






Languages
Pages
Legal


Thomas Repas DO FACP FACOI FNLA FACE CDE
OSTEOPOROSIS 2012Update and Review of Current Controversies
Board Certified:• Endocrinology, Diabetes and
Metabolism• Clinical Lipidology• Nutrition• Internal Medicine
Regional Medical ClinicAspen Centre- Endocrinology640 Flormann StreetRapid City, South Dakota
Clinical Assistant Professor, Dept. of Internal Medicine, University of South Dakota, Sanford School of Medicine

Objectives Brief review of pathophysiology, diagnosis and
prevalence of osteoporosis Understand the concept of fracture risk and how
it should be applied to therapeutic decision-making
Identify current treatment options: Non-pharmacologic Medications
Discuss controversies in osteoporosis Adverse events: ONJ, Atypical femur fractures Bisphosphonate Holidays? Use of bone turnover markers? How often should follow-up DXAs be performed?

OSTEOPOROSISPathophysiology and
prevalence

Osteoporosis: Definition
“Osteoporosis is defined as a skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture.”
NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis,
and Therapy.. JAMA. 2001;285:785-795.

Fracture Risk Depends on Bone Strength
Increased
bone
turnover
Reduced bone strength/
Increasedfracturerisk
Decreased bone mass
Decreased mineralizati
on
Increased cortical porosity
Disrupted trabecular
connectivity
Lips P. Endocr Rev. 2001;22(4):477–501.

Clinical Presentation of Osteoporosis
Bone Health and Osteoporosis: A Report of the Surgeon General. Rockville, Md: US Department of Health and Human Services; 2004:187-217.
• Usually asymptomatic until fracture occurs
• Clinical signs and symptoms:• Low-trauma fragility
fractures of spine, wrist or hip
• Loss of height• Kyphosis• Acute or chronic pain
• Diagnostic studies• Bone mineral density
assessment• X-rays or morphometry

Bone Remodeling Cycle in Normal Bone
Lining cells
Resting
Bone
ResorptionOsteoclasts digest bone within a sealed resorption vacuole
Bone
Reversal
Apoptotic osteoclasts
Preosteoblasts
Bone
Mature osteoblasts building osteoid tissue
MineralizationFormation
Bone
Illustration Copyright ©2009 Nucleus Medical Art, All rights reserved. www.nucleusinc.com

Why Bone Remodeling?Allows skeleton toRespond to mechanical loadingRepair and prevent microdamage
(“wear & tear”) Maintains quality control
Release growth factors and minerals (calcium and phosphate) stored in matrix into circulation
All bone cells participate in remodeling Considerable energy expended to remodel the skeleton

Osteoporosis: Factors that increase risk of fractureGenetic or non-modifiable• Age• Female sex• Asian or white
ethnic origin• Previous fragility
fracture• Family history of
hip fracture• Small frame
National Osteoporosis Foundation. Fast facts on osteoporosis. Available at: http://www.nof.org/osteoporosis/diseasefacts.htm. Accessed August 13, 2007.
Potentially modifiable• Estrogen deficiency and
menopause• Low body weight• Calcium and vitamin D
deficiency• Inadequate physical
activity• Excessive alcohol intake• Cigarette smoking• Long-term glucocorticoid
use

Annual Incidence of Osteoporotic Fractures in US
National Osteoporosis Foundation. Fast facts on osteoporosis. Available at: http://www.nof.org/osteoporosis/diseasefacts.htm.
Accessed February 7, 2007.
• Osteoporosis is a major public health threat with serious clinical consequences
• 1.5 million fractures annually in the United States
• One hip fracture increases the risk of a second hip fracture fourfold.

Consequences of Fractures
1. National Osteoporosis Foundation. Fast Facts on Osteoporosis. Available at: http://www.nof.org/osteoporosis/diseasefacts.htm. Accessed August 13, 2007.
2. Delmas PD, van de Langerijt L, Watts NB, J Bone Miner Res. 2005;20:557-563.3. Burge R, Dawson-Hughes B, et al .. J Bone Miner Res. 2007;22:465-475.
• Vertebral fractures• Severe back pain• Kyphosis and height loss
• Hip fracture• Loss of ambulatory status
(30%)• Admission to chronic care
facility• Death
• All fractures are associated with increased risk for future fractures
• Burden on society in terms of public health, health care resources, direct and indirect costs

1-Year Risk of Refracture in Patients With Incident Vertebral Fracture
Lindsay R, Burge RT, Strauss DM. One year outcomes and costs following a vertebral fracture. Osteoporos Int. 2005;16:78-85.

Osteoporosis: Prevalence
10 million in the US have established osteoporosis.
34 million additional people have low bone mass (osteopenia)
National Osteoporosis Foundation. Fast facts on osteoporosis. Available at: http://www.nof.org/osteoporosis/diseasefacts.htm. Accessed February 7, 2007.

