






Languages
Pages
Legal


Tools for Health TeUsing WHO's inte
Tools for Health TeUsing WHO's integ
Technology PackageHealthcare Qua
gTechnology Package
Healthcare QuaHealthcare Quawww.ih
Healthcare Quawww.ih
TomWHO Health Tec
National Project Director KaiseNational Project Director, KaiseAtlanta, G
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
echnology Planning: grated Healthcare
echnology Planning: grated Healthcare ge (iHTP) To Improve lity and Delivery
ge (iHTP) To Improve lity and Deliverylity and Deliveryhtp.infolity and Deliveryhtp.info
m Juddchnology Consultanter Permanente Clinical Technologyer Permanente Clinical TechnologyGeorgia USA
008

AgendaAgendagg
Why iHTP Why iHTP
iHTP Concept and Methodop
iHTP System Overview
Country Implementations witHealthcare Quality and DelivHealthcare Quality and Deliv
iHTP Tool Support
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
logygy
th Impacts on veryvery
008

Wh iHTPWh iHTPWhy iHTP Why iHTP
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
……
008

Process ImprovementProcess Improvement
If you cannot measure something,
t ityou cannot manage it.
If you cannot manage it,
you cannot improve it !
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20008

C t SiC t SiCurrent SiCurrent Si
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
t tit tituation …tuation …
008

Given challengesg
Within WHO technical programsgare known, but rarely linked to te
Program and implementation str Program and implementation strwithout looking at resource plan
Resources are planned and imp
Implementation, training, monito Implementation, training, monitoisolation
Th t t i d ti l di The strategic and operational di
Currently, too many resource pla8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
y, y p
s health needs and priorities (often) ( )echnology planning
rategies have been developedrategies have been developed ning implications
plemented vertically
oring and evaluation often done inoring and evaluation often done in
id i id tvide is evident;
an assumptions008
p

iHTP Concept and MeiHTP Concept and Me
D t i th t t l
pp
Determines the total resources neeservices based on:
P l ti d hi di Population demographics, diseaof pregnancies, number of birthsdiabetes, low birth weight, etc.); , g , );
Health care service targets and pcoverage by 2015; first level carecoverage by 2015; first level care
WHO clinical standards and guidWHO/PAHO set of tools and guiWHO/PAHO set of tools and gui
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
ethodologyethodology
d d t d li d fi d t f
gygy
eded to deliver a defined set of
d h lth fil ( bse and health profile (e.g. number s, prevalence of hypertension,
policy decisions (e.g. universal e to be provided by midwives; etc.);e to be provided by midwives; etc.);
delines (according to the delines)delines).
008

ConceptConcept
Medical
What ? How
Medical Equipment Guidelin
Drugs
HumanResources
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
w ?
HealthP k
How much ?
nes Package
Inter-ventions
Procedure
Facilities
008

Typical Healthcare DelivTypical Healthcare Deliv
Human Resources
c L
evel Facilities
Stra
tegi
cev
eltio
nal L
eO
pera
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
very Scenariovery Scenario
Medical EquipmentPharmaceuticals
008

Gaps analysis in iHTPGaps analysis in iHTPp yp y
Based on the estimated needs upiHTP provides a detail gaps an
d d i d tresources needed in order to starget and quality level.
Focus is on resource planning anp gprescription of clinical practice
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
PP
p against the current situation nalysis of the additional
l i t d i dscale up service to a desired
nd costing and not necessarily on g yes
008

Cost ImplicationsCost Implications
Incorrect specifications and donation provision leads to increased life-cycle costs;increased life-cycle costs;
Risk transferred to recipient;
Cost-benefit often very lowType Impact of
donationAdditional cost (%)
(CAPEX)
Incorrect Specifications High 10-30
Excessive sophistication Medium 20-30
Sub-optimal utilization High 30-80
Lack of spares High 30-50
Excessive downtime High 25-30
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20008

Planning ChallengesPlanning Challengesg gg g
FinancialHP
es
FinancialH
ealth ackageW
hat
reso
urc e
How to deliver
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
ss
008

