





Languages
Pages
Legal


Int. J. Radiation Oncology Biol. Phys., Vol. 80, No. 2, pp. 398–402, 2011Copyright � 2011 Elsevier Inc.
Printed in the USA. All rights reserved0360-3016/$–see front matter
jrobp.2010.02.042
doi:10.1016/j.iCLINICAL INVESTIGATION Breast
TIMING OF RADIOTHERAPY AND OUTCOME IN PATIENTS RECEIVINGADJUVANT ENDOCRINE THERAPY
PER KARLSSON, M.D.,* BERNARD F. COLE, PH.D.,yzMARCO COLLEONI, M.D.,xMARIO RONCADIN, M.D.,{
BOON H. CHUA, M.D., PH.D.,k ELIZABETH MURRAY, M.D.,# KAREN N. PRICE, B.S.,**
MONICA CASTIGLIONE-GERTSCH, M.D.,yy ARON GOLDHIRSCH, M.D.,zzxx AND GUNTHER GRUBER, M.D.{{
FOR THE INTERNATIONAL BREAST CANCER STUDY GROUP
*Department of Oncology, Sahlgrenska University Hospital, Gothenburg, Sweden; yDepartment of Mathematics and Statistics,University of Vermont College of Engineering and Mathematical Sciences, Burlington, VT; zInternational Breast Cancer Study GroupStatistical Center, Department of Biostatistics and Computational Biology, Dana-Farber Cancer Institute, Boston, MA; xDepartment ofMedicine, Research Unit in Medical Senology, European Institute of Oncology, Milan, Italy; {Department of Radiotherapy, Centro diRiferimento Oncologico, Aviano, Italy; kDepartment of Radiation Oncology, Peter MacCallum Cancer Centre, Melbourne, Australia;#Department of Radiation Oncology, Groote Shuur Hospital and University of Cape Town, Cape Town, South Africa; **InternationalBreast Cancer Study Group Statistical Center, Frontier Science and Technology Research Foundation, Boston, MA; yyInternationalBreast Cancer Study Group Coordinating Center, Bern, Switzerland; zzEuropean Institute of Oncology, Milan, Italy; xxOncologyInstitute of Southern Switzerland, Bellinzona, Switzerland; {{Institut fuer Radiotherapie, Klinik Hirslanden, Zurich, Switzerland
Reprinogy, UniGothenbu(+46) 31-
PrelimiBreast Co
The Intby the Swence andAustralia,
Purpose: To evaluate the association between the interval from breast-conserving surgery (BCS) to radiotherapy(RT) and the clinical outcome among patients treated with adjuvant endocrine therapy.Patients and Methods: Patient information was obtained from three International Breast Cancer Study Grouptrials. The analysis was restricted to 964 patients treated with BCS and adjuvant endocrine therapy. The patientswere divided into two groups according to the median number of days between BCS and RT and into four groupsaccording to the quartile of time between BCS and RT. The endpoints were the interval to local recurrence, disease-free survival, and overall survival. Proportional hazards regression analysis was used to perform comparisonsafter adjustment for baseline factors.Results: The median interval between BCS and RT was 77 days. RT timing was significantly associated with age,menopausal status, and estrogen receptor status. After adjustment for these factors, no significant effect of a RTdelay #20 weeks was found. The adjusted hazard ratio for RT within 77 days vs. after 77 days was 0.94 (95% con-fidence interval [CI], 0.47–1.87) for the interval to local recurrence, 1.05 (95% CI, 0.82–1.34) for disease-free sur-vival, and 1.07 (95% CI, 0.77–1.49) for overall survival. For the interval to local recurrence the adjusted hazardratio for #48, 49–77, and 78–112 days was 0.90 (95% CI, 0.34–2.37), 0.86 (95% CI, 0.33–2.25), and 0.89 (95% CI,0.33–2.41), respectively, relative to $113 days.Conclusion: A RT delay of #20 weeks was significantly associated with baseline factors such as age, menopausalstatus, and estrogen-receptor status. After adjustment for these factors, the timing of RT was not significantlyassociated with the interval to local recurrence, disease-free survival, or overall survival. � 2011 Elsevier Inc.