Osteoporosis: Prevalence
By 2020, 61 million may have osteoporosis or low bone mass 14 million with established
osteoporosis. 47 million with low bone mass.
National Osteoporosis Foundation. Fast facts on osteoporosis. Available at: http://www.nof.org/osteoporosis/diseasefacts.htm.
Accessed February 7, 2007.

Osteoporosis is underdiagnosed
Morris CA, Carrino JA, Lang P, et al. Incidental vertebral fractures on chest radiographs. Recognition, documentation, and treatment. J Gen Intern Med. 2006;21:352-356.
Among 10,291 hospitalized women with chest radiographs, 142 (1.4%) had vertebral fractures.
• 41% had fracture noted in the x-ray report.
• 16% had fracture noted on discharge summary.
• 13% were given an initial prescription for osteoporosis therapy at discharge

OSTEOPOROSISDiagnosis, fracture risk
assessment and therapeutic decision-
making

ISCD: Indications for Bone Mineral Density (BMD) Testing
2007 ISCD Official Positions http://www.iscd.org/visitors/pdfs/ISCD2007OfficialPositions-Combined-AdultandPediatric.pdf
• Women aged 65 and older • Postmenopausal women under age 65
with risk factors for fracture. • Women during the menopausal
transition with clinical risk factors for fracture, such as low body weight, prior fracture, or high-risk medication use.
• Men aged 70 and older. • Men under age 70 with risk factors for
fracture.

ISCD: Indications for BMD Testing -continued-
2007 ISCD Official Positions http://www.iscd.org/visitors/pdfs/ISCD2007OfficialPositions-Combined-AdultandPediatric.pdf
.
• Adults with a fragility fracture. • Adults with a disease or condition
associated with low bone mass or bone loss.
• Adults taking medications associated with low bone mass or bone loss.
• Anyone being considered for pharmacologic therapy.
• Anyone being treated, to monitor treatment effect.
• Anyone not receiving therapy in whom evidence of bone loss would lead to treatment

Bone Density Criteria for Diagnosing Osteoporosis
Prevention and Management of Osteoporosis. Report of a WHO Scientific Group. WHO Technical Report Series 921. Geneva: World Health Organization, 2003.
•T-score = units of standard deviation (SD) that a patient’s BMD is above or below mean peak bone mass for a young adult, measured at the spine or hip.
• Reduction in T-score by 1 SD is equivalent to a 10% to 12% decrease in BMD.
• Generally, a change in T-score by 1 SD increases a person’s fracture risk by 1.5 to 2.5-fold.

Bone Density Criteria for Diagnosing Osteoporosis
Prevention and Management of Osteoporosis. Report of a WHO Scientific Group. WHO Technical Report Series 921. Geneva: World Health Organization, 2003.
• Normal BMD: T-score of -1 or above.
• Low bone mass (osteopenia) : T-score between 1 and 2.5.
• Osteoporosis: T-score lower than 2.5.
• Severe, or established, osteoporosis: T-score lower than 2.5 with fragility fractures.

Fragility Fracture and Osteoporosis
Prevention and Management of Osteoporosis. Report of a WHO Scientific Group. WHO Technical Report Series 921. Geneva: World Health Organization, 2003.
• The presence of a fragility fracture is diagnostic for osteoporosis regardless of the T-score.
• Definition: A fracture that occurs spontaneously or with minimal trauma, such as due to a fall of one’s standing height or less.

BMD Reporting in Females Prior to Menopause and in Males < 50 yrs
2007 ISCD Official Positions http://www.iscd.org/visitors/pdfs/ISCD2007OfficialPositions-Combined-AdultandPediatric.pdf
• Z-scores, not T-scores, are preferred. This is particularly important in children.
• Z-score of -2.0 or lower is defined as “below the expected range for age”
• Z-score above -2.0 is “within the expected range for age.”
• Osteoporosis cannot be diagnosed in men under age 50 on the basis of BMD alone.

WHO Fracture Risk Assessment Tool
WHO Fracture Risk Assessment Tool http://www.shef.ac.uk/FRAX/

Risk Factors used in the WHO FRAX® tool
WHO Fracture Risk Assessment Tool http://www.shef.ac.uk/FRAX/
• Enter Age, gender, height (cm), weight (kg).
• Previous fracture? a fracture in adult life occurring spontaneously, or arising from trauma which, in a healthy individual, would not have resulted in a fracture.
• Parent fractured hip? history of hip fracture in the patient's mother or father.
• Current smoking?

Risk Factors used in the WHO FRAX® tool
WHO Fracture Risk Assessment Tool http://www.shef.ac.uk/FRAX/
• Glucocorticoids? is patient currently exposed to oral glucocorticoids or has been exposed to oral glucocorticoids for more than 3 months at a dose of prednisolone of 5mg daily or more (or equivalent doses of other glucocorticoids)?

