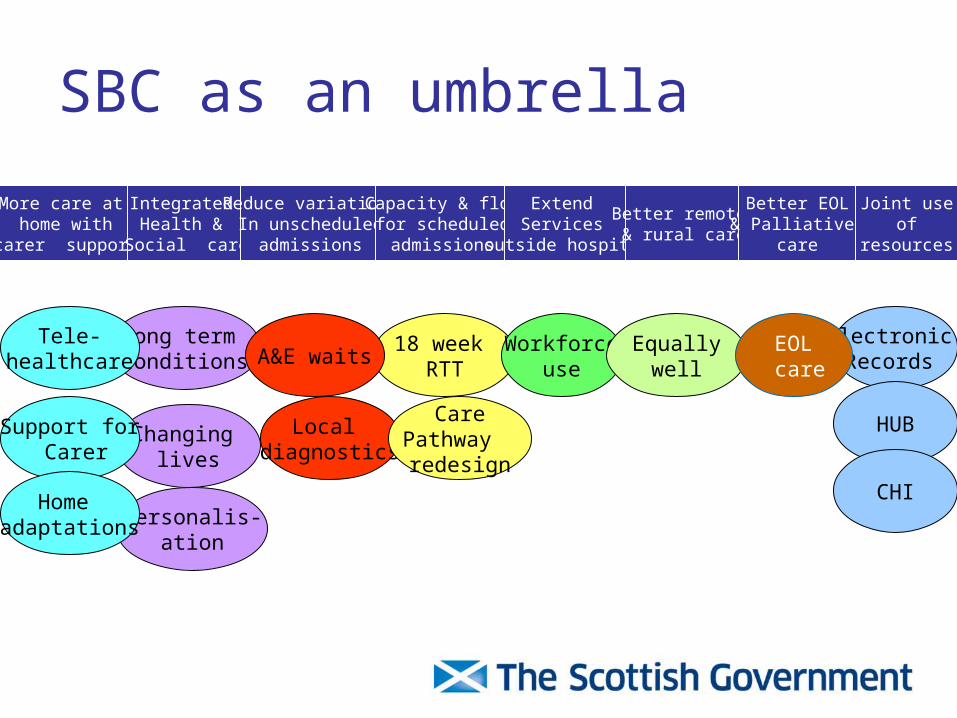
SBC as an umbrella
More care at home with
carer support
Integrated Health &
Social care
Reduce variation In unscheduled
admissions
Capacity & flow for scheduled
admissions
Extend Services
outside hospital
Better remote & rural care
Better EOL& Palliative
care
Joint use of
resources
Long term conditions
18 week RTT
Workforceuse
Electronic Records
Changing lives
Personalis-ation
Tele-healthcare
Support for Carer
A&E waitsEqually
wellEOL care
HUB
CHIHome adaptations
Local diagnostics
CarePathway redesign
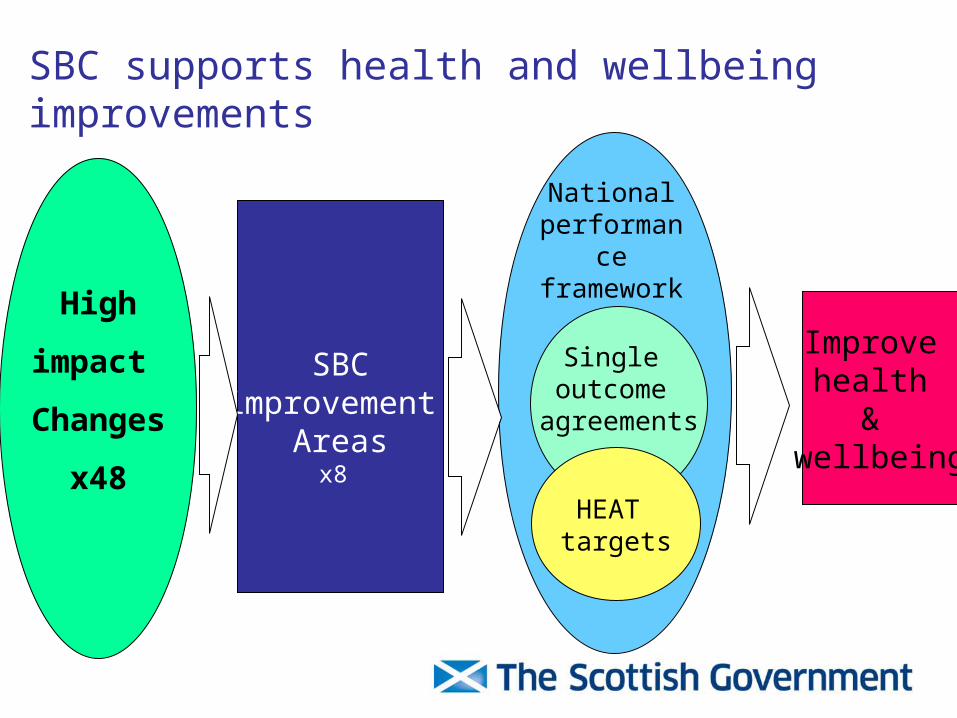
SBC supports health and wellbeing improvements
Single outcome
agreements
HEAT targets
National performance framework
High
impact
Changes
x48
SBCimprovement
Areasx8
Improve health
& wellbeing
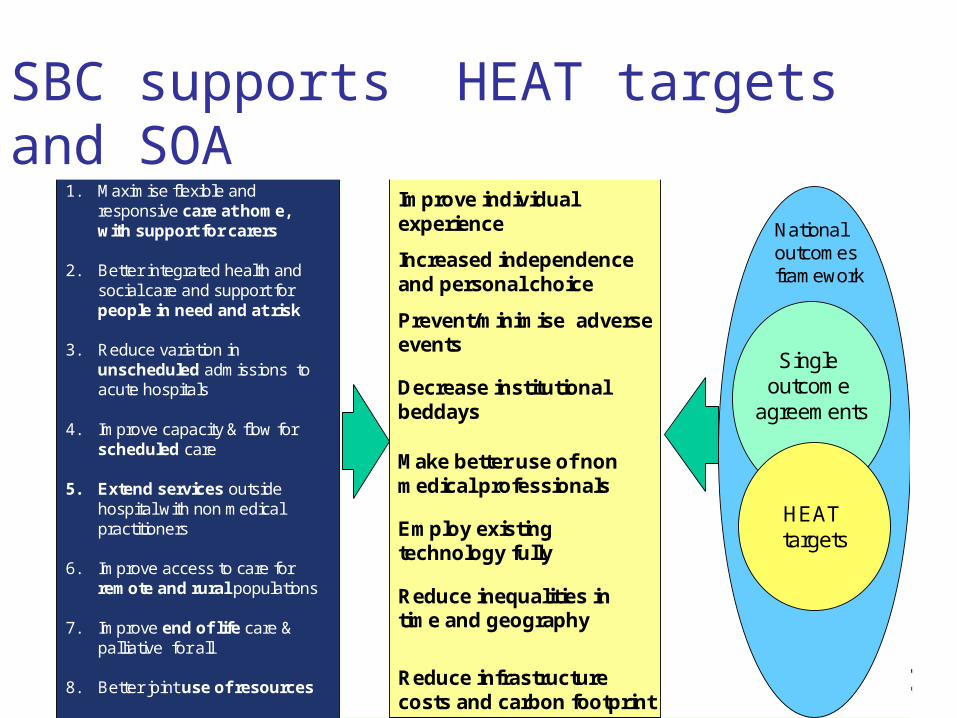
1. Maximise flexible and responsive care at home, with support for carers
2. Better integrated health and social care and support for people in need and at risk
3. Reduce variation in unscheduled admissions to acute hospitals
4. Improve capacity & flow for scheduled care
5. Extend services outside hospital with non medical practitioners
6. Improve access to care for remote and rural populations