Breast cancer, Radiotherapy, Radiotherapy timing, Breast-conserving surgery, Endocrine therapy.
INTRODUCTION
Radiotherapy (RT) to the breast after breast-conserving sur-
gery (BCS) reduces the risk of local recurrence and improves
breast cancer-specific survival (1). The optimal interval be-
tween surgery and the start of RT is not known. Theoretically,
t requests to: Per Karlsson, M.D., Department of Oncol-versity of Goteborg, Sahlgrenska University Hospital,rg S 413 45 Sweden. Tel: (+46) 31-342-2246; Fax:820-114; E-mail: [email protected] results were presented in a poster at the St. Gallennference, St. Gallen, Switzerland, March 2009.ernational Breast Cancer Study Group was funded in partiss Group for Clinical Cancer Research, the Frontier Sci-Technology Research Foundation, the Cancer Councilthe Australian New Zealand Breast Cancer Trials Group
398
the risk of recurrence is related to the density of the clonogenic
cells in the surgical bed. Therefore, a delay between surgery
and the start of RT could increase the likelihood of tumor
cell growth and the development of radioresistance (2). Sev-
eral retrospective studies have yielded variable results (3–8).
(National Health Medical Research Council), the National CancerInstitute (Grant CA-75362), the Swedish Cancer Society, the CancerAssociation of South Africa, and the Foundation for Clinical CancerResearch of Eastern Switzerland (OSKK).
Conflict of interest: none.Acknowledgments—We thank the patients, physicians, nurses, anddata managers who participated in the International Breast CancerStudy Group trials.
Received Oct 9, 2009, and in revised form Feb 3, 2010. Acceptedfor publication Feb 11, 2010.

Table 1. Baseline characteristics
CharacteristicRT within 77 d
(n = 492)RT after 77 d
(n = 472) p*
Age (y) 55.6 � 8.9 58.8 � 7.3 <.0001Menopausal status <.0001
Pre 128 (26) 45 (10)Post 364 (74) 427 (90)
ER status .042Negative 123 (25) 89 (19)Positive 357 (73) 358 (76)Unknown 12 (2) 25 (5)
Tumor grade .941 89 (18) 86 (18)2 237 (48) 221 (47)3 165 (34) 162 (34)Unknown 1 (0) 3 (1)
Positive lymphnodes (n)
.62
0 454 (92) 441 (93)1–3 25 (5) 23 (5)$4 13 (3) 8 (2)
Tumor size (cm) .35#2 371 (75) 366 (78)>2 118 (24) 100 (21)Unknown 3 (1) 6 (1)
Vessel invasion .098No 378 (77) 364 (77)Yes 94 (19) 67 (14)Unknown 20 (4) 41 (9)
Abbreviations: RT = radiotherapy; ER = estrogen receptor.Data presented as number of patients, with percentages in parenthe-
ses, except for age, which is given as mean +/� standard deviation.* Unknown data for given category excluded from calculation of
p values.
Timing of RT for adjuvant breast cancer d P. KARLSSON et al. 399
Generally, on univariate analysis, an increased risk of local
recurrence was observed with a longer delay between surgery
and the start of RT. However, on multivariate analysis, this
effect was not observed. Two systematic reviews showed an
increase in the risk of local recurrence with RT delay of >8
weeks (9, 10). However, these reviews included all subtypes
of breast cancer and a variety of study designs, rendering
interpretation of the results difficult. The risk of local
recurrence in relation to RT delay can vary by breast cancer
subtype and systemic treatment. An International Breast
Cancer Study Group (IBCSG) study has shown that delaying
RT until the completion of chemotherapy did not adversely
affect the treatment outcome (11). No study has examined
the effect of RT delay on local recurrence in breast cancer ex-
clusively in patients receiving endocrine therapy. The aim of
the present study was to investigate the effect of a delay from
BCS to the start of RT in patients treated with endocrine therapy
in three IBCSG trials.