Risk Factors used in the WHO FRAX® tool
WHO Fracture Risk Assessment Tool http://www.shef.ac.uk/FRAX/
• Rheumatoid arthritis?
• Secondary osteoporosis? Does the patient have a disorder strongly associated with osteoporosis. This includes type I (insulin dependent) diabetes, osteogenesis imperfecta in adults, untreated long-standing hyperthyroidism, hypogonadism or premature menopause (<45 years), chronic malnutrition, or malabsorption and chronic liver disease
Alcohol 3 or more units/day
Enter yes if the patient takes 3 or more units of alcohol daily. A unit of alcohol varies slightly in different countries from 8-10g of alcohol. This is equivalent to a standard glass of beer (285ml), a single measure of spirits (30ml), a medium-sized glass of wine (120ml), or 1 measure of an aperitif (60ml) (see also notes on risk factors).
Bone mineral density (BMD)
(BMD) Please select the make of DXA scanning equipment used and then enter the actual femoral neck BMD (in g/cm2). Alternatively, enter the T-score based on the NHANES III female reference data. In patients without a BMD test, the field should be left blank (see also notes on risk factors) (provided by Oregon Osteoporosis Center).

Risk Factors used in the WHO FRAX® tool
WHO Fracture Risk Assessment Tool http://www.shef.ac.uk/FRAX/
• Alcohol 3 or more units/day? A unit of alcohol is equivalent to a standard glass of beer (285ml), a single measure of spirits (30ml), a medium-sized glass of wine (120ml), or 1 measure of an aperitif (60ml)
• Bone mineral density (BMD): select the make of DXA scanning equipment used and then enter the actual femoral neck BMD (in g/cm2) or the T-score

WHO Fracture Risk Assessment Tool
WHO Fracture Risk Assessment Tool http://www.shef.ac.uk/FRAX/

NOF Criteria for Initiating Medical Therapy for Low Bone Mass and Osteoporosis
NOF Clinician's Guide to Prevention and Treatment of Osteoporosis: http://www.nof.org/professionals/clinical-guidelines
1. A hip or vertebral (clinical or morphometric) fracture
2. T-score ≤ -2.5 at the femoral neck or spine after evaluation excluding secondary causes
3. Low bone mass (T-score -1.0 to-2.5 at the femoral neck or spine) AND a 10-year probability of a hip fracture ≥ 3% OR a 10-year probability of a major osteoporosis-related fracture ≥ 20%
• Clinicians judgment and/or patient preferences also must also be taken into consideration

OSTEOPOROSISCurrent therapeutic options

US Department of Health and Human Services. Bone Health and Osteoporosis: A Report of the Surgeon General. US Dept of Health and
Human Services, Office of the Surgeon General; 2004.
Pharmacotherapy
(antiresorptives and anabolics)
Address Secondary Factors
(drugs and diseases)
Lifestyle Changes(nutrition, physical activity, and fall prevention)
Osteoporosis Prevention and Treatment
Preventing and Treating Osteoporosis

Measures to Prevent Bone Loss Maintain adequate calcium intake; use
calcium supplements, if needed, to meet minimal required intake
Maintain adequate vitamin D intake; supplement vitamin D, if needed, to maintain serum levels of 25-OH vit D between 30 and 60 ng/mL
Limit alcohol intake to no more than 2 servings/day
Limit caffeine intake Avoid or stop smoking Maintain an active lifestyle, including
weight bearing exercises for at least 30 minutes daily
American Association of Clinical Endocrinologists Guidelines for Clinical Practice for the Diagnosis and Treatment of Postmenopausal Osteoporosis © 2010.

Non-Pharmacologic Treatment of OsteoporosisAll the previous measures plus the following: Maintain adequate protein intake Use proper body mechanics Consider the use of hip protectors in
individuals with a high risk of falling Take measures to reduce the risk of
falling Consider referral for physical therapy
and occupational therapyAmerican Association of Clinical Endocrinologists Guidelines for Clinical Practice for the Diagnosis and Treatment of Postmenopausal Osteoporosis © 2010.

Measures to Prevent Falls Anchor rugs, use nonskid mats,
remove loose wires and minimize clutter
Install handrails in bathrooms, halls, and long stairways
Light hallways, stairwells, and entrances
Encourage patient to wear sturdy, low-heeled shoes
Recommend hip protectors for patients who are predisposed to falling
American Association of Clinical Endocrinologists Guidelines for Clinical Practice for the Diagnosis and Treatment of Postmenopausal Osteoporosis © 2010.

Before Starting Medication Consider…
Basic laboratory work up: Complete blood count Serum chemistry, including calcium,
phosphorus, total protein, albumin, liver enzymes, alkaline phosphatase, creatinine, and electrolytes
Serum 25-hydroxyvitamin D
American Association of Clinical Endocrinologists Guidelines for Clinical Practice for the Diagnosis and Treatment of Postmenopausal Osteoporosis © 2010.