System OverviewSystem Overview
iHTP Simulation Tool
Sharing of resources
iHTP Simulation Tool
Patient Profiles
iHTP Databases
Country Database
Reference Database
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
Clinical Guidelines
HCT Constraints
Simulations
Simulations and Planning
008

Medical EquipmentMedical Equipment
Comprehensive medical equipment datT h l i t d ti d Technology, maintenance and costing d
usability and technical criticality indicat Separated scenario and reference data
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
tabase (UMDNS based)d tdatatorsbase for improved country implementation
008
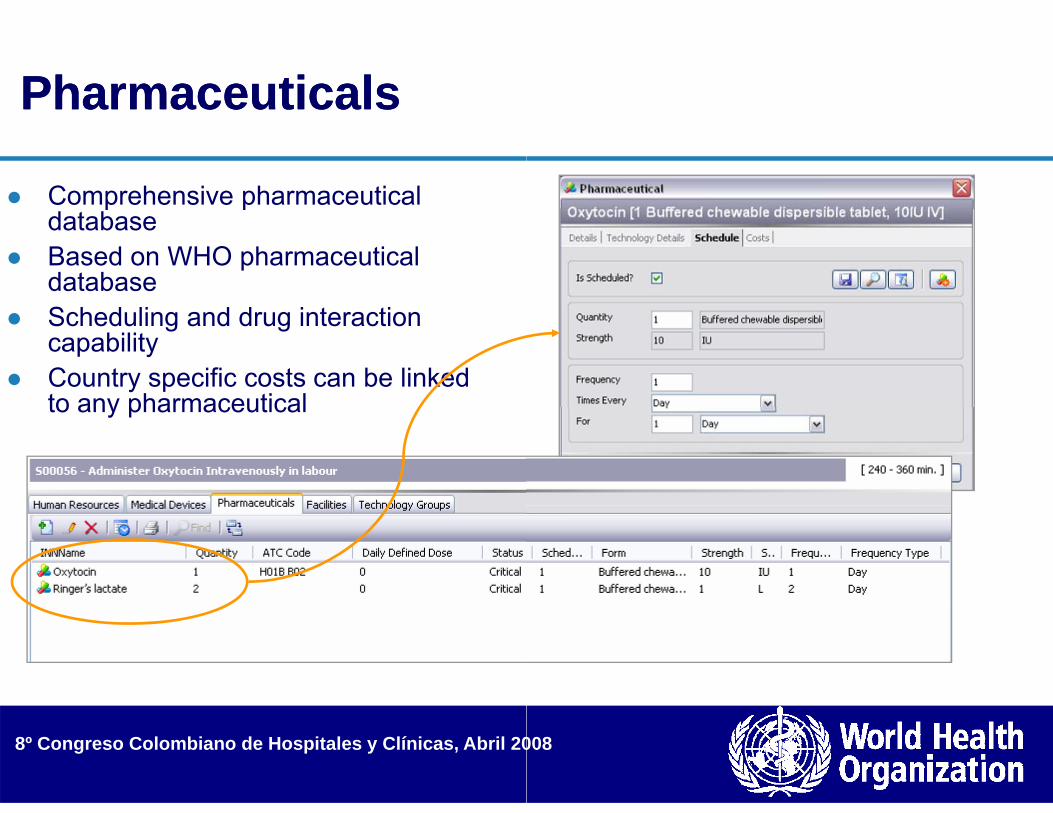
PharmaceuticalsPharmaceuticals
Comprehensive pharmaceutical p pdatabase
Based on WHO pharmaceutical databaseS h d li d d i t ti Scheduling and drug interaction capability
Country specific costs can be linked to any pharmaceuticalto any pharmaceutical
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20008

Clinical guidelinesClinical guidelinesgg
iHTP reference iHTP reference database contains 4500 pre-linked proceduralsprocedurals
Over 600 clinical guidelines (iHTP terminology: scenarios)terminology: scenarios) have been completed and are available on the web
Scenarios can be adapted to any country situationsituation
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20008

Epidemiological profileEpidemiological profileEpidemiological profileEpidemiological profile
Population indicatorsp Coverage rate and
hospital admissions Target indicators (i.e. g (
Caesarean rates) can be model to over specific years
Allows scaling up Allows scaling up
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
eseseses
008