PATIENTS AND METHODS
Patient information was obtained from 1,108 patients who had
undergone BCS and were randomized to selected treatment arms
from IBCSG Trials VII, VIII, and IX. Of the 1,108 patients identi-
fied, 135 did not receive RT and an additional 9 did not have a record
of RT start dates, leaving 964 patients in the analyzed cohort.
Trial VII compared adjuvant tamoxifen alone vs. chemoendocrine
treatment with tamoxifen with concurrent classic cyclophospha-
mide, methotrexate, and 5-fluorouricil (CMF) in postmenopausal pa-
tients with node-positive breast cancer (12). Trial VIII studied
adjuvant ovarian function suppression with luteinizing hormone-
releasing hormone analog for 2 years vs. six courses of CMF vs.
six courses of CMF followed by 18 months of ovarian function sup-
pression in premenopausal patients with node-negative disease (13).
Trial IX compared adjuvant tamoxifen vs. three courses of CMF fol-
lowed by tamoxifen in postmenopausal patients with node-negative
disease (14). The present study was restricted to the following treat-
ment groups receiving adjuvant endocrine therapy: Trial VII, Arm A,
tamoxifen for 5 years (n = 69); Trial VIII, Arm B, luteinizing
hormone-releasing hormone analog for 2 years ((n = 173); Trial
IX, Arm A, tamoxifen for 5 years (n = 374); and Trial IX, Arm B,
CMF�3 followed by tamoxifen for 57 months (n = 370). Trial VII
specified that RT was required for all patients who had undergone
BCS. Although Trials VIII and IX did not mandate RT to the
conserved breast, 88% of the patients who had undergone BCS
were treated with RT. In all three trials, patients who had undergone
BCS and RT and were randomized to receive endocrine therapy
alone were required to begin RT within 3 months of randomization,
and those randomized to receive CMF before tamoxifen in Trial
IX were to begin RT 2 weeks after the end of the last cycle of
chemotherapy.
For the present study, the patients were divided into two groups
according to the median number of days from surgery to the start
of RT. Kaplan-Meier survival curves were plotted for the two
groups, and the log–rank test was used to compare them. The end-
points were the interval to local recurrence, disease-free survival
(DFS), and overall survival (OS), measured from the start of RT.
This approach accounted for how the interval to an event had to
exceed the number of days between surgery and the start of RT.
In addition, the patients were divided into four groups according to
the quartiles of days from surgery until the start of RT. Proportional
hazards regression was used to estimate the hazard ratios (HRs) and
95% confidence intervals (CIs) for the two-group and four-group
analyses following adjustment for baseline factors.. Wald tests
were used to evaluate the heterogeneity among the HRs according
to the four-group analysis. Of the 964 patients in the analytic cohort,
715 had estrogen receptor (ER)-positive disease. All analyses were
repeated for the ER-positive cohort.
RESULTS
The median number of days from surgery to the start of RT
was 77 (mean, 84; standard deviation, 45; range, 14–436). A
total of 409 patients (42%) received RT >90 days after sur-
gery. Table 1 summarizes the baseline characteristics of the
two groups of patients who started RT within or after the me-
dian of 77 days after surgery. Age, premenopausal status, and
hormone receptor status were significantly associated with
RT timing. However, it should be noted that some of these dif-
ferences might have resulted from the CMF-tamoxifen arm of
Trial IX in which patients underwent RT after chemotherapy.