If reasons to suspect secondary causes of bone loss: TSH Erythrocyte sedimentation rate PTH for possible primary or secondary
hyperparathyroidism 24-hour urine calcium Tissue transglutaminase antibodies for suspected
celiac disease Urinary free cortisol or other tests for suspected
Cushings Serum tryptase or other tests for mastocytosis Serum protein electrophoresis and free kappa and
lambda light chains for suspected myeloma In men, testosterone Other? Bone marrow biopsy? Iliac crest bone
biopsy?
American Association of Clinical Endocrinologists Guidelines for Clinical Practice for the Diagnosis and Treatment of Postmenopausal Osteoporosis © 2010.

Ultimate Goal of Osteoporosis PharmacotherapyTo minimize fracture risk by achieving
“normal” bone strength
Ideally therapy should be safe, well-tolerated, easy to administer, and inexpensive
Slide by Dr. David Dempster

Medications for treating low bone mass and osteoporosis
Antiresorptives Bisphosphonates Anti-RANK ligand
antibody (denosumab)
Calcitonin SERMs (selective
estrogen receptor modulators)
Anabolic Therapy Teriparatide
Estrogen and HRT For prevention
onlyNational Osteoporosis Foundation.. Available at:
http://www.nof.org/patientinfo/medications.htm. Accessed February 7, 2007.
Rogers MJ, Frith JC, Luckman P, et al. Bone. 1999;24(suppl):73S-79S.
Papapoulos S, Frölich M. J Clin Endocrinol Metab. 1996;81:2990-3997.

Antiresorptive TherapyMechanism of Fracture Risk Reduction Antiresorptive
therapy
Stabilize or improve
microarchitecture
REDUCE bone turnover
Decrease in fracture risk
Increase BMD
From presentation given by Dr. Paul Miller.

Estrogen: Women’s Health Initiative Fracture Data
5.2 years average follow-up
Writing Group for the Women’s Health Initiative. JAMA. 2002; 288 (3): 321-333 .

Estrogen: Women’s Health Initiative Over one year, 10,000 women taking
estrogen plus progestin compare to placebo experienced: 7 more CHD events 8 more strokes 18 more thromboembolic events 8 more invasive breast cancers 6 fewer colorectal cancers 5 fewer hip fractures
Writing Group for the Women’s Health Initiative. JAMA. 2002; 288 (3): 321-333 .

Estrogen: FDA Recommendations
When prescribing medications to prevent osteoporosis, clinicians should consider all non-estrogen preparations first.
When prescribing estrogen, clinicians should prescribe lowest dose for shortest time possible.
Clinicians should prescribe estrogen containing products only when benefits outweigh the risks for a specific patient.
US Food and Drug Administration. FDA News. January 8,2003

Selective estrogen receptor modulators (SERMs) Raloxifene: a selective estrogen receptor
modulator: Acts as estrogen agonist on bone Acts as estrogen antagonist on breast and
uterus
↓ Bone turnover
↑ BMD but to lesser degree than bisphosphonates
↓ Vertebral fractures
Does not reduce hip or other non-vertebral fractures
Ettinger B, et al. JAMA. 1999;282:637-645.

Effect of Raloxifene in Women with or Without Pre-Existing FracturesMORE Trial—3 Years
aWomen who completed the study and had evaluable radiographs at 36 months.
Ettinger B, et al. JAMA. 1999;282:637-645.
% o
f W
om
en
wit
hIn
cid
en
t Vert
eb
ral Fr
act
ure
s
Raloxifene 60 mg/dPlacebo
Without Pre-ExistingVertebral Fracture
RR 0.5a
(95% CI = 0.3–0.7)
With Pre-ExistingVertebral Fracture
RR 0.7a
(95% CI = 0.6–0.9)
30%
55%
0
5
10
15
20
25

Raloxifene and Breast Cancer
4 years with raloxifene 72% relative risk reduction in incidence of new breast cancer compared to placebo
8-year extension trial data showed 66% relative risk reduction in incidence of new onset breast cancer in raloxifene treated patients compared to placebo
Vogel VG, et al. JAMA. 2006;295:2727-2741.

Raloxifene: Side effects and adverse events
Hot flashes Deep vein thrombosis Leg cramps Small increase in risk of fatal stroke
Barret-Connor E, et al. N Enlg J Med. 2006 Jul 13; 355 (2): 125-137

Calcitonin
Derived from parafollicular cells of the thyroid gland
Inhibits bone resorption
Available in nasal and subcutaneous formulations
Excellent safety profile
Ability to reduce pain with injectable formulations
Indicated for women at least 5 years postmenopausal who are unable to tolerate other osteoporosis medications.

Calcitonin: Effects on Fracture
• Nasal formulation’s reduction in vertebral fracture occurred only in the 200 IU/spray formulation
• Lower and higher doses had no effect
• No dose has shown nonvertebral fracture risk reductionChesnut CH 3rd, et al. Am J Med. 2000; Sep; 109 (4): 267-76.
N=1255 postmenopausal women with osteoporosis.