7. Improve end of life care & palliative for all
8. Better joint use of resources
Reduce inequalities in time and geography
Decrease institutional beddays
Prevent/minimise adverse events
Make better use of non medical professionals
Reduce infrastructure costs and carbon footprint
Employ existing technology fully
Improve individual experience
8 SBC impact areas Shifts/improvements
Single outcome
agreements
HEAT targets
Increased independence and personal choice
National outcomes framework
SBC supports HEAT targets and SOA
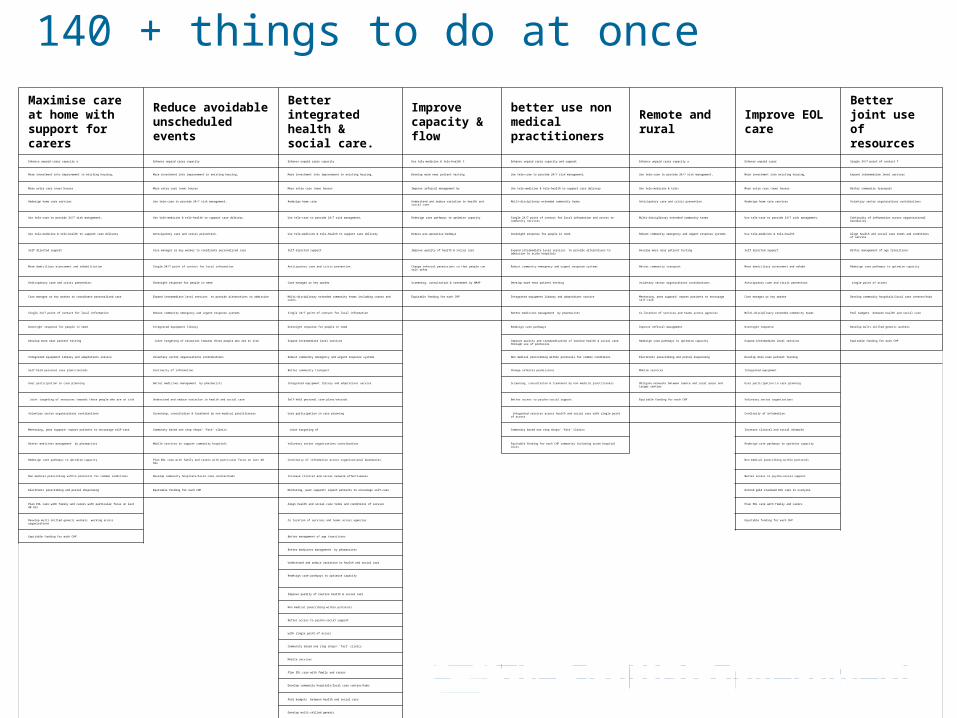
Maximise care at home with support for carers
Reduce avoidable unscheduled events
Better integrated health & social care.
Improve capacity & flow
better use non medical practitioners
Remote and rural
Improve EOL care
Better joint use of resources
Enhance unpaid carer capacity a Enhance unpaid carer capacity Enhance unpaid carer capacity Use tele-medicine & tele-health t Enhance unpaid carer capacity and support Enhance unpaid carer capacity a Enhance unpaid carer Single 24/7 point of contact f
More investment into improvement in existing housing, More investment into improvement in existing housing, More investment into improvement in existing housing, Develop more near patient testing Use tele-care to provide 24/7 risk management, Use tele-care to provide 24/7 risk management, More investment into existing housing, Expand intermediate level services
More extra care (new) houses More extra care (new) houses More extra care (new) houses Improve referral management by Use tele-medicine & tele-health to support care delivery Use tele-medicine & tele- More extra care (new) houses Better community transport
Redesign home care services Use tele-care to provide 24/7 risk management, Redesign home care Understand and reduce variation in health and social care Multi-disciplinary extended community teams Anticipatory care and crisis prevention. Redesign home care services Voluntary sector organisations contributions
Use tele-care to provide 24/7 risk management, Use tele-medicine & tele-health to support care delivery Use tele-care to provide 24/7 risk management, Redesign care pathways to optimise capacity Single 24/7 point of contact for local information and access to community services Multi-disciplinary extended community teams Use tele-care to provide 24/7 risk management, Continuity of information across organisational boundaries.
