







Languages
Pages
Legal


Ulnar and Radial Nerve Entrapment
Anton Sharapov,PGY 3

Anatomic considerations: Ulnar nerve
median cord, C7-T1btw axillary a. and v.medial to arterypierces im septum a->panterior to medial head of triceps

cubital tunnel: med. epicondyle & olecranon, under fibrous arcade of aponeurosis of two heads of FCU.

no branches in armenters forearm btw humeral and ulnarhead of FCU.first branch is articular - behind med epicondyle.next - FCU and medial FDP

Travels on surface of FDP, deep to FCU.accompanied by ulnar a. in distal 2/3.at musculotendinous junction - a. and n. are subcutaneous.palmar branch of ulnar n. - 5-7 cm prox to
wrist, dorsal - 5-10 cm prox to wrist.

Floor - transverse carpal lig to pisiform. Pisiform - ulnar border, hook of hamate - radial border. Roof - volar carpl lig.sup branch - supplies palmaris brevis, skin med palm, two digital n.
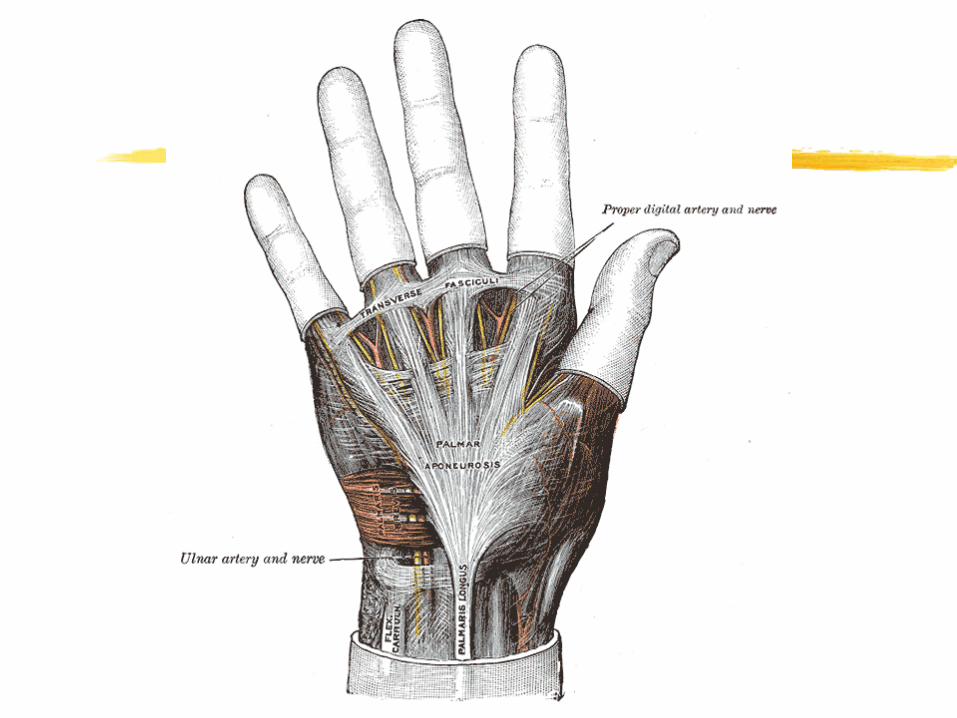


Specifically:
deep terminal - passes around hook -abductor/flex digiti minimi; pierces opponents DM and accompl deep palmar arch dorsal to flexor tendons:

all interosseilumbricals of the ring/small finger,aDDuctor policis,
deep head of the flexor policis brevis. (in some - both heads of FPB and aBDuctor brevis)

entrapment:
at elbow (10 times more)in Guyon's canal

Elbow:2nd to CTS in frequencydescribed 100 years ago

Wide DD:cervical disc diseasepancoast tumorlower trunk brachial plexopathylower motor neuron diseasecompression at Guyon's canal

Surgical indications:if intermittent sx and no motor signs -conservativelyavoid extreme flexion, repetitive flex/ext, leaning.splints, NO steroid (no synovium), role for NSAIDs

surgery - if sx after 3-6/12 on conservative OR sooner if motor sxs. Check: arcade of Struthers, intermuscularseptum, medial epicondyle, two heads of FCU.

Surgical options
in situ decompresssion +/-epicondylectomysc anterior transpositionintramuscular anterior transpositionsubmuscular transposition

id branches of medial antebrachialcutaneous nerve and preserve - or else painful neuromas result

in situ: no transposition ->no risk to devascularisation
epicondylectomy - amount of bone taken off important.
transposition - need to decompress along the entire course (IM, muscular heads)

comparison of in situ, ant sc trans, and epicondylectomy -
no difference in EMGs/strength, better satisfaction for med epicondylectomy.
85-95% success regardless procedure. Recovery continues for 3-5 years, better for sensory then motor sxs.

Poor prognosticators:age>50DMalcoholismmore advanced neuropathy

fare better if no motor involvement, sensory response obtainable, good two point discrimination

complications: scar, neuromas, recurrence, persistent sxs, RSD.

