







Languages
Pages
Legal


Welcome Back From Lunch

Thursday Afternoon
2:00-3:00 Studies of Diagnostic Test Accuracy (Tom)
3:00-3:45 Combining Tests (Mark)3:45-4:00 Break4:00-5:30 Small Groups6:00 Meet in 6702 to head to
Giants game

Studies of Diagnostic Test Accuracy: Outline
Diagnostic accuracy study checklist Understanding specific biases
Incorporation Spectrum Verification Double gold standard
Example: Does ability to hop without pain rule out appendicitis in children?

Checklist
Was there an independent, blind comparison with a reference (“gold”) standard of diagnosis?
Was the diagnostic test evaluated in an appropriate spectrum of patients (like those in whom we would use it in practice)?
Was the reference standard applied regardless of the diagnostic test result?
Was the test (or cluster of tests) validated in a second, independent group of patients?
From Sackett et al., Evidence-based Medicine,2nd ed. (NY: Churchill Livingstone), 2000. p 68

Beyond the Checklist
Consider not only possibility of bias, but WHY if may occur and DIRECTION Incorporation bias Spectrum bias Verification bias Double gold standard bias

Incorporation Bias
When the test itself can be incorporated into the gold standard
Prevented by blinding

Gold standard: determination of CHF by two cardiologists blinded to BNP
“The best clinical predictor of congestive heart failure was an increased heart size on chest roentgenogram (accuracy, 81 percent)”
Is there a problem with assessing accuracy of chest x-rays to diagnose CHF in this study?
Example: Study of BNP as a test for congestive heart failure (CHF)*
*Maisel AS, Krishnaswamy P, Nowak RM, McCord J, Hollander JE, Duc P, et al. Rapid measurement of B-type natriuretic peptide in the emergency diagnosis of heart failure. N Engl J Med 2002;347(3):161-7. Problem 4.3

Cardiologists not blinded to Chest X-ray
Used (incorporated) Chest x-ray for CHF diagnosis
Incorporation bias for assessment of Chest X-ray, not BNP
Incorporation bias

Spectrum of Disease and Nondisease
Disease is often easier to diagnose if severe
“Nondisease” is easier to diagnose if patient is well than if the patient has other diseases

Spectrum Bias
Sensitivity depends on the spectrum of disease in the population being tested.
Specificity depends on the spectrum of non-disease in the population being tested.
Example: Absence of Nasal Bone (on 13-week ultrasound) as a Test for Chromosomal Abnormality

Spectrum Bias Example: Absence of Nasal Bone as a Test for Chromosomal Abnormality*
Sensitivity = 229/333 = 69%BUT the D+ group only included fetuses with
Trisomy 21
Nasal Bone Absent D+ D- LR
Yes 229 129 27.8No 104 5094 0.32
Total 333 5223
Cicero et al., Ultrasound Obstet Gynecol 2004; 23: 218-23

D+ group excluded 295 fetuses with other chromosomal abnormalities (esp. Trisomy 18)
Among these fetuses, sensitivity 32% (not 69%)
What decision is this test supposed to help with? If it is whether to test chromosomes using
chorionic villus sampling or amniocentesis, these 295 fetuses should be included!
Spectrum Bias: Absence of Nasal Bone as a Test for Chromosomal Abnormality

Sensitivity = 324/628 = 52%NOT 69% obtained when the D+ group only included
fetuses with Trisomy 21
Spectrum Bias:Absence of Nasal Bone as a Test for Chromosomal Abnormality, effect of including other trisomies in D+ group
Nasal Bone Absent D+ D- LR Yes 229 + 95 =324 129 20.4No 104 + 200=304 5094 0.50Total 333 + 295=628 5223

Verification bias: Example Visual assessment of
jaundice in newborns Study patients who are getting
a bilirubin measurement Ask clinicians to estimate
extent of jaundice at time of blood draw

Visual Assessment of jaundice*: Results
*Moyer et al., Archives Pediatr Adol Med 2000; 154:391
Sensitivity of jaundice below the nipple line for bilirubin ≥ 12 mg/dL = 97%
Specificity = 19%
What is the problem?
Editor’s Note: The take-home message for me is that no jaundice below the nipple line equals no bilirubin test, unless there’s some other indication.
--Catherine D. DeAngelis, MD

Verification Bias*
Inclusion criterion for study: gold standard test was done in this case, blood test for bilirubin
Subjects with positive index tests are more likely to be get the gold standard and to be included in the study clinicians usually don’t order blood test for
bilirubin if there is little or no jaundice How does this affect sensitivity and
specificity?
*AKA Work-up, Referral Bias, or Ascertainment Bias

Verification Bias Effects
TSB >12 TSB < 12
Jaundice below nipple
a b
No jaundice below nipple
c d
Sensitivity, a/(a+c), is biased ___.
Specificity, d/(b+d), is biased ___.
*AKA Work-up, Referral Bias, or Ascertainment Bias