The median follow-up was 10.5 years. The total number of
events was 37 local recurrences, 271 DFS events, and 161
deaths. Adjusting for the differences in baseline characteris-
tics, the HR for starting RT within 77 days relative to after 77
days was 0.94 (95% CI, 0.47–1.87) for local recurrence, 1.05
(95% CI, 0.82–1.34) for DFS, and 1.07 (95% CI, 0.77–1.49)
for OS (Tables 2 and 3). When patients were divided into

Table 2. Adjusted proportional hazards regression resultsdividing at median
RT timing (from surgery) HR 95% CI p
Local recurrence#77 d 0.94 0.47–1.87 .86$78 d 1.00
Disease-free survival#77 d 1.05 0.82–1.34 .73$78 d 1.00
Overall survival#77 d 1.07 0.77–1.49 .67$78 d 1.00
Abbreviations: RT = radiotherapy; HR = hazard ratio; CI = con-fidence interval. Adjustment factors: age, ER status, tumor grade,nodal status, tumor size and vessel invasion status.
Table 4. Adjusted proportional hazards regression resultsaccording to quartiles
RT timing from surgery HR 95% CI p
Local recurrence*#48 d 0.90 0.34–2.37 .8349–77 d 0.86 0.33–2.25 .7678–112 d 0.89 0.33–2.41 .81$113 d 1.00
Disease-free survivaly
#48 d 0.78 0.55–1.10 .1649–77 d 0.95 0.68–1.32 .7578–112 d 0.68 0.47–0.97 .03$113 d 1.00
Overall survivalz
#48 d 0.70 0.45–1.11 .1349–77 d 0.86 0.56–1.31 .4778–112 d 0.50 0.31–0.81 .005$113 d 1.00
Abbreviations as in Table 2.* Overall Wald p = .99.y Overall Wald p = .12.z Overall Wald p = .03. Adjustment factors as in Table 2.
400 I. J. Radiation Oncology d Biology d Physics Volume 80, Number 2, 2011
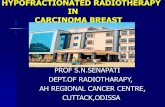
quartiles according to the surgery-to-RT interval, the
adjusted HRs were not significantly different (Tables 4
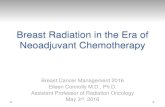
and 5). The Kaplan-Meier curves for the interval to local re-
currence, DFS, and OS with the interval to an event from the
start of RT for the two-group analysis and the four-group
analysis are shown in Figs. 1 and 2, respectively. Kaplan-
Meier analysis with the interval to event measured from
Day 77 after surgery gave similar results (data not shown).
The analyses were repeated for the ER-positive cohort (n =
715), with similar results (Tables 3 and 5), with no significant
interactions found between RT timing and ER positivity (data
not shown).
The mean interval from surgery to the start of endocrine
therapy was 33 days in the group that started RT within 77
days and 81 days in the group that started RT after 77
days. Of the 841 patients (89%) who began endocrine therapy
before RT, the mean interval from the start of endocrine ther-
apy to the start of RT was 26 days in the group that started RT
within 77 days and 48 days in the group that started RT after
77 days.
Table 5. Estrogen receptor-positive cohort: adjustedproportional hazards regression results according to quartiles
RT timing from surgery HR 95% CI p
Local recurrence*#48 d 1.03 0.34–3.14 .9649–77 d 0.67 0.21–2.17 .50
DISCUSSION
After adjustment for differences in the baseline character-
istics, RT timing was not significantly associated with the in-
terval to local recurrence, DFS, or OS in patients receiving
adjuvant endocrine therapy for RT delay of up to about 20
weeks. Postoperative RT after BCS reduces local failure rates
Table 3. Estrogen receptor-positive cohort: adjustedproportional hazards regression results divided at median
RT timing from surgery HR 95% CI p
Local recurrence#77 d 0.84 0.38–1.89 .68$78 d 1.00
Disease-free survival#77 d 0.95 0.71–1.28 .73$78 d 1.00
Overall survival#77 d 1.16 0.77–1.74 .48$78 d 1.00
Abbreviations as in Table 2. Adjustment factors as in Table 2.
