







Languages
Pages
Legal



Vasculitis

Inflamation and necrosis ofInflamation and necrosis of a a blood vessel with subsequent blood vessel with subsequent impairment of flow.impairment of flow.

VasculitisVasculitis
Large vessel vasculitisLarge vessel vasculitis Giant vessel vasculitisGiant vessel vasculitis
Takayasu vasculitisTakayasu vasculitis
Medium sized vessel vasculitisMedium sized vessel vasculitis Polyarteritis nodosaPolyarteritis nodosa
Kawasaki diseaseKawasaki disease
Small vessel vasculitisSmall vessel vasculitis ANCA associatedANCA associated
None ANCA associatedNone ANCA associated

Takayasu’s arteritis
Takayasu’s arteritis is a chronic inflammatory disorder of unknown etiology
primarily affecting the aorta and its major
branches.
• Occurs most commonly in females under 40
years of age.

Takayasu’s arteritis: clinicalfeatures
Systemic phase: malaise, fever, night sweats
and fatigue. Occlusive phase: upper limb claudication,
headaches, postural dizziness and visual disturbances. Reduced or absent upper limb pulses. Arterial bruits over the carotid, abdominal and
subclavian vessels

Aortic arch arteriogram in a patient with Takayasu’s
arteritis. Smooth taperedstenosis of bilateralcommon carotid arteries(upper arrows) and of theright subclavian artery(lower arrow) can be seen.There is poststenoticdilatation beyond the leftcommon carotid narrowedsegment. Totalinvolvement is seen alongthe length of the rightcommon carotid artery

Giant Cell Arteritis
A vasculitis of unknown etiology occurring primarily in the elderly. Other terms commonly used include temporal arteritis, cranial arteritis and granulomatous arteritis.
Early recognition and treatment can prevent
blindness and other complications due to occlusion or rupture of involved arteries.

Giant Cell Arteritis: ClinicalFeatures
There are a wide range of symptoms, but most
patients have clinical findings related to involved
arteries. Frequent features: fatigue, headaches, jaw
claudication, loss of vision, scalp tenderness, polymyalgia rheumatica and aortic arch syndrome. The ESR is usually highly elevated.
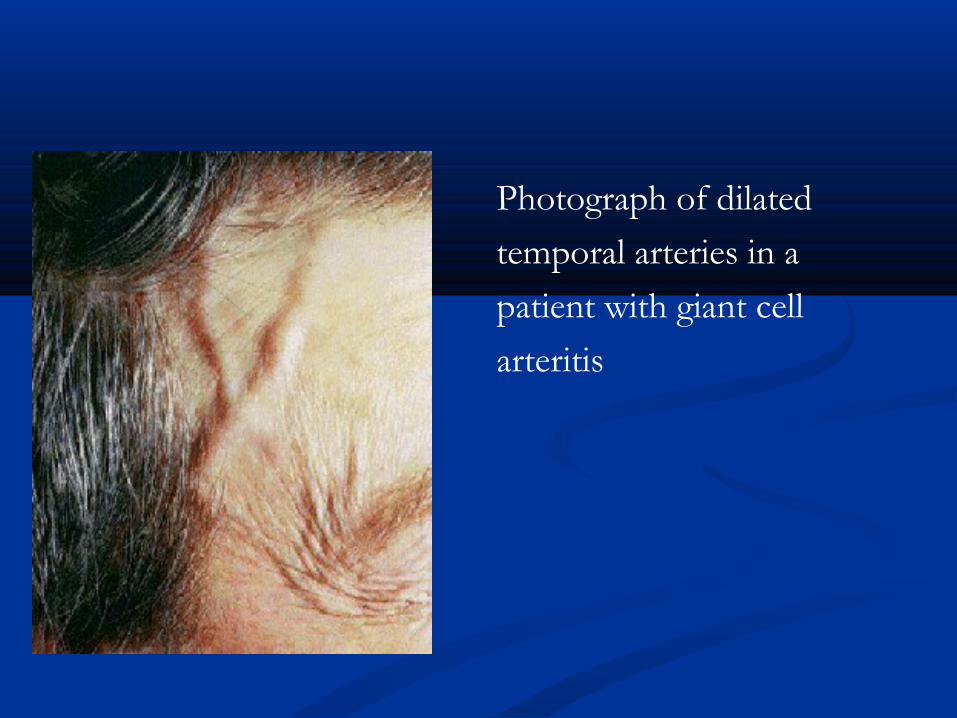
Photograph of dilated
temporal arteries in a
patient with giant cell
arteritis

Polymyalgia Rheumatica
A clinical syndrome of the middle aged and
elderly characterized by pain and stiffness in the neck, shoulder and pelvic girdles, often accompanied by constitutional symptoms.
The musculoskeletal symptoms are usually bilateral and symmetrical
The clinical response to small doses of corticosteroids can be dramatic.