Visual Assessment of jaundice*: Results
*Moyer et al., Archives Pediatr Adol Med 2000; 154:391
Recall “Gold Standard” was bilirubin ≥ 12 mg/dL Specificity = 19% This low specificity was a clue! What does it
mean? NIH: 19% of newborns who don’t have a bilirubin
≥ 12 mg/dL are not jaundiced below the nipple line
81% of babies with bilirubin <12 mg/dL are jaundiced below the nipple line
Copyright restrictions may apply.
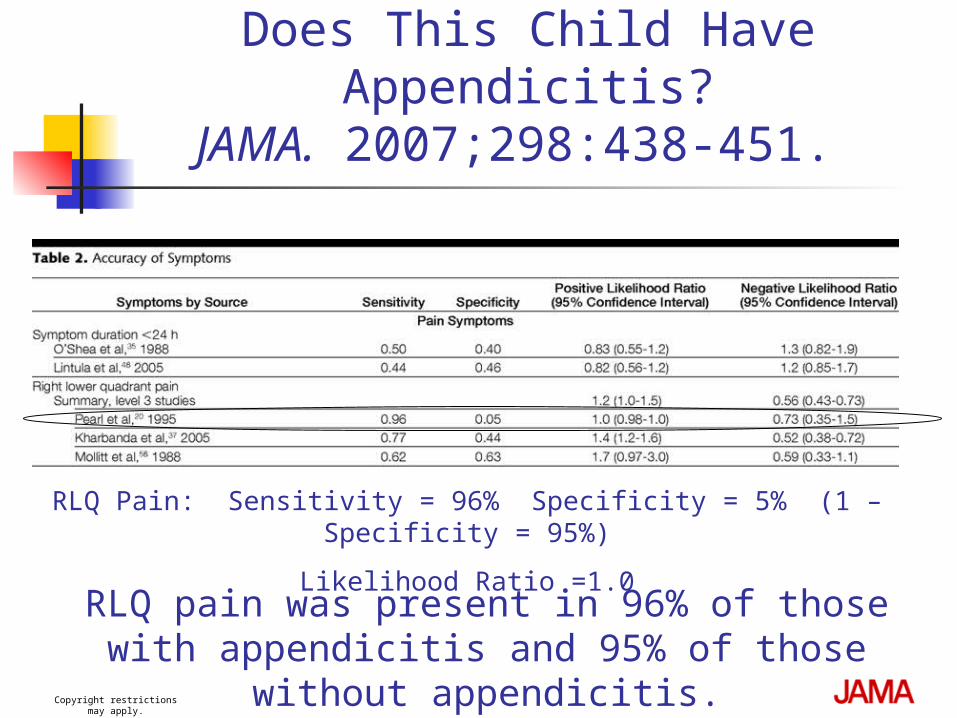
Does This Child Have Appendicitis?
JAMA. 2007;298:438-451.
RLQ Pain: Sensitivity = 96% Specificity = 5% (1 – Specificity = 95%)
Likelihood Ratio =1.0RLQ pain was present in 96% of those with
appendicitis and 95% of those without appendicitis.

Double Gold Standard Bias-1*
Two different “gold standards” One gold standard (e.g., surgery, invasive test)
is more likely to be applied in patients with positive index test
Other gold standard (e.g., clinical follow-up) is more likely to be applied in patients with a negative index test.
*AKA Differential verification bias

Double Gold Standard Bias- 2 There are some patients in whom the
two “gold standards” do not give the same answer Spontaneously resolving disease
(positive with immediate invasive test, but not with follow-up)
Newly occurring or newly detectable disease (positive with follow-up but not with immediate invasive test)

Double Gold Standard Bias, example
Study Population: All patients presenting to the ED who received a V/Q scan
Test: V/Q Scan Disease: Pulmonary embolism (PE) Gold Standards:
1. Pulmonary arteriogram (PA-gram) if done (more likely with more abnormal V/Q scan)
2. Clinical follow-up in other patients (more likely with normal VQ scan)
What happens if some PE resolve spontaneously?
*PIOPED. JAMA 1990;263(20):2753-9.

Effect of Double Gold Standard Bias 1: Spontaneously resolving disease
Test result will always agree with gold standard Both sensitivity and specificity increase Example: Joe has a small pulmonary embolus
(PE) that will resolve spontaneously. If his VQ scan is positive, he will get an
angiogram that shows the PE (true positive) If his VQ scan is negative, his PE will resolve
and we will think he never had one (true negative)
Joe’s VQ scan can’t be wrong!
Effect of Double Gold Standard Bias 2: Newly occurring or newly detectable disease
Test result will always disagree with gold standard Both sensitivity and specificity decrease Example: Jane has or will soon get a nasty breast
cancer that is currently undetectable If her mammogram is positive, she will get biopsies
that will not find the tumor (mammogram will look falsely positive)
If her mammogram is negative, she will return in several months and we will think the tumor was initially missed (mammogram will look falsely negative)
Jane’s mammogram can’t be right!