substantially and thus has been well accepted (1). However,
the optimal interval between surgery and the start of RT is
controversial. A recent meta-analysis by Chen et al. (9) indi-
cated an increasing relative risk of 1.11/month of RT delay
for local recurrence in so-called high-quality series, irrespec-
tive of whether chemotherapy was given; however, no signif-
icant effect was found on distant metastasis or OS. That meta-
analysis confirmed a previous systematic review (10), in
which the 5-year local relapse rate was significantly greater
in breast cancer patients starting adjuvant RT >8 weeks after
surgery compared with patients treated within 8 weeks (odds
ratio, 1.62; 95% CI, 1.21–2.16). However, these meta-
analyses included patients with a variety of breast cancer
subtypes and for whom the use of systemic therapy was
78–112 d 0.99 0.31–3.17 .99$113 d 1.00
Disease-free survivaly
#48 d 0.72 0.48–1.09 .1249–77 d 0.82 0.55–1.22 .3278–112 d 0.65 0.42–0.99 .04$113 d 1.00
Overall survivalz
#48 d 0.76 0.44–1.32 .3349–77 d 0.80 0.47–1.38 .4278–112 d 0.42 0.23–0.78 .005$113 d 1.00
Abbreviations as in Table 2.* Overall Wald p = .85.y Overall Wald p = .20.z Overall Wald p = .05. Adjustment factors as in Table 2.

Loca
l rec
urre
nce
free
inte
rval
(%)
0
20
40
60
80
100
Time from Start of Radiotherapy (Years)0 1 2 3 4 5 6 7 8 9 10 11 12
≤ 77 days≥ 78 days
N492472
Events2116
10-YearInterval% ± SE
95 ± 196 ± 1
0.55pDays Surgery to RT
A
DFS
(%)
0
20
40
60
80
100
Time from Start of Radiotherapy (Years)0 1 2 3 4 5 6 7 8 9 10 11 12
≤ 77 days≥ 78 days
N492472
Events145126
10-YearDFS% ± SE
72 ± 273 ± 2
0.55pDays Surgery to RT
B
OS
(%)
0
20
40
60
80
100
Time from Start of Radiotherapy (Years)0 1 2 3 4 5 6 7 8 9 10 11 12
≤ 77 days≥ 78 days
N492472
Events8576
10-YearOS% ± SE
83 ± 284 ± 2
0.79pDays Surgery to RT
C
Fig. 1. Kaplan-Meier curves for (A) interval to local recurrence, (B)disease-free survival (DFS), and (C) overall survival (OS) with in-terval to event from start of radiotherapy (RT) for patients with ra-diotherapy within or after 77 days after surgery. SE = standard error.
Loca
l rec
urre
nce
free
inte
rval
(%)
0
20
40
60
80
100
Time from Start of Radiotherapy (Years)0 1 2 3 4 5 6 7 8 9 10 11 12
≤ 48 days49-77 days
N234258
Events1110
10-YearInterval% ± SE
95 ± 295 ± 2
78-112 days≥ 113 days
226246
88
95 ± 296 ± 1
0.91pDays Surgery to RT
A
DFS
(%)
0
20
40
60
80
100
Time from Start of Radiotherapy (Years)0 1 2 3 4 5 6 7 8 9 10 11 12
≤ 48 days49-77 days
N234258
Events6778
10-YearDFS% ± SE
72 ± 372 ± 3
78-112 days≥ 113 days
226246
5571
75 ± 372 ± 3
0.39pDays Surgery to RT
B
OS
(%)
0
20
40
60
80
100
Time from Start of Radiotherapy (Years)0 1 2 3 4 5 6 7 8 9 10 11 12
≤ 48 days49-77 days
N234258
Events3946
10-YearOS% ± SE
83 ± 383 ± 3
78-112 days≥ 113 days
226246
2947
86 ± 381 ± 3
0.22pDays Surgery to RT
C
Fig. 2. Kaplan-Meier curves for (A) interval to local recurrence, (B)disease-free survival (DFS), and (C) overall survival (OS) with in-terval to event from start of radiotherapy (RT) in quartiles (#48,49–77, 78–112, and $113 days). SE = standard error.