Polyarteritis Nodosa
Small and medium-sized artery inflammation involving the skin, kidney, peripheral nerves, muscle and gut.
Polyarteritis Nodosa: ClinicalFeatures
Constitutional symptoms – fever, anorexia, weight loss. Skin involvement – palpable purpura, infarctions,
livedo reticularis. Arthralgia and arthritis. Peripheral neuropathy and mononeuritis multiplex. Renal involvement – red blood cells and red blood cell
casts, proteinuria, renal insufficiency. Gut involvement – abdominal pain, liver function
abnormalities.
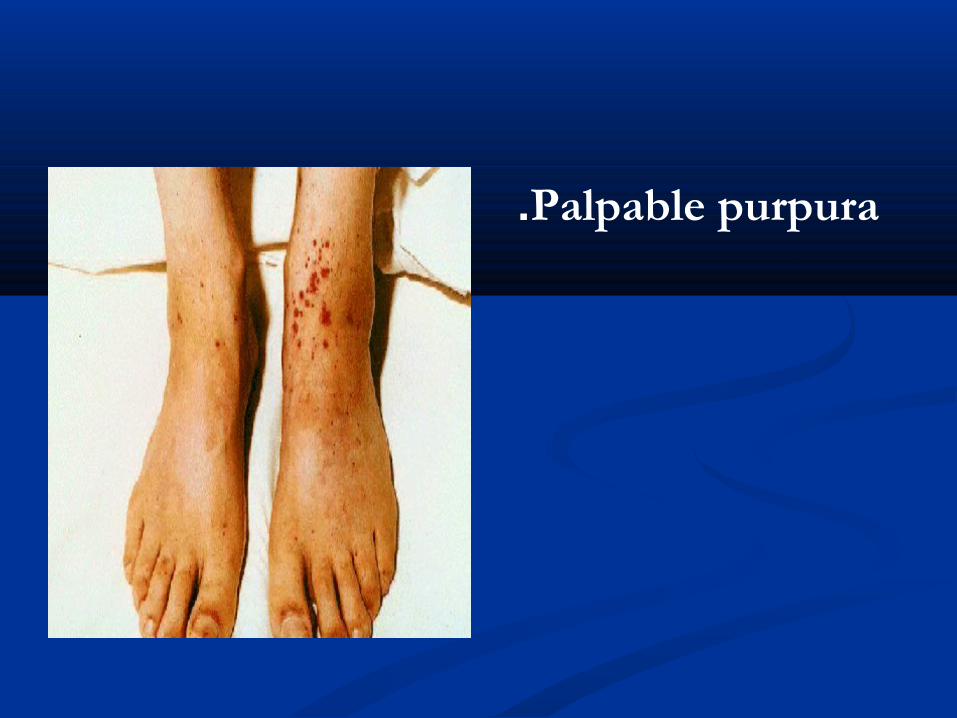
Palpable purpura.

Digital tip infarctions

Wegener’s Granulomatosis
A multisystem disease of unknown etiology with
the following clinicopathologic complex:
• Necrosis, granuloma formation and vasculitis of
the upper and lower respiratory tracts.
• Glomerulonephritis developing in 75% of patients.
• Variable degrees of small and occasionally
medium-sized vessel vasculitis