Use tele-medicine & tele-health to support care delivery Anticipatory care and crisis prevention. Use tele-medicine & tele-health to support care delivery Reduce pre-operative beddays Overnight response for people in need Robust community emergency and urgent response systems Use tele-medicine & tele-health Align health and social care terms and conditions of service
Self directed support Case manager or key worker to coordinate personalised care Self directed support Improve quality of health & social care Expand intermediate level services to provide alternatives to admission to acute hospitals Develop more near patient testing Self directed support Better management of age transitions
More domiciliary assessment and rehabilitation Single 24/7 point of contact for local information Anticipatory care and crisis prevention. Change referral permissions so that people can self refer Robust community emergency and urgent response systems Better community transport More domiciliary assessment and rehabi Redesign care pathways to optimise capacity
Anticipatory care and crisis prevention. Overnight response for people in need Case manager or key worker Screening, consultation & treatment by NMAP Develop more near patient testing Voluntary sector organisations contributions Anticipatory care and crisis prevention. single point of access
Case manager or key worker to coordinate personalised care Expand intermediate level services to provide alternatives to admission Multi-disciplinary extended community teams including carers and users. Equitable funding for each CHP Integrated equipment library and adaptations service Mentoring, peer support/ expert patients to encourage self-care Case manager or key worker Develop community hospitals/local care centres/hubs
Single 24/7 point of contact for local information Robust community emergency and urgent response systems Single 24/7 point of contact for local information Better medicines management by pharmacists Co location of services and teams across agencies Multi-disciplinary extended community teams Pool budgets between health and social care
Overnight response for people in need Integrated equipment library Overnight response for people in need Redesign care pathways Improve referral management Overnight response Develop multi-skilled generic workers
Develop more near patient testing Joint targeting of resources towards those people who are at risk Expand intermediate level services Improve quality and standardisation of routine health & social care through use of protocols Redesign care pathways to optimise capacity Expand intermediate level services Equitable funding for each CHP
