






Languages
Pages
Legal

The enteric fevers are caused by Salmonella typhi S. paratyphi A and B The bacilli may live in the gallbladder of
carriers for months or years after clinical recovery and pass intermittently in the stool and less commonly in the urine.
faecal-oral route
Rout of transmission
After a few days of bacteraemia, the bacilli localise mainly in the lymphoid tissue of the small intestine.
The typical lesion is in the Peyer's patches and follicles. These swell at first, then ulcerate and ultimately heal, but during this sequence they may perforate or bleed.
Pathology
The incubation period of typhoid fever is about 10-14 days
The onset may be insidious.

After clinical recovery, about 5% of patients become chronic carriers
The bacilli may live in the gallbladder for months or years and pass intermittently in the stool and less commonly in the urine.
Those patients developed chronic gall bladder diseases
The course tends to be shorter and milder than that of typhoid fever .
The onset is often more abrupt with acute enteritis.
The rash may be more abundant.
The intestinal complications less frequent.
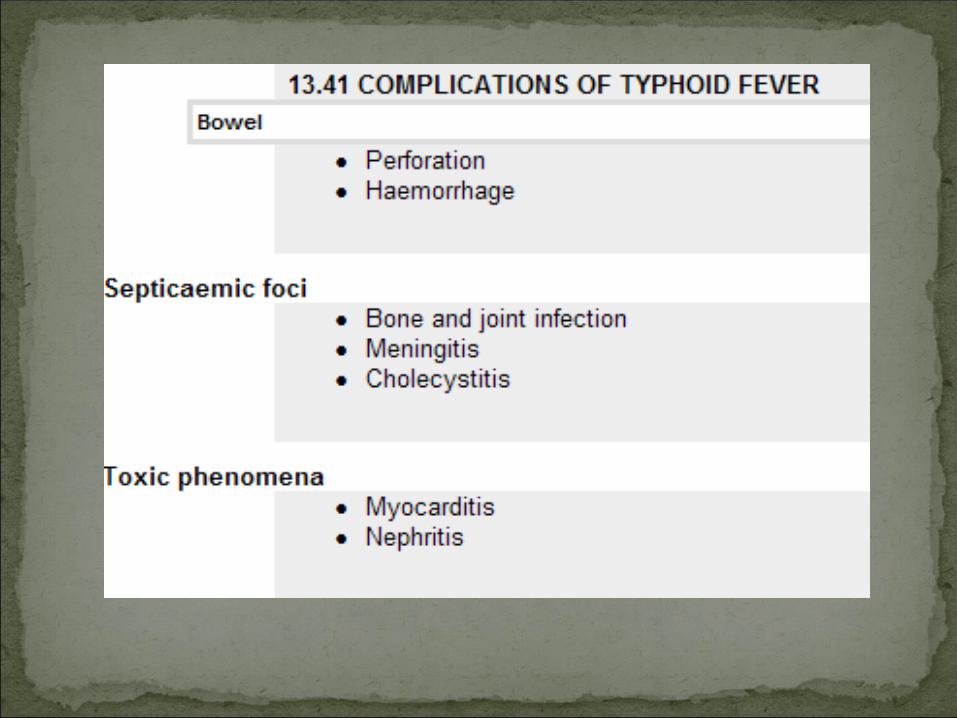
Haemorrhage from the ulcerated Peyer's patches may occur at the end of the 2nd week or during the 3rd week of the illness.
Perforation of Peyer's patches lead to acute peritonitis
A drop in temperature to normal or subnormal levels may be falsely reassuring in patients with intestinal haemorrhage.
Bone and joint infection is common in children with sickle-cell disease.
septicaemia
In the first week the diagnosis may be difficult because in this invasive stage with bacteraemia the symptoms are those of a generalised infection without localising features.
Complete blood count show leucopenia thrombocytopenia anaemia
Blood culture is the most important diagnostic method.
The faeces will contain the organism more frequently during the 2nd and 3rd weeks.
Bone marrow culture
The Widal reaction detects antibodies to the causative organisms.
However, it is not a reliable diagnostic test and should be interpreted with caution.
Chloramphenicol (500 mg 6-hourly), ampicillin (750 mg 6-hourly) amoxicillin (750 mg- 1gm 8 hr ) co-trimoxazole (2 tablets or i.v.
equivalent 12-hourly) are important therapies but are losing
their effect due to resistance in many areas of the world, especially India and South-east Asia
The fluoroquinolones are the drugs of choice (e.g. ciprofloxacin (500 mg 12-hourly) if the organism is susceptible, but resistance is common.
Extended-spectrum cephalosporins (ceftriaxone and cefotaxime) are useful alternatives but have a slightly increased treatment failure rate.
ceftriaxone 1- 2 gm / day IV or IM for 7-10 days Azithromycin (500 mg once daily) is an
alternative where fluoroquinolone resistance is present but has not been validated in severe disease.
Management
Treatment should be continued for 14 days.
Pyrexia may persist for up to 5 days after the start of specific therapy.