Bisphosphonates
Analogs of naturally occurring pyrophosphates
High affinity for bone at the calcium-phosphorus interface surface and stabilizes the crystal
Reduce osteoclast activity by inhibiting the enzyme farnesyl pyrophosphate synthetase (FPPS)
Differences among bisphosphonates are related to differences in the physiochemical and cellular effects
Bisphosphonates are not metabolized. The molecule released from bone retains biologic activity

Bisphosphonates: Effects
↓ Bone turnover
↑ BMD at lumbar spine and hip
↓ Vertebral and non-vertebral fractures
Sustained effects with continued treatment
Best studied class of medications used to treat osteoporosis.
Long term record of safety and adverse events1. Black DM et al. Lancet. 1996; 1535-1541.
2. Body J-J, et al. J Clin Endocrinol Metab. 2002; 87: 4528-45353. Chestnut CH III et al J Bone Miner Res. 2004; 19: 1241 – 12494. Harris ST et al. JAMA 1999; 282: 1344-1352..

Available Bisphosphonates for Osteoporosis
Oral Alendronate (daily, weekly) Risedronate (daily, weekly, monthly) Ibandronate (daily, monthly)
Intravenous Ibandronate (quarterly) Zoledronic acid (annual)
Off-label Pamidronate (IV quarterly)

Effects of Bisphosphonates on Osteoclast Function
1. Rogers MJ, Frith JC, Luckman SP, et al.. Bone. 1999;24(suppl 5):73S-79S.2. Fleisch H.. Endocr Rev. 1998;19:80-100. 3. Sato M, Grasser W, Endo N, et al.. J Clin Invest. 1991;88:2095-2105. 4. Rogers MJ Curr Pharm Des. 2003;9(32):2643-58. 5. Hughes DE, Wright KR, Uy HL, et al. J Bone Miner Res. 1995;10:1478-1487.
Normal Osteoclast Osteoclast after uptake of bisphosphonate

Administration guidelines for oral bisphosphonates
Must take medication first thing in AM after arising before eating or drinking with 8 oz of water.
Must be NPO for at least ½ hour Ibandronate must be taken at least 1 hour
before eating or drinking Patients must remain upright by walking,
standing or sitting for ½ hour. Remind patients that this includes not lying
down of going back to bed. Exception: AtelviaTM

Poor Compliance and Persistence Lead to Compromised Fracture Risk Reduction
Siris ES, Harris ST, Rosen CJ, et al. Mayo Clin Proc. 2006;81:1013-1022.

Refill Compliance and Fracture Protection Over 24 Months for Bisphosphonate-Treated Patients
Siris ES, Harris ST, Rosen CJ, et al. Mayo Clin Proc. 2006;81:1013-1022.

Advantages of IV Bisphosphonates Oral bisphosphonates have fastidious
absorption patterns (exception: AtelviaTM )
Oral bisphosphonates may induce GI intolerability
Oral bisphosphonate may be contraindicated in patients with GI diseases (achalasia, scleroderma, Barrett’s, etc)
Serum levels of bisphosphonate cannot be measured, creating uncertainties around oral absorption and bone bioavailability in certain clinical scenarios

Bisphosphonates: Side effects, contraindications and other concerns Side effects:
Upper GI (oral) Musculoskeletal pain First phase reactions (IV)
Contraindicated in renal insufficiency Other concerns (these will be discussed
more later): Osteonecrosis of the jaw? Atypical femur fractures?

Denosumab Human monoclonal antibody-IgG2 isotype
High affinity and specificity for human RANK ligand
Does not bind to TNFα, TNFβ, TRAIL, or CD40L
Pharmacokinetics (SC): similar to other fully human IgG2 monoclonal antibodies
Absorption is rapid and prolonged (Cmax ≈1–4 wks postdose)
Long half-life ≈34 days with maximum dose Distribution ≈ intravascular volume Clearance ≈ reticuloendothelial system No kidney filtration or excretion of intact
molecule Bekker PJ, et al. J Bone Miner Res. 2004;19:1059-1066.
Boyle WJ, et al. Nature. 2003;423:337-342.
Abbreviations: TNF, tumor necrosis factor; TRAIL, TNF-related apoptosis-inducing ligand.

Denosumab: Mechanism of Action
Growth Factors HormonesCytokines
Bone
Abbreviation: CFU-M, colony forming unit macrophage.
Osteoblast Lineage
Osteoclast
CFU-M
Pre-Fusion Osteoclast
MultinucleatedOsteoclast
RANK
RANKL
OPGDmab

Denosumab: Serum Levels (1 mg/kg SC)
Bekker PJ, et al. J Bone Miner Res. 2004;19:1059-1066.
1 3 5 9
Study Month
0 2 4 60
101
102
103
104
Ser
um
Lev
el (
ng
/mL
)
EC50

Denosumab: Effects 68% decrease in vertebral fractures
2.3% vs 7.2%, P <.0001
41% decrease in hip fractures 0.7% vs 1.2%, P = .036
20% decrease in nonvertebral fractures 6.5% vs 8.0%, P = .011
Denosumab increases BMD and reduces bone turnover markers compared with placebo
AEs and SAEs generally similar to placebo No increased risk of cancer, infection,
cardiovascular disease, delayed fracture healing, hypocalcemia, no osteonecrosis of the jaw
Increased risk of cellulitis, eczema, flatulence; decreased risk of falls, concussionCummings SR, et al. N Engl J Med. 2009;361:1-10.