Integrated equipment library and adaptations service Voluntary sector organisations contributions Robust community emergency and urgent response systems Non medical prescribing within protocols for common conditions Electronic prescribing and postal dispensing Develop more near patient testing
Self-held personal care plans/records Continuity of information. Better community transport Change referral permissions Mobile services Integrated equipment
User participation in care planning Better medicines management by pharmacists Integrated equipment library and adaptations service Screening, consultation & treatment by non medical practitioners Obligate networks between remote and rural areas and larger centres User participation in care planning
Joint targeting of resources towards those people who are at risk Understand and reduce variation in health and social care Self-held personal care plans/records Better access to psycho-social support Equitable funding for each CHP Voluntary sector organisations
Voluntary sector organisations contributions Screening, consultation & treatment by non medical practitioners User participation in care planning Integrated services across health and social care with single point of access Continuity of information.
Mentoring, peer support/ expert patients to encourage self-care Community based one stop shops/ ‘fast’ clinics Joint targeting of Community based one stop shops/ ‘fast’ clinics Increase clinical and social networks
Better medicines management by pharmacists Mobile services to support community hospitals Voluntary sector organisations contributions Equitable funding for each CHP community including acute hospital costs Redesign care pathways to optimise capacity
Redesign care pathways to optimise capacity Plan EOL care with family and carers with particular focus on last 48 hrs Continuity of information across organisational boundaries. Non medical prescribing within protocols
Non medical prescribing within protocols for common conditions Develop community hospitals/local care centres/hubs Increase clinical and social network effectiveness Better access to psycho-social support
Electronic prescribing and postal dispensing Equitable funding for each CHP Mentoring, peer support/ expert patients to encourage self-care Extend gold standard EOL care to everyone
Plan EOL care with family and carers with particular focus on last 48 hrs Align health and social care terms and conditions of service Plan EOL care with family and carers