Even with effective chemotherapy there is still a danger of complications, and the development of a carrier state.
Chronic carriers are treated for 4 weeks with ciprofloxacin 500 mg twice daily cholecystectomy may be necessary.
Improved sanitation and living conditions reduce the incidence of typhoid.
Travellers to countries where enteric infections are endemic should be inoculated with one of the three available typhoid vaccines
two inactivated injectable and one oral live attenuated
Listeriosis is a serious infection caused by eating foods contaminated with the bacterium Listeria Monocytogenes.
Listeria monocytogenes is an environmental Gram-positive bacillus which can contaminate food.
Outbreaks have been associated with raw vegetables, soft cheeses, undercooked chicken, fish and meat .
This disease affects primarily pregnant women, newborn, and adults with weakened immune systems.
Listeria monocytogenes is a rod-shaped aerobic and gram positive pathogenic bacterium that invades the cytoplasm of living cells. It develops a distinctive rocket tail structure to help push through the cytoplasm.
food-borne outbreaks of gastroenteritis
In pregnancy, listeriosis causes chorioamnionitis, fetal deaths, abortions and neonatal infection.
Meningitis, similar to other bacterial meningitis but with normal CSF glucose, CSF usually shows increased neutrophils.
FeverMuscle acheGI Sx: Nausea, diarrheaPregnant women: mild
flu-like Sx, miscarriage, still birth, premature delivery, or infected newborn.
Lethargyirritability
If infection spreads to the nervous system: headache, stiff neck, confusion, loss of balance, or convulsions.
Listeria can cause Pneumonia, Meningitis, and Sepsis.
Eating food contaminated with Listeria.
Babies can be born with Listeriosis if the mother eats contaminated food during pregnancy.
Listeriosis is generally not contagious from person to person.
There is no routine screening test for susceptibility.
During pregnancy, a blood test is the most reliable way to find out if your Sx are due to Listeriosis.
Diagnosis is made by blood and CSF culture. The organism grows readily in culture media.
Listeriosis is a serious disease requiring hospitilization.Listeriosis is a serious disease requiring hospitilization.A combination of antibiotics is given intravenouslyA combination of antibiotics is given intravenouslyWhen infection occurs during pregnancy, antibiotics must be When infection occurs during pregnancy, antibiotics must be
given promptly to the mother to prevent infection of the fetus or given promptly to the mother to prevent infection of the fetus or newborn.newborn.
The most effective regimen consists of a combination of an intravenous (amoxicillin or ampicillin) plus an aminoglycoside.
Cephalosporins are of no use in this infection, as the organism is inherently resistant
The duration of antibiotic treatment is at least 2 weeks.The duration of antibiotic treatment is at least 2 weeks.Even with prompt treatment, some infections result in death.Even with prompt treatment, some infections result in death.

Top Related