Health package modelHealth package modelgg
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
linglinggg
008

Reports - StaticReports - Static
St ti h lth t h l Static healthcare technology reports (for pharmaceuticals; medical equipment; human resources and facilities)
Can be used for static equipment lists i.e. pedicure equipment procurement; technology scope evaluationgy p
Does not indicate quantity
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20008

Reports - DynamicReports - Dynamicyy
Dynamic healthcare technology ry gycalculation is based on workload
Provides operational costs; dynaiopportunity cost
Takes into consideration healthca
Reports provided “drill down techdrivers
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
reports includes quantities –p qand schedule
mic quantities; recurrent and
are technology availability
hnology” – ideal in evaluating cost
008

Drill-down CapabilityDrill-down Capabilityyy
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20008

Making Pregnancy SafMaking Pregnancy SafMaking Pregnancy SafMaking Pregnancy Saf Routine antenatal care (1st visit) - Prima Routine antenatal care (2nd visit)-Prima Routine antenatal care (3rd visit)-Primar Routine antenatal care (4th visit)-Primar Routine antenatal care (4th visit) Primar Severe anemia in pregnancy - Primary/S STIs and RTIs in pregnancy - Primary/S
Mild l i P i /S d Mild pre-eclampsia - Primary/Secondary Malaria in pregnancy - Primary/Seconda HIV in pregnancy - Primary/Secondaryp g y y y Antenatal infection - Primary/Secondary Routine labor and delivery - Primary/Sec Obstructed labor Primary/Secondary Obstructed labor - Primary/Secondary Antepartum hemorrhage - Primary/Seco Postpartum hemorrhage - Primary/Secon
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
fer (MPS) CPGsfer (MPS) CPGsfer (MPS) CPGsfer (MPS) CPGsary/Secondary ary/Secondary ry/Secondary ry/Secondaryry/SecondarySecondary
Secondaryyary
condary
ndaryndary
008

55 MPS CPGs continued55 MPS CPGs continued55 MPS CPGs, continued55 MPS CPGs, continued
Sepsis in pregnancy - Primary/Secondar Pre-labor rupture of membranes - Prima Eclampsia - Primary/Secondary Fetal distress - Primary/Secondary Fetal distress Primary/Secondary Caesarean section - Primary/Secondary Routine postpartum care - Primary/Seco
P t t f il l i P i /S Postpartum family planning - Primary/Se Postpartum infection - Primary/Secondar Routine newborn care - Primary/Secondy Low birth weight - Primary/Secondary Birth asphyxia - Primary/Secondary Newborn infection Primary/Secondary Newborn infection - Primary/Secondary Newborn malformation - Primary/Second
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
dddd
ryry/Secondary
ondarydecondary
ryaryy
dary
008

Integrated Manageme( C )
Integrated Manageme( C )Illnesses (IMCI)Illnesses (IMCI)
118 WHO Ideal CPGs mapped in 200● Pneumonia, cold, bronchiolitis, croup● Diphtheria, Pertussis (whooping coug● Diarrhea, Dehydration, Dysentery, Ma● Meningitis, Measles, Typhoid Fever, MMeningitis, Measles, Typhoid Fever, M● Otitis Media, UTI, Heart Failure, Hypo● HIV/AIDS in Child, Pneumocystis Car
B F t H d I j i● Burns, Fractures, Head Injuries
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
nt of Childhood nt of Childhood
05, at primary/secondary care levels:pgh), TBalnutrition, Typhoid FeverMalaria , Dengue FeverMalaria , Dengue Fever
othermiarinii Pneumonia (PCP)
008

iHTP VenuesiHTP VenuesiHTP VenuesiHTP Venues Kyrgyzstan and Mozambiqu Namibia, China (PRC), and Ukraine WHO internal programs
● MPS ● IMCI● Surgery, HIV, TB
S l Senegal Mexico, Malawi, and Sri Lan
DRC DRC USA (KP), Lux Developmen
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
ue 2001South Africa 2002
2003
200320052006
20042004nka 2005
20062006nt (several countries) 2007
008