Wegener’s Granulomatosis:Clinical features
Inflammatory destructive lesions often affect the eyes, ears, nose, throat, lungs, and kidneys.
Although musculoskeletal features are common, they tend to be mild and not destructive. About 25% of cases may have peripheral or central nervous system disease.
The greatest morbidity results from airway, renal, auditory and ocular disease.
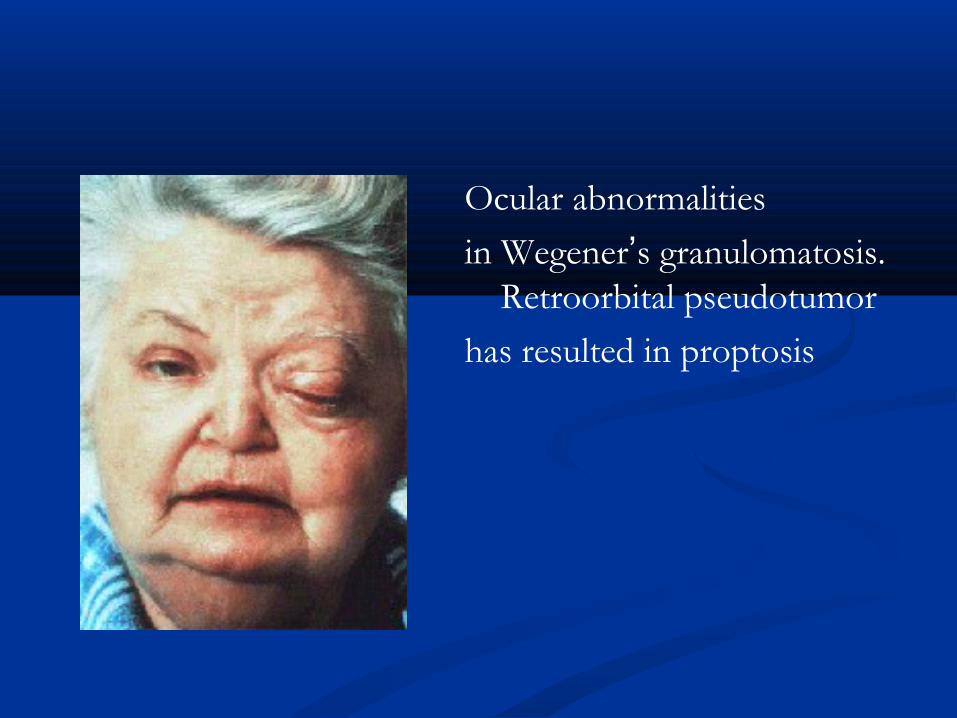
Ocular abnormalities
in Wegener’s granulomatosis. Retroorbital pseudotumor
has resulted in proptosis
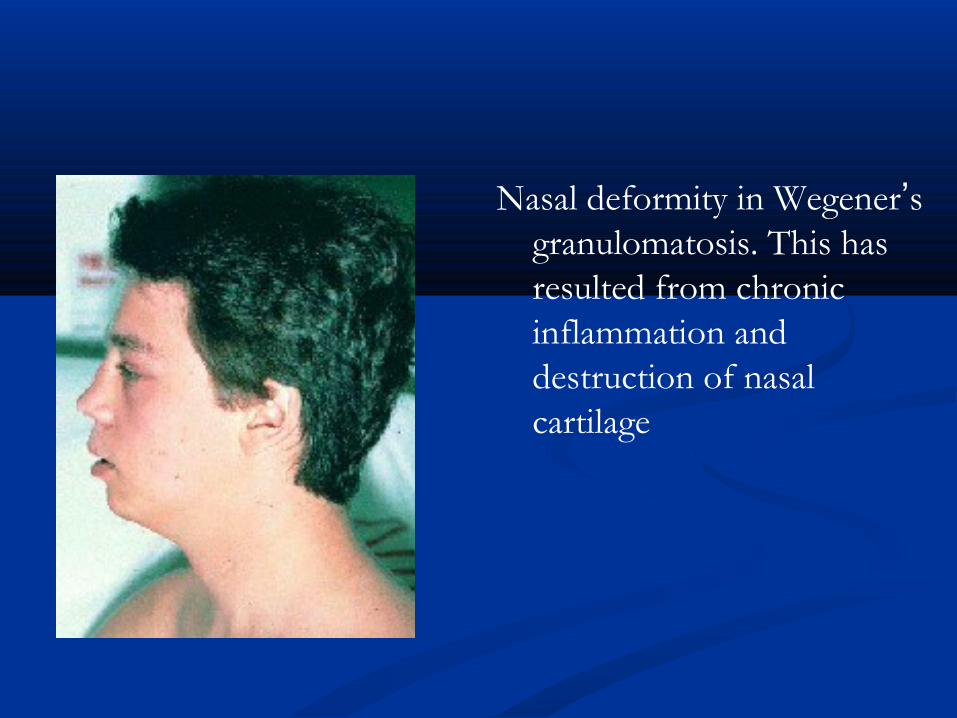
Nasal deformity in Wegener’s granulomatosis. This has resulted from chronic inflammation and destruction of nasal cartilage