Denosumab: Discontinuation
Serum CTx Lumbar Spine BMD
Miller PD et al. . Bone. 2008; 43: 222-229

Denosumab: Retreatment
Serum CTx Lumbar Spine BMD
Miller PD et al. . Bone. 2008; 43: 222-229

Anabolic TherapyMechanism of Fracture Risk Reduction
Anabolic therapy
Stabilize or improve
microarchitecture
INCREASE bone turnover
From presentation given by Dr. Paul Miller.
Increase in BMD
Decrease Fracture Risk

Teriparatide
First in class of anabolic (bone-building) agents
Human PTH has 84 amino acids, teriparatide is the active 1-34 amino acid portion
Approved by the FDA in 2002.
Approximately doubles rate of bone formation in patients with osteoporosis1. Neer RM, et al. N Eng J Med. 2001; 344: 1434-1441.
2. Forteo (teriparatide [rDNA origin] injection) prescribing information. Eli Llly and Co; September 2004.

Teriparatide
Stimulates osteoblast activity and overall bone remodeling, resulting in new bone formation.
↑ bone mass
↓ vertebral and non-vertebral fractures
Improves trabecular microarchitecture and increases cortical thickness
Requires daily SC injections.
1. Neer RM, et al. N Eng J Med. 2001; 344: 1434-1441.2. Forteo (teriparatide [rDNA origin] injection) prescribing information. Eli Llly and Co; September 2004.

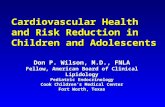
Effect of Teriparatide on Risk of Vertebral Fractures in Postmenopausal Women
0
2
4
6
8
10
12
14
16
Placebo Teriparatide 20 µg
% o
f Pa
tients
wit
h ≥
1 F
ract
ure
RR 0.35 (95% CI = 0.22–0.55)a
65%
aP <.001 vs placebo.
Neer RM, et al. N Engl J Med. 2001;344:1434-1441.Adapted from graphic by Dr. Paul Miller.

Nonvertebral and Hip Fractures Teriparatide
5 fragility hip fractures (control + primary treatment group).Nonvertebral fractures = fragility fractures, otherwise not specified.
0
5
10
15
20
Nonvertebral Fractures Hip Fractures
Control
Teriparatide 20 µg
RR = 0.5 (0.3,0.9)
NSPer
cen
t w
ith
New
Fra
ctu
res
Neer R, et al. N Engl J Med. 2001;344:1434–1441.Adapted from graphic by Dr. Paul Miller.

Teriparatide
Subcutaneous injections every day
Treatment duration = 2 years
Patient must be initiated on antiresorptive therapy after course of teriparatide completed or will rapidly lose any gains in BMD
Cannot be used in patients with contraindications
1. Neer RM, et al. N Eng J Med. 2001; 344: 1434-1441.2. Forteo (teriparatide [rDNA origin] injection) prescribing information. Eli Llly and Co; September 2004.

Contraindications to Teriparatide
Unexplained hypercalcemia Unexplained elevated alkaline
phosphatase Paget’s disease Prior skeletal (therapeutic) radiation Metastatic cancer Unfused epiphysis GFR <30 mL/min

Teriparatide: Side Effects and Adverse Events Side effects:
Leg cramps Dizziness
Use currently limited to 2 years Long term effects unknown Initial PTH trials were stopped early due to
finding of osteosarcoma in animals No excess osteosarcoma reported in
humans FDA assigned boxed warning because of
osteosarcoma in animal studiesUS Food and Drug Administration. FDA Talk Paper. November 2002

AACE Postmenopausal Osteoporosis Guidelines 2010: Choosing a drug First line agents: alendronate,
risedronate, zoledronic acid, and denosumab
Use ibandronate as a second-line agent
Use raloxifene as a second- or third-line agent
Use calcitonin as the last line of therapy
Use teriparatide for patients with very high fracture risk or patients in whom bisphosphonate therapy has failed
Do not use combination therapy
•American Association of Clinical Endocrinologists Guidelines for Clinical Practice for the Diagnosis and Treatment of Postmenopausal Osteoporosis © 2010

Follow-up of Patients on Medication for the Treatment of OsteoporosisMinimal follow-up Verify that patient is taking the medication Verify appropriate dosing procedure for oral
bisphosphonates Verify that patient is taking sufficient calcium
and vitamin D
Other Bone density – not usually before 2 years Bone turnover markers – role uncertain- may be
useful for confirming compliance with therapy and/or effect of therapy
Creatinine, Other labs? 25-OH vitamin D level?