iHTP Impact on HealtiHTP Impact on HealtiHTP Impact on HealtiHTP Impact on Healt Quality: Accelerate health re
infrastructure
Planning: Optimize resource Planning: Optimize resourcehealth providers
C ti C t k i t ti Costing: Cost key interventitechnology investment
HTM: Calculate recurrent coother key health technology
EBM: Use health technologyevidence-based clinical prac
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
p
th Quality & Deliveryth Quality & Deliveryth Quality & Deliveryth Quality & Deliveryeform and developing quality
e planning and utilization bye planning and utilization by
i t d t i b tions to determine best
osts (device maintenance), and management indicators
y performance data to drive ctice and improved quality008
p q y

Kyrgyzstan iHTP ImpaKyrgyzstan iHTP ImpaKyrgyzstan iHTP ImpaKyrgyzstan iHTP Impa
Key objectivesKey objectives
Quality
Costing
Results Databases
● National health resource four databas● National health resource four databas Evidence Based Medicine (EBM)
● Facilitated use of EBM improving qua Clinical Practice Guidelines
● Over 120 CPGs approved by MOH at ● Mapped in iHTP, validated by experts
Anemia/pregnancy, TB, ARI children, Bru
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
actsactsactsacts
ses standardizedses standardized
ality performance
three levels of care s, increased compliance: early focus Hypertensiocellosis
008

Kyrgyzstan Impacts, cKyrgyzstan Impacts, cKyrgyzstan Impacts, cKyrgyzstan Impacts, c
Human Resources Human Resources● More family practice staff identified● Set standards and clarified physicia
D Drugs ● Removed VAT fees for externally p● Developed MoH rules allowing med
h i t il blpharmacies not available● Improved handling of donated drug
Facilities● Improved coordination with local go
and secondary facility renovations Medical Equipment Technology
● National MoH policy for rational use● National policy for purchase of high
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
continuedcontinuedcontinuedcontinued
and trainedan/nurse responsibilities
purchased drugsdical drugs sold at sites where local
gs
overnments assuring funding for primary
y Managemente of medical devices h technology devices
008

Kyrgyzstan iHTP AppKyrgyzstan iHTP AppKyrgyzstan iHTP AppKyrgyzstan iHTP App
EBM CPGs EBM CPGs● Ideal (6): Finnish Lung Health Prog● Actual (6): Acute Bronchitis, Bronc
Acute Respiratory Viral Infection
Gaps Analysis● 5 sites in urban and rural areas, pr● Cost analysis compared for Ideal vy p
• Pre-post provider training sho• Providers began to reduce un• Facilities begin to ensure/sha
Results● MoH began to use ideag
reimbursement throug
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
plicationplicationplicationplication
gram for Adultschial Asthma, TB, COPD, Pneumonia, and
rimary and secondaryversus Actual CPGsowed cost-effectiveness of EBMnnecessary tests, staff, and drugsre vital medical devices for testing
al CPG costs for national gh the Health Insurance Fund
008

Mozambique iHTP ImpMozambique iHTP ImpMozambique iHTP ImpMozambique iHTP ImpKey objective Planning
ImplementationImplementation iHTP Team: Established in MoH Plan Levels/Venues: Primary & secondaryy y CPGs: Focus on MPS, Malaria, TB,
Key FindingKey Finding Demonstrated cost HIV Volunta
USD/encounter, not $11 used Incomplete resource planning (r
access for an important segm
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
pactspactspactspacts
nning Groupy, urban & ruraly,and STD including HIV
ary counseling & testing (VCT) $24 to build 35 rural clinics
re staffing and facilities) delayed ment of this population
008

Namibia iHTP ImpactsNamibia iHTP ImpactsNamibia iHTP ImpactsNamibia iHTP Impacts
Key objectivesy j
Planning
CostingImplementation iHTP Team: Established in MoH Quality Group Levels/Venues: 3 key Rural District Hospitals - p CPGs: Mapped 13 from MPS IMCI Malaria and CPGs: Mapped 13 from MPS, IMCI, Malaria and
Key FindingsDi t i t H it l G A l i District Hospital Gaps Analysisversus Actual CPGs demonstrate
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
ssss
primary/secondaryTBTB
Id l CPG b d ti l: Ideal CPGs based on national normd significant resource efficiencies
008