Develop multi-skilled generic workers working across organisations Co location of services and teams across agencies Equitable funding for each CHP
Equitable funding for each CHP Better management of age transitions
Better medicines management by pharmacists
Understand and reduce variation in health and social care
Redesign care pathways to optimise capacity
Improve quality of routine health & social care
Non medical prescribing within protocols
Better access to psycho-social support
with single point of access
Community based one stop shops/ ‘fast’ clinics
Mobile services
Plan EOL care with family and carers
Develop community hospitals/local care centres/hubs
Pool budgets between health and social care
Develop multi-skilled generic
140 + things to do at once
Pool budgets
Self referral
Self Directed support
24/7 local information
Non medical prescribing
Anticipatory care reducing crises
Local careCentres/hubs
Userparticipation
Continuity of information
Redesignedhome care
Existing housingadaptations
Extended Comm teams
Referralmanagement
MentoringPeer supportUrgent care
response
Targetingresources
EOLplanning
Telecare Domiciliary assess
& rehab
One stop shopsFast clinics
Generic workers
Case management
Co-location Near patienttesting
Intermediatecare alternatives
Home careredesign
redesign carepathways
Enhance carersupport
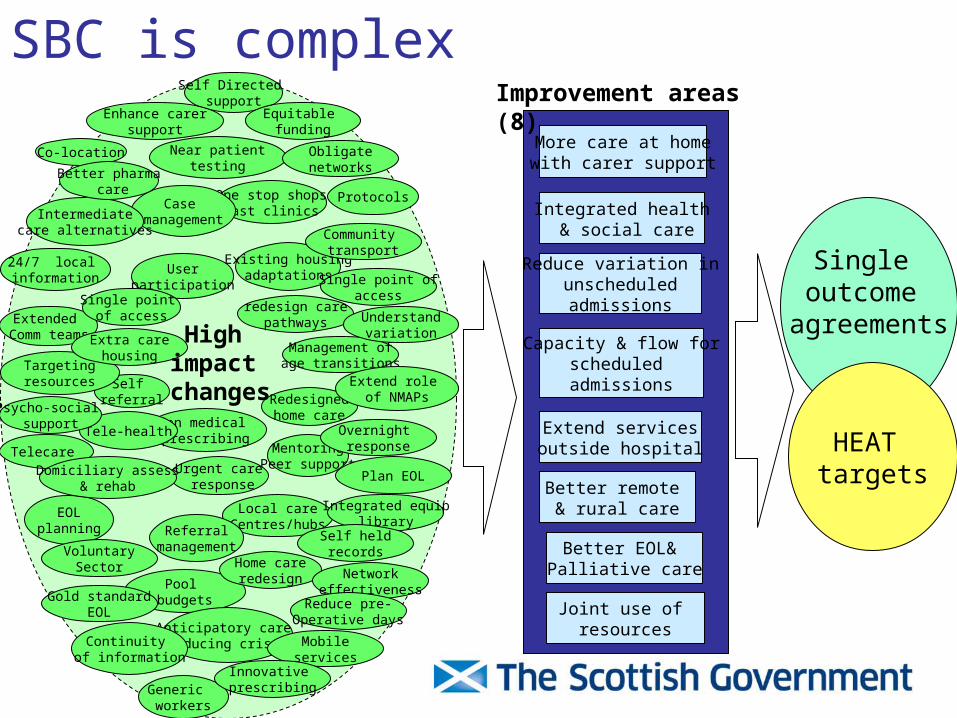
SBC is complex
More care at home with carer support
Integrated health & social care
Reduce variation inunscheduledadmissions
Capacity & flow forscheduled admissions
Extend servicesoutside hospital
Better remote & rural care
Better EOL& Palliative care
Joint use of resources
Improvement areas (8)
Single outcome
agreements
HEAT targets
Single point of access
Tele-health
Better pharma care
Obligatenetworks
Community transport
Single point ofaccess
Management ofage transitions
Extra carehousing
High impact
changes
Overnight response
Integrated equiplibrary
Self heldrecordsVoluntary
Sector Networkeffectiveness
Reduce pre-Operative days
Mobileservices
Innovative prescribing
Equitable funding
Understandvariation
Protocols
Gold standardEOL
Plan EOL
Psycho-social support
Extend role of NMAPs
SBC changes are generic
1.Apply to health, social care, housing, and transport
2.Apply to several improvement areas
3.Are inter-dependent
4.Apply to any age group
5.Apply to any disease or dependency
Implementing change
Actions for communities
• Describe baseline position in relation to 8 improvement areas
• Outline actions that will lead to measurable changes in locally selected areas of Improvement and Resource Framework