Ulnar tunnel syndrome
trauma to hook of hamate/pisiformrepetitive trauma (hypothenar trauma syndrome)cyclingpisiform instabilitypiso-triquetral arthritisulnar a. thrombosis/ aneurism

Causes cont’d
masses - ganglions, lipomas, neurolemmomas - 32-48%, anomalous muscles - 16%,tendinous bands within canal

sxs - sensory, motor, or bothmay coexist with CTStreat: conservatively -> surgery

Radial n.
posterior cord, C5-T1enters arm btw brachial a/long headaccompanied by deep brachial a. , spirals in the groove behind humeruspasses - btw long-medial, then medial-lat heads - then goes deep to lateral headsinnervates triceps

at distal 1/3 traverses IM septum to enter anterior compartment -> branch to anconeus, joint, brachialis, brachioradialis, ECRL, occasionally ECRBthen passes anterior to the lateral epicondyle/ant joint capsule of elbow: between brachialis/brahioradialis. There it divides into superficial/deep branches

Superficial branch: under cover of BR, on top of supinator, pronator teres, FDS, FPL.
Accompanies radial a. as it emerges from BR, goes to dorsum of the hand (thumb web space)
Deep (post interosseous) - btw humeral/radial heads of supinator.


Deep branch
Passes deep to supinator, close to radial shaft with post interosseous a.lie sandwiched between sup and deep
extensor muscles. Supplies ED, EDM, ECU, EC, EI, ABD policis longus. Then sensory to wrist join from dorsum.
High Radial Neuropathies Proximal to the Spiral Groove
weakness of elbow extensors and wrist extensorsdecreased sensation over the posterior arm and the forearm, weakness and numbness in the distributions of the PIN and SRN.Triceps and BR reflexes may be reduced or absent. Proximal humerus #.

High Radial Neuropathies At, or Distal to, the Spiral Groove
intact elbow extensors and intact posterior arm and forearm sensation; exhibits wrist drop, decreased sensation in the posterolateral hand, weakness in a PIN distribution. The triceps reflex present, BR reflex may be reduced or absent.A common cause is a "Saturday night palsy."

Posterior Interosseus Neuropathies
fingerdropintact sensation in a radial distribution.Wrist drop may be partial with radial deviationThumb abduction and forearm supination may
also be weak. radial reflexes and sensation normal. Common causes include radial tunnel syndrome and Supinator syndrome.

Superficial Radial Neuropathies
Wartenberg syndromedecreased sensation over the posterolateral hand and thumb and the proximal dorsum of the index, middle, and ring fingers. Radial reflexes again should be normal. Common causes include external compression from handcuffs, wristwatches, casts, and penetrating or blunt trauma.
Entrapment at elbow
anatomic variants at the arcade of Frohse: fibrous band at origin at the origin of the supinator, or at the distal end of it.Leash of Henry (arcade of vessels)Tendinous origin of hte ECRBFibrous band from radiocapitellar joint.
mass lesions (rheumatoid synovitis, bicipital bursitis)lateral epicondylitis may have confounding effect

Treatment: conservative initially if no motor involvementrest, avoid aggravation, splint, NSAIDs.splint: writs extended, elbow flexed, Surgery if no supinated - max relief for RTS.improvement after 3-6/12

CLINICAL CONDITIONS THAT MAY PRESENT SIMILARLY TO RADIAL NEUROPATHIES

C7 (and C8) Radiculopathy
presents with weakness in the elbow extensors, wrist extensors, and finger flexors, may have sensory loss over the posterior arm,
forearm, and hand. A radiculopathy is accompanied by neck painradiating down the arm and, in the case of a C7 radiculopathy, into the middle finger

Sensory loss may be less in a C7 radiculopathy than in a radial neuropathy may also involve the palmar surface of the hand and the middle finger. Weakness may also be less severe as only one myotome is affected.

Physical examination may reproduce radiating pain down the upper extremity with provocative tests such as Spurling's maneuver (ipsilateralcervical rotation and extension). The triceps reflex may be reduced in both C7 radiculopathies and radial neuropathiesBR reflex should be normal in a C7 radiculopathy.

EMG is helpful. Imaging studies of the cervical spine to evaluate neural foraminal impingement (OA, DDD)

Posterior Cord Brachial Plexopathy
presents with weakness in elbow, wrist, and finger extensors.

may have weakness in …
shoulder abduction (axillary nerve to deltoid muscle),shoulder internal rotation (axillary
nerve to teres minor, subscapular nerves to subscapularis, and thoracodorsal nerve to latissimus dorsi),and shoulder adduction (thoracodorsalnerve to latissimus dorsi).

impaired sensation over the posterior arm, the forearm, and the hand (radial nerve)……as well as over the lateral shoulder (upper lateral cutaneous nerve of arm, a cutaneous branch of the axillary nerve).

physical examination:
muscle testing of axillary, subscapular, and thoracodorsal-innervated muscles, sensory examination of the lateral shoulder

Deep tendon reflexes in the triceps and BR should be absent in both radial neuropathy and posterior plexopathy.EMGs helpful
Top Related