China iHTP ImpactsChina iHTP ImpactsChina iHTP ImpactsChina iHTP ImpactsImplementation: Fudan University Health Tec Levels/Venues – Tertiary Hospital focus
● 9 tertiary hospitals in 3 large cities in Zhejiang CPGs
● Tertiary level: Gallstones, Stroke● Secondary level: Orthopedics: (1) Fracture lon
protrusion, (3) Open injury of finger, (4) Fractu● Local “Actual” CPGs compared to national “Ide● Local Actual CPGs compared to national Ide
HT Management (HTM)● Conducted Health Technology Audit fo
C t Utili ti F ti lit C• Costs, Utilization, Functionality, Con● Outcomes
• Strengthened HTM system in provinceG l i O th di CPG• Gaps analysis re Orthopedics CPGs a
• Noted links between quality of HTM an• Gave clear direction on how to extend
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
chnology Assessment & Research Center, Shangh
Province ; provincial district hospital
g bone of 4 limbs, (2) Lumbar inter-vertebral disc re of lumbar vertebra
eal” CPGs from Shanghaieal CPGs from Shanghai
or medical devices re:bl HTM t t i t hi tsumables, HTM structure, maintenance history
e, including subsystem for device maintenanced ti lnd national norms
nd health quality and efficiency of care deliveryd the benefits of the project to other provinces
008

South Africa iHTP ImpSouth Africa iHTP ImpSouth Africa iHTP ImpSouth Africa iHTP Imp
Key objectivesy j Planning Costing Calculate recurrent costs and o
Levels/Venues Levels/Venues● Various at district level (prim● Focus on Mother and Child H
Results Wide number of CPGs developed Wide number of CPGs developed Several studies conducted: gaps
technology audit; national health
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
pactspactspactspacts
other key HTM indicators
mary/secondary healthcare)Health (MPS, IMCI), HIV, TB
ddanalysis (MPS); national health technology scoping study
008

Ukraine iHTP ImpactsUkraine iHTP ImpactsUkraine iHTP ImpactsUkraine iHTP Impacts
Mapping of Mother and Child healthMapping of Mother and Child health package
Approximately 30 guidelines – based on observations and recommended clinical practice
Primar and secondar le el of care Primary and secondary level of care
Resource requirements, including operational and recurrent costsoperational and recurrent costs
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
Operational Costs per Year (HR)
Nurse, Professional
8%
Specialist, family doctor71%
Laboratory assistant
21%
Primary Level: Maternal Services (Ukraine)Operational Costs Physical
Infrastructure73.53%
Human Resources
26.29%
Pharmaceutical0.18%
008

Ukraine iHTP ImpactsUkraine iHTP ImpactsUkraine iHTP Impacts Ukraine iHTP Impacts
• Identification of cost drivers• Minimum quantities of resources• Critical path identification
O ti i ti th h id
FURNITURE GENERAL G T
• Optimization through evidence
FURNITURE GENERAL Group TypeBench, {Not Specified} Furniture General Reusable
Desk, {Not Specified} Furniture General Reusable
Racks, Test Tube, {Not Specified} Furniture General Reusable
Cabinets, Laboratory, {Not Specified} Furniture Medical Reusable
Chairs, Office Furniture Medical Reusable
F t t l T /Th St {N t S ifi d} F it M di l R blFootstools, Two/Three-Step, {Not Specified} Furniture Medical Reusable
Tables, Examination/Treatment, Adjustable, Obstetrical, {Not Furniture Medical Reusable
Tables, Instrument, {Not Specified} Furniture Medical Reusable
8
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
- continued- continued- continued- continued
Simulated Total i d
Unit Cost ( i )
Unit Cost ( )
FIXED REPLACE
Qty Required (min) (max) OPER COST COST
0.7 1.0 300.00 394.00 260.71 394.00
2.8 3.0 300.00 320.00 895.37 960.00
0.9 1.0 30.00 35.00 30.66 35.00
0.3 1.0 140.00 160.00 47.05 160.00
4.9 5.0 70.00 90.00 443.97 450.00
0 1 1 0 80 00 120 00 10 79 120 000.1 1.0 80.00 120.00 10.79 120.00
0.1 1.0 5,400.00 12,000.00 1,089.86 12,000.00
0.1 1.0 500.00 600.00 55.59 600.00
9.8 14.0 2,834.02 14,719.00
Ukraine, UAH
008