Behçet’s Syndrome A systemic vasculitis of unknown cause with
mucocutaneous and frequent ocular and musculoskeletal involvement.
Recurrent oral and/or genital aphthous ulceration. Chronic relapsing uveitis leading to blindness in10% of all cases. A variety of skin manifestations, including the‘pathergy’ phenomenon. Musculoskeletal, neurologic, major artery andvein involvement

Kawasaki Disease
An acute febrile eruptive disease occurring most commonly in infants and children under 5 years of age. • Vasculitis, especially involving coronary arteries, is a serious complication

Kawasaki Disease: ClinicalFeatures
Fever of unknown etiology lasting 5 days or more.
• Bilateral conjunctival congestion.
• Dry and red lips, reddening of oral cavity.
• Acute nonpurulent swelling of the cervical lymph
nodes.
• Polymorphous exanthema of the trunk without
vesicles or crusts.
• Red palms and soles.
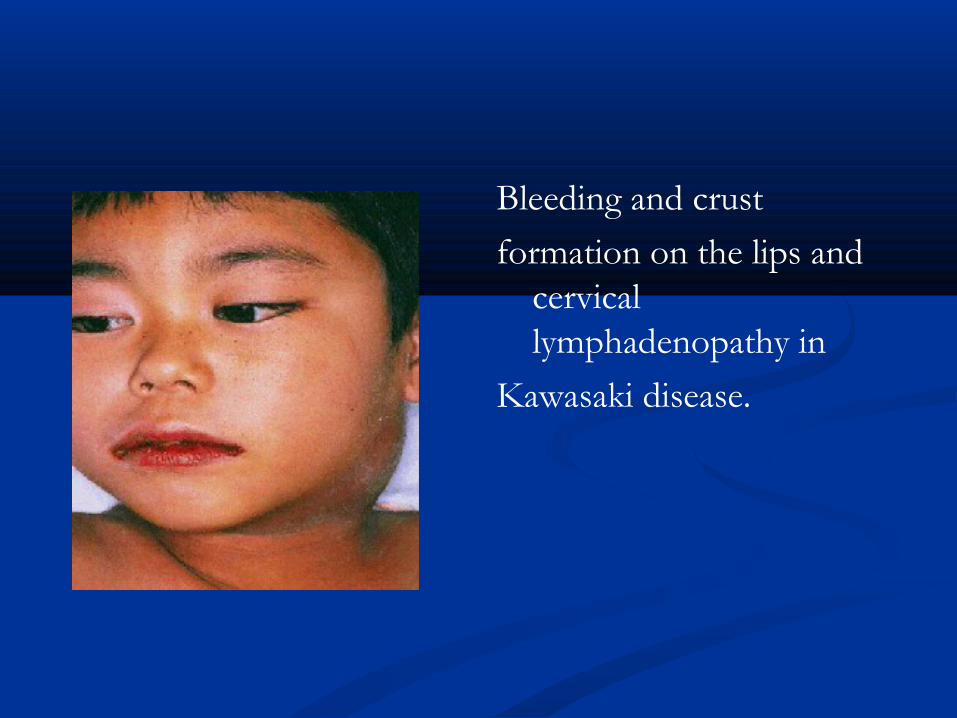
Bleeding and crust
formation on the lips and cervical lymphadenopathy in
Kawasaki disease.

Polymorphous exanthema on the limbs and trunk of an
infant with Kawasaki disease.

TreatmentTreatment
CorticosteroidsCorticosteroids Immunosuppressive drugs such as: Imuran, Immunosuppressive drugs such as: Imuran,
cyclophosphamide, Methotrexate and cyclophosphamide, Methotrexate and Azathioprine. Azathioprine.

THANKSTHANKS
Top Related