• Demonstrate clear line of sight into workforce development plans, eHealth and eCare strategies and infrastructure investment plans
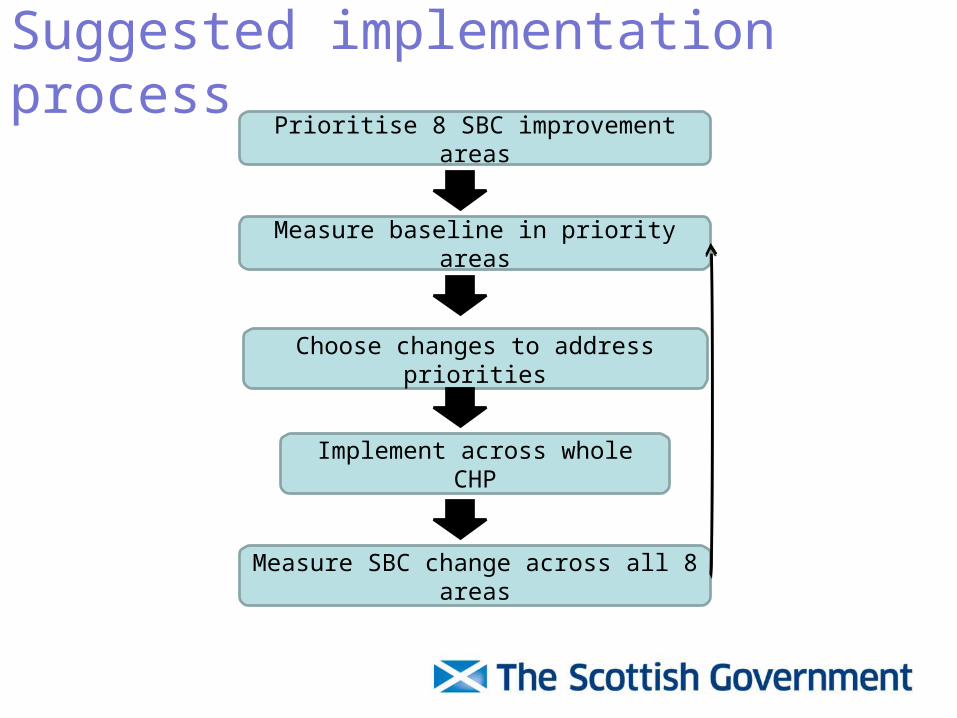
Suggested implementation process
Measure baseline in priority areas
Prioritise 8 SBC improvement areas
Choose changes to address priorities
Implement across whole CHP
Measure SBC change across all 8 areas
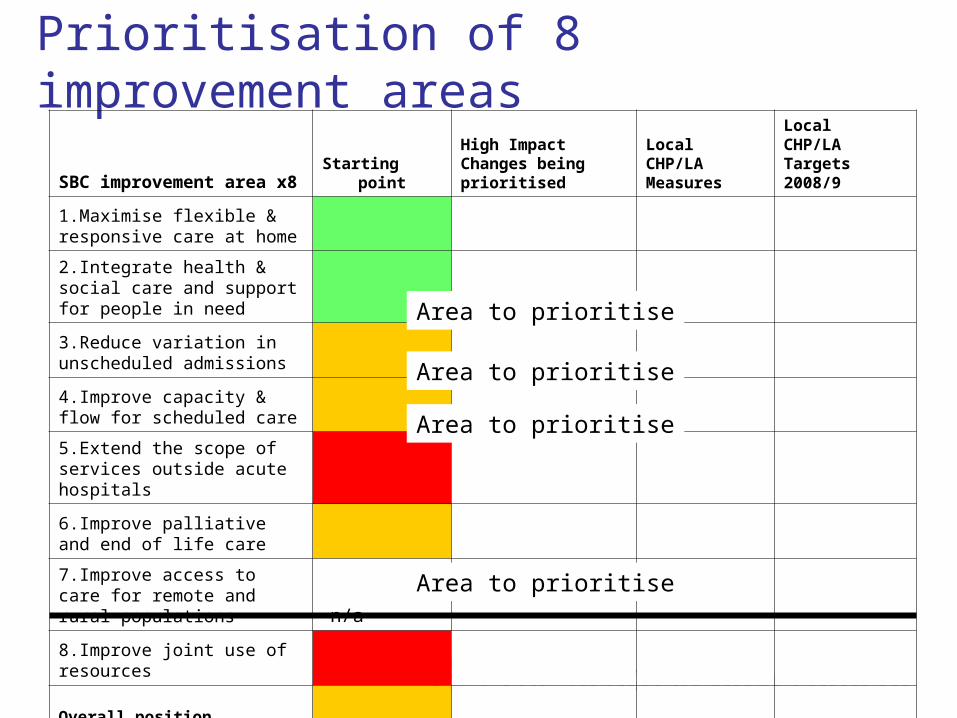
Prioritisation of 8 improvement areas
SBC improvement area x8 Starting pointHigh Impact Changes being prioritised
Local CHP/LA Measures
LocalCHP/LA Targets 2008/9
1.Maximise flexible & responsive care at home
2.Integrate health & social care and support for people in need
3.Reduce variation in unscheduled admissions
4.Improve capacity & flow for scheduled care
5.Extend the scope of services outside acute hospitals
6.Improve palliative and end of life care
7.Improve access to care for remote and rural populations n/a
8.Improve joint use of resources
Overall position
Area to prioritise
Area to prioritise
Area to prioritise
Area to prioritise
Sylvia WyattSPACE lead for SBC
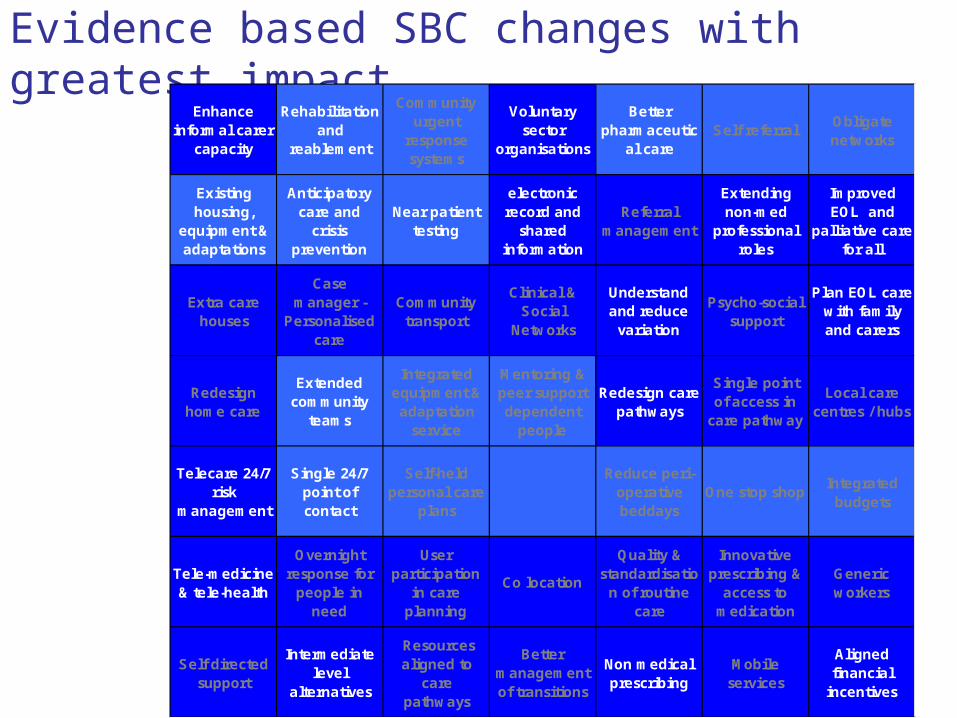
Evidence based SBC changes with greatest impactEnhance
informal carer capacity
Rehabilitation and
reablement
Community urgent
response systems
Voluntary sector
organisations
Better pharmaceutic
al careSelf referral
Obligate networks
Existing housing,
equipment & adaptations
Anticipatory care and
crisis prevention
Near patient testing
electronic record and
shared information
Referral management
Extending non-med
professional roles
Improved EOL and
palliative care for all
Extra care houses
Case manager -
Personalised care
Community transport
Clinical & Social
Networks
Understand and reduce
variation
Psycho-social support
Plan EOL care with family and carers
Redesign home care
Extended community
teams
Integrated equipment & adaptation
service
Mentoring & peer support dependent
people
Redesign care pathways
Single point of access in
care pathway
Local care centres / hubs
Telecare 24/7 risk
management
Single 24/7 point of contact
Self-held personal care
plans
Reduce peri-operative beddays
One stop shopIntegrated
budgets
Tele-medicine & tele-health
Overnight response for
people in need
User participation
in care planning
Co location
Quality & standardisatio
n of routine care
Innovative prescribing &
access to medication
Generic workers
Self directed support
Intermediate level
alternatives
Resources aligned to
care pathways
Better management of transitions
Non medical prescribing
Mobile services
Aligned financial
incentives

Which of these....?