Mexico iHTP Impacts 2Mexico iHTP Impacts 2Mexico iHTP Impacts 2Mexico iHTP Impacts 2 Mexican Ministry of Health (MoHy (
value in rapid prototyping and cprocess maps of clinical proced
In 2006, CENETEC (The Center fled by biomedical engineer Adriwith a team of 40 engineers phwith a team of 40 engineers, phPAHO had a small team with prpartner, et al.- lead pilot use of ito evaluate care in 2 Mexico CitInsurance Catalog (90 different of charge to Mexico’s significanof charge to Mexico s significan
A CENETEC consultant also be
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
2006200620062006H) deployment demonstrates iHTP ) p y
cost modeling based on using dures and resource databases.
for Excellence in Technology in Healthcare)iana Velazquez, #3 level in MoH,
hysicians etc ) in partnership withhysicians, etc.) in partnership with roject manager and physician iHTP for the perinatal care CPGs (4) ty clinics - as part of the Popular procedures) provided by MoH free t percentage of poor people.t percentage of poor people.
egan Spanish translation of iHTP.
008

Mexico iHTP Impacts 2Mexico iHTP Impacts 2Mexico iHTP Impacts 2Mexico iHTP Impacts 2 In early 2007, the MoH on beh
a national health initiative: “Cacare / outreach clinic allowing - to several of Mexico’s remote- to several of Mexico s remotewere sent throughout all states
C C CENETEC using iHTP assistefor Caravan in this implementadeliver caredeliver care.
Later in 2007, CENETEC alsod l i ll Cli i l P tideveloping all Clinical Practicewith various national experts.
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
2007200720072007half of President Calderon beganaravan” – a traveling primary timely referrals to hospital care
e rural areas 50 Caravanse rural areas. 50 Caravans s of Mexico.
ed the MoH planning departmentation, studying optimal ways to
o gained responsibility for G id li (CPG ) f M He Guidelines (CPGs) for MoH
008

Mexico MoH CaravanMexico MoH CaravanMexico MoH CaravanMexico MoH Caravan Project team: CENETEC Prj
leaders; WHO consultant
Various national physician l Various national physician ldevelopment of 20 evidence● Diabetes Screening
B t C S i● Breast Cancer Screening● 18 from Perinatal Care:
• Prenatal Care visits (4)Pre Eclampsia (4)• Pre-Eclampsia (4)
• Eclampsia (3)• Hemorrhage (4)• Newborn Care (3)• Newborn Care (3)
Completing cost and resource anresults to all MoH primary care (f
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
results to all MoH primary care (f
Project 2007Project 2007 Project - 2007 Project - 2007roject Leader and 2 physician j p y
eaders, assisting witheaders, assisting with e-based CPGs including:
nalysis currently; expected to apply fixed clinics) as well008
fixed clinics) as well

iHTP Tool SupportiHTP Tool SupportiHTP Tool SupportiHTP Tool Support iHTP Help Files (2006) and Tep ( )
iHTP website – www.iHTP.infcapabilities (2007)capabilities (2007)
MPS Resource Kit (individual potential users (2007)potential users (2007)
Ongoing Development of iHTPfor Q&A (2006-present)
Email response guiding user ta espo se gu d g use
Monthly Web Meetings for iHT
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
echnical Manual resource (2007(
fo for New Releases of iHTP
training guide) to train other
P Support Center (South Africa)
to “Knowledge Base” of FAQo o edge ase o Q
TP Users (begun 2007)
008

ThThThanThan
TomTom.juddj
8º Congreso Colombiano de Hospitales y Clínicas, Abril 20
kkk youk you
m [email protected]@ p g
008
Top Related