Timing of RT for adjuvant breast cancer d P. KARLSSON et al. 401
inconsistent. Both of these factors could have affected the lo-
cal recurrence rate. Only a few studies have evaluated the in-
terval of RT after surgery in the absence of chemotherapy.
The more recent meta-analysis (9) identified only four studies
(3, 5, 15, 16), all of which were observational. However, all
had an adequate description of the distribution of relevant
prognostic factors, which were either well balanced
between the comparison groups or appropriately adjusted
for in the analyses. Of the individual studies, the largest by
far (5) examined the effect of RT delay of <6, 6–8, 9–12,
and $13 weeks on 1,962 patients who had undergone
BCS. Of the 1,962 patients, 677 had received tamoxifen,
and no patients had undergone chemotherapy. Of these pa-
tients, 23 had had a RT delay of >20 weeks. At a median
follow-up of 71 months, the local recurrence rate was signif-
icantly associated with the omission of tamoxifen and a high

402 I. J. Radiation Oncology d Biology d Physics Volume 80, Number 2, 2011
histologic tumor grade. The interval between BCS and RT
was not significantly associated with local recurrence in
a model incorporating tamoxifen use and histologic grade,
in contrast to the overall finding of the meta-analysis, but
consistent with our results.
A more recent publication from the British Columbia Can-
cer Agency examined different intervals between surgery and
RT in early-stage breast cancer patients in the absence of che-
motherapy (8). The study yielded results similar to those of
the present study for an RT delay of #20 weeks. However,
a RT delay of >20 weeks resulted in an inferior outcome. Pa-
tients who were not given endocrine therapy were analyzed
separately, and the findings were similar to those for the en-
tire cohort. However, no separate subgroup analysis was
done for patients who were given endocrine therapy (8). In
a recent study from Florence (4), the risk of developing breast
cancer failure for patients without any systemic adjuvant
treatment (n = 1,935) was inversely proportional to the inter-
val between surgery and RT on univariate analysis. However,
timing of RT was not statistically significance on multivariate
analysis. Similar results were obtained in the RT/endocrine
therapy group (n = 1,684) and RT/endocrine therapy/chemo-
therapy group (n = 529). RT timing was statistically signifi-
cant on multivariate analysis only for the RT and
chemotherapy group (n = 672; HR, 1.69; p = .045) (4).
That report also did not provide separate analyses of patients
undergoing RT and endocrine therapy. In a previous publica-
tion by our group, we analyzed the effect of RT delay result-
ing from chemotherapy in IBCSG Trials VI and VII (11). The
present analysis was undertaken, because studies investigat-
ing RT timing in patients with endocrine therapy have been
rare. Similar to others (4), we could not find any effect of
the interval from surgery to RT on local control or other end-
points. However, the present study had too few events to pro-
vide an accurate estimate of the effect of RT delay of >20
weeks. In addition, a limitation of the present study was an
insufficient power to reject an association between an RT de-
lay of shorter intervals and a small increase in the local recur-
rence risk. Nevertheless, and despite its retrospective design,
the present study included patients treated in a randomized
study with defined inclusion/exclusion criteria, uniform adju-
vant therapy, and rigid follow-up control, in contrast to most
previously published observational series.
The question of the effect of sequential or concurrent use
of endocrine treatment and RT on tumor control could not
be addressed in the present study. In IBCSG Trials VII–IX,
most patients started endocrine therapy within 2 days after
randomization, except for those assigned to receive CMF
first, and RT was administered concurrently with endocrine
therapy.