OSTEOPOROSISCurrent controversies

Current controversies in osteoporosis Safety and adverse events
Osteonecrosis of the jaw Atypical or mid-shaft femoral
fractures Bisphosphonate holidays? Assessment of bone turnover
markers? How often should follow-up DXAs
be performed?

Osteonecrosis of the jaw:Background Reports of ONJ have primarily been in
patients with advanced malignancies and skeletal metastases (>90% of cases)
Etiology and pathogenesis are not well characterized
Role of bisphosphonates uncertain
The clinical diagnosis of ONJ is usually made on the basis of visual inspection (eg, presence of exposed bone) and/or radiographic appearance1
No uniform diagnostic criteria currently applied
Ruggiero S, et al. J Oncol Practice. 2006;2:7-14.

Osteonecrosis of the jaw:Signs and symptoms Symptoms
- “Heavy jaw”, a dull aching sensation- Numbness/tingling of the jaw- Tooth pain- Undiagnosed oral pain
Signs- Rough area on the jawbone- soft tissue swelling, drainage or infection- exposed bone in the oral cavity- sudden change in the health of periodontal tissue- Failure of oral mucosa to heal- Loosening of teeth
Ruggiero S, et al. J Oncol Practice. 2006;2:7-14.

Osteonecrosis of the jaw:Clinical Presentation
Exposed bone in maxillofacial area that occurs in association with dental surgery or occurs spontaneously, with no evidence of healing
No evidence of healing after 6 to 8 weeks of appropriate evaluation and dental care
No evidence of metastatic disease in the jaw or osteoradionecrosis
Ruggiero S, et al. J Oncol Practice. 2006;2:7-14.

Osteonecrosis of the jaw:Prevalence 190 million prescriptions in the United
States for oral alendronate, risedronate, and ibandronate
Over 6 million patients treated with iv bisphosphonates for cancer worldwide
ONJ in oral bisphosphonate users ranges from 1:10,000 (from Australia and Israel) to 1:250,000 (from Germany) to 1:160,000 worldwide.
These figures are rough approximations because of difficulties in case finding (not all cases of ONJ are reported and not all cases reported are really ONJ)
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.

Osteonecrosis of the jaw:Bisphosphonates Several different sources of
retrospective data on ONJ incidence are available
ONJ incidence varies widely in retrospective studies
Risk factors vary for different disease states
ONJ was not identified prospectively in any of the clinical trials that included more than 60,000 patient-years in studies of osteoporosis or Paget’s disease
Black DM, et al. N Engl J Med. 2007;356:1809-1822. 2. Grbic J, et al. J Am Dent Assoc.2008;139 (1):32-40. Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565..

Osteonecrosis of the jaw:Bisphosphonates Only 1 study was prospectively
designed to look at adjudicated incidence of ONJ1,2
HORIZON-PFT examined efficacy of zoledronic acid in 7736 patients with postmenopausal osteoporosis:
Only two cases of ONJ identified: 1 case in the active treatment group, 1 case in the placebo group
Both cases healed with conservative treatment of debridement and antibiotics
No difference in rate of ONJ was observed in treatment vs placebo group over 6 years
Black DM, et al. N Engl J Med. 2007;356:1809-1822. 2. Grbic J, et al. J Am Dent Assoc.2008;139 (1):32-40.

Osteonecrosis of the jaw:Prevention Patients who are starting or taking
bisphosphonates should be informed that there are risks of treatment, including a low risk of ONJ.
Regular dental visits and maintenance of good oral hygiene are important for everyone.
Routine dental cleaning and restorative procedures should be strongly encouraged.
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565American Association of Oral and Maxillofacial Surgeons 2007 Position paper on bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg 65:369–376

Osteonecrosis of the jaw:Prevention Patients on bisphosphonates who are
considering surgery should be advised of the risks and alternatives.
Invasive surgical procedures should be avoided, if possible, especially in patients receiving iv bisphosphonates for cancer.
If dental treatment is needed, it should progress stepwise, if possible.
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565American Association of Oral and Maxillofacial Surgeons 2007 Position paper on bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg 65:369–376

Osteonecrosis of the jaw:Prevention Patients with periodontal disease
should receive appropriate non-surgical therapy first.
Patients starting oral bisphosphonates who need invasive dental procedures should have procedures done and healing complete before starting, if circumstances permit.
Patients already taking a bisphosphonate may elect to take some time off therapy, however there is no evidence that this will prevent ONJ.
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565American Association of Oral and Maxillofacial Surgeons 2007 Position paper on bisphosphonate-related osteonecrosis of the jaws. J Oral Maxillofac Surg 65:369–376

Atypical femur fracturesBackground
Case reports of unusual low-energy sub-trochanteric femoral fractures and pelvic insufficiency fractures, which exhibited problems with healing, in patients on long term bisphosphonate therapyWatts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.