• Addresses priority improvement areas•Fits with local population needs•Addresses inequalities•Improves patient experience
Implement changes across whole system

implement across whole partnership
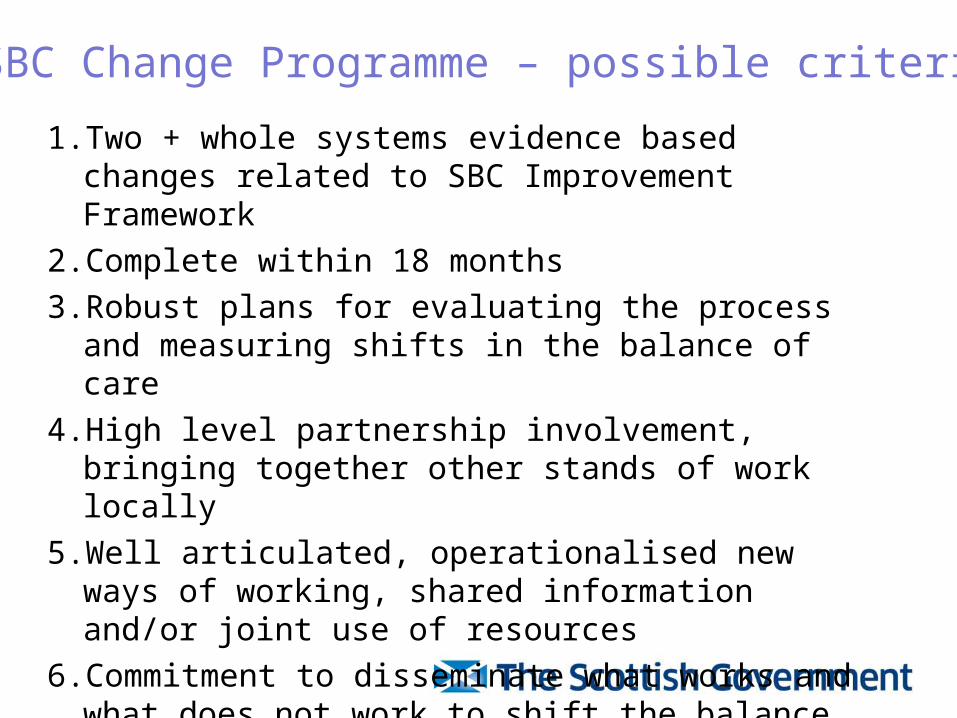
1. Two + whole systems evidence based changes related to SBC Improvement Framework
2. Complete within 18 months
3. Robust plans for evaluating the process and measuring shifts in the balance of care
4. High level partnership involvement, bringing together other stands of work locally
5. Well articulated, operationalised new ways of working, shared information and/or joint use of resources
6. Commitment to disseminate what works and what does not work to shift the balance of care
7. Supports the delivery of HEAT targets and SOAs
SBC Change Programme – possible criteria
Top Related