A study of IBCSG Trials VI and VII showed that a delay of
RT from BCS of #6.6 months (28 weeks), during which che-
motherapy was given, did not adversely influence the treat-
ment outcome (11). The results of the present IBCSG study
have indicated that an interval of up to about 20 weeks be-
tween BCS and RT does not increase the risk of local recur-
rence in a cohort of patients receiving standard adjuvant
endocrine treatment.
REFERENCES
1. Clarke M, Collins R, Darby S, et al. Effects of radiotherapy andof differences in the extent of surgery for early breast cancer onlocal recurrence and 15-year survival: An overview of the rand-omised trials. Lancet 2005;366:2087–2106.
2. Fletcher GH. Implications of the density of clonogenic infesta-tion in radiotherapy. Int J Radiat Oncol Biol Phys 1986;12:1675–1680.
3. Clarke DH, Le MG, Sarrazin D, et al. Analysis of local-regionalrelapses in patients with early breast cancers treated by excisionand radiotherapy: Experience of the Institut Gustave-Roussy.Int J Radiat Oncol Biol Phys 1985;11:137–145.
4. Livi L, Borghesi S, Saieva C, et al. Radiotherapy timing in4,820 patients with breast cancer: University of Florence expe-rience. Int J Radiat Oncol Biol Phys 2009;73:365–369.
5. Froud PJ, Mates D, Jackson JS, et al. Effect of time interval be-tween breast-conserving surgery and radiation therapy on ipsi-lateral breast recurrence. Int J Radiat Oncol Biol Phys 2000;46:363–372.
6. Benk V, Joseph L, Fortin P, et al. Effect of delay in initiatingradiotherapy for patients with early stage breast cancer. Clin On-col (R Coll Radiol) 2004;16:6–11.
7. Hebert-Croteau N, Freeman CR, Latreille J, et al. Delay in ad-juvant radiation treatment and outcomes of breast cancer—A re-view. Breast Cancer Res Treat 2002;74:77–94.
8. Olivotto IA, Lesperance ML, Truong PT, et al. Intervals longerthan 20 weeks from breast-conserving surgery to radiation ther-apy are associated with inferior outcome for women with early-stage breast cancer who are not receiving chemotherapy. J ClinOncol 2009;27:16–23.
9. Chen Z, King W, Pearcey R, et al. The relationship betweenwaiting time for radiotherapy and clinical outcomes: A system-atic review of the literature. Radiother Oncol 2008;87:3–16.
10. Huang J, Barbera L, Brouwers M, et al. Does delay in startingtreatment affect the outcomes of radiotherapy? A systematic re-view. J Clin Oncol 2003;21:555–563.
11. Wallgren A, Bernier J, Gelber RD, et al. Timing of radiotherapyand chemotherapy following breast-conserving surgery for pa-tients with node-positive breast cancer. Int J Radiat OncolBiol Phys 1996;35:649–659.
12. International Breast Cancer Study Group. Effectiveness of adju-vant chemotherapy in combination with tamoxifen for node-positive postmenopausal breast cancer patients. J Clin Oncol1997;15:1385–1394.
13. International Breast Cancer Study Group. Adjuvant chemother-apy followed by goserelin versus either modality alone for pre-menopausal lymph node-negative breast cancer: a randomizedtrial. J Natl Cancer Inst 2003;95:1833–1846.
14. International Breast Cancer Study Group. Endocrine respon-siveness and tailoring adjuvant therapy for postmenopausallymph node-negative breast cancer: A randomized trial. J NatlCancer Inst 2002;94:1054–1065.
15. Whelan TJ, Clark RM, Levine MN, et al. The effect of delay ininitiating radiotherapy postlumpectomy on local breast recur-rence. Int J Radiat Oncol Biol Phys 1996;36:280.
16. Vujovic O, Perera F, Dar AR, et al. Does delay in breast irradi-ation following conservative breast surgery in node-negativebreast cancer patients have an impact on risk of recurrence?Int J Radiat Oncol Biol Phys 1998;40:869–874.
Top Related