Effect of Double Gold Standard Bias
Spontaneously resolving disease
Sensitivity falsely high
Specificity falsely high
Newly occurring or newly detectable disease Sensitivity falsely
low Specificity falsely
low
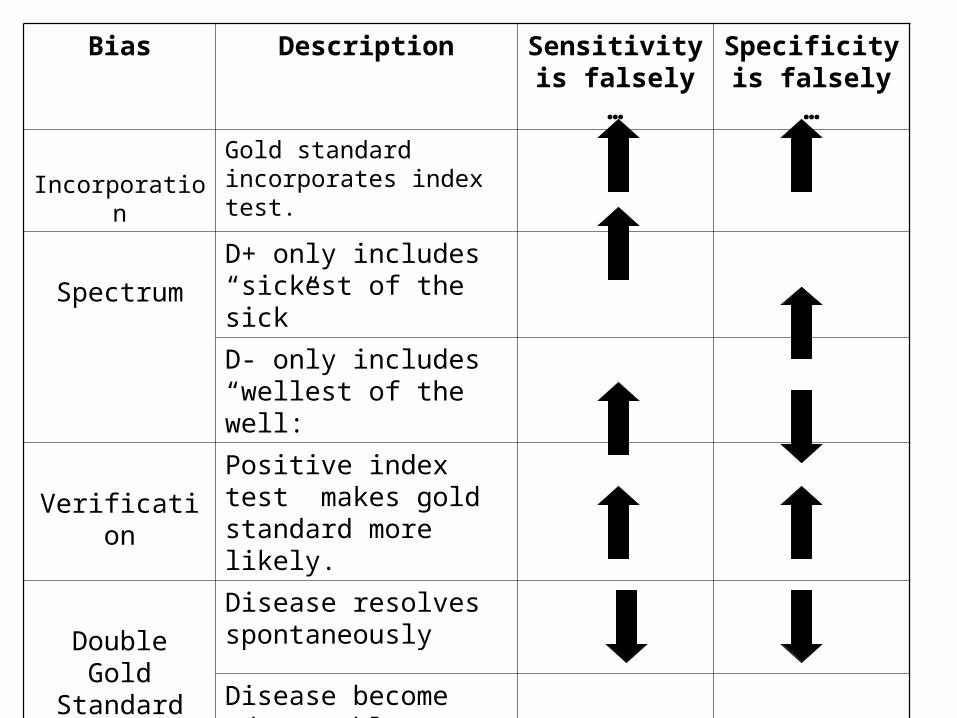
Bias Description Sensitivity is falsely …
Specificity is falsely …
Incorporation
Gold standard incorporates index test.
Spectrum
D+ only includes “sickest of the sick”
D- only includes “wellest of the well:
Verification
Positive index test makes gold standard more likely.
Double Gold Standard
Disease resolves spontaneously
Disease become sdetectable during follow-up

Example: Does ability to hop or jump without pain rule out appendicitis in children?
Kharbanda et al. Pediatrics 2005; 116(3): 709-16

Example: A clinical decision rule to identify children at low risk for appendicitis (Problem 5.6)
Study design: prospective cohort study Subjects
4140 patients 3-18 years presenting to Boston Children’s Hospital ED with abdominal pain
Of these, 767 (19%) received surgical consultation for possible appendicitis
113 excluded (chronic diseases, recent imaging) 53 missed 601 included in the study (425 in derivation set)

A clinical decision rule to identify children at low risk for appendicitis
Predictor variable Standardized assessment by pediatric ED
attending Focus on “Pain with percussion, hopping or
cough” (complete data in N=381) Outcome variable:
Pathologic diagnosis of appendicitis (or not) for those who received surgery (37%)
Follow-up telephone call to family or pediatrician 2-4 weeks after the ED visit for those who did not receive surgery (63%)
Kharbanda et al. Pediatrics 2005; 116(3): 709-16

A clinical decision rule to identify children at low risk for appendicitis
Results: Pain with percussion, hopping or cough
78% sensitivity and 83% NPV seem low to me. Are they valid for me in deciding whom to image?
Kharbanda et al. Pediatrics 2005; 116(3): 709-16

Checklist
Was there an independent, blind comparison with a reference (“gold”) standard of diagnosis?
Was the diagnostic test evaluated in an appropriate spectrum of patients (like those in whom we would use it in practice)?
Was the reference standard applied regardless of the diagnostic test result?
Was the test (or cluster of tests) validated in a second, independent group of patients?
From Sackett et al., Evidence-based Medicine,2nd ed. (NY: Churchill Livingstone),
2000. p 68

In what direction would these biases affect results?
Sample not representative (population referred to pedi surgery)?
Verification bias? Double-gold standard bias? Spectrum bias

For children presenting with abdominal pain to SFGH 6-M Sensitivity probably valid (not
falsely low) But whether all of them tried to hop is
not clear Specificity probably low PPV is too high NPV is too low Does not address surgical
consultation decision
Questions?
Top Related