Atypical femur fracturesClinical features
Fractures are typically associated with prodromal pain in the region of the fracture
Frequently bilateral Characteristic
radiographic findings include cortical hypertrophy, a transverse fracture pattern, and medial cortical spiking
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.

Atypical femur fractures
Bone biopsies in such patients often (but not always) show severely suppressed bone turnover
Thought to be due to long term over-suppression of bone turnover leading to impaired bone remodeling, accumulation of micro-damage in bone and increased skeletal fragility
Several retrospective studies suggest an association between bisphosphonate use and atypical fractures
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.

Atypical femur fractures
However the observed association between long-term bisphosphonate use and atypical fractures does not prove causality
A register-based national cohort study from Denmark showed that the ratio of classical to atypical hip fractures was identical in the alendronate treated subjects vs. matched untreated controls
Atypical fractures may be due to osteoporosis rather than the bisphosphonate therapy itselfWatts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.
Abrahamsen B, Eiken P, Eastell R 2009 Subtrochanteric and diaphyseal femur fractures in patients treated with alendronate: a registerbased national cohort study. J Bone Miner Res 24:1095–1102

Atypical femur fractures
“Concern about oversuppression of bone turnover resulting in atypical fractures should not lead to stopping bisphosphonate therapy in the vast majority of postmenopausal women at the present time”
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.

Bisphosphonate “Drug Holiday”
Not a topic of discussion when bisphosphonates first launched
Became a consideration after July 9, 2002(WHI JAMA publication)
Became more widely discussed after FLEX (Black et al, JAMA 2004) and better science defining bisphosphonate PK/PD became available
FRAXTM also drove the “drug holiday” discussion in women (untreated) who had been at low risk before bisphosphonates were started
Not yet standard of care in the United StatesMiller PD. Best Prac Res Clin Endocrinol Metab. 2008;22:849–868.

Bisphosphonate “Drug Holiday”
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.

Bisphosphonate “Drug Holiday”
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.
“Duration based largely on personal opinion”

Bisphosphonate “Drug Holiday”
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.
Low risk of fracture: treatment is not needed.
If bisphosphonate has been prescribed, it should be discontinued and not restarted unless/until the patient meets treatment guidelines.

Bisphosphonate “Drug Holiday”
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.
Example- Low risk of fracture:
53-yr-old woman, menopause at age 50 yr, lowest T-score -1.6, no risk factors, bisphosphonate therapy for 2 yr.
Treatment was never indicated in the first place and can be discontinued.

Bisphosphonate “Drug Holiday”
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.
Mild risk of fracture: treat with bisphosphonate for 3–5 yr and then stop.
Continue drug holiday until there is significant loss of BMD (i.e. more than the LSC) or the patient has a fracture, whichever comes first.

Bisphosphonate “Drug Holiday”
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.
Example- Mild risk of fracture:
65-yr old woman, menopause at age 52 yr, initial lowest T-score -2.6, no risk factors, bisphosphonate treatment for 5 yr, BMD stable over that time.
Treatment was indicated, but after 5 yr of treatment, a drug holiday might be considered.

Bisphosphonate “Drug Holiday”
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.
Moderate risk of fracture: treat with bisphosphonate for 5–10 yr
Offer a drug holiday of 3–5 yr or until there is significant loss of BMD or the patient has a fracture, whichever comes first.

Bisphosphonate “Drug Holiday”
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.
Example- Moderate risk of fracture:
70-yr-old woman, menopause at age 49 yr, lowest initial T score -2.7, no risk factors, bisphosphonate therapy for 8 yr, BMD increased over that time so lowest T-score now is -2.3.
Treatment was indicated, but after 8 yr of treatment, a drug holiday might be considered.

Bisphosphonate “Drug Holiday”
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.
High risk of fracture: treat with bisphosphonate for 10 yr
Offer a drug holiday of 1–2 yr until there is significant loss of BMD or the patient has a fracture, whichever comes first.
A non-bisphosphonate treatment (e.g. raloxifene, teriparatide) may be offered during the holiday from the bisphosphonate.

Bisphosphonate “Drug Holiday”
Watts N et al. J Clin Endocrinol Metab, April 2010, 95(4):1555–1565.
Example - High risk of fracture: 72-yr-old woman, menopause at age 43 yr,
lowest initial T-score -3.8, rheumatoid arthritis requiring ongoing corticosteroid therapy for 12 yr, 3-in. height loss and two vertebral fractures by VFA, treatment with bisphosphonate therapy for 10 yr
Treatment was indicated. After 10 yr, she remains at high risk of fracture.
If a holiday from the bisphosphonate is considered, interval treatment with teriparatide or raloxifene would be prudent.

Biochemical Markers of Bone TurnoverAACE 2010 Guidelines:
“Bone turnover markers may be used at baseline to identify patients with high bone turnover and can be used to follow the response to therapy”American Association of Clinical Endocrinologists Guidelines for Clinical Practice for the Diagnosis and Treatment of Postmenopausal Osteoporosis © 2010

Biochemical Markers of Bone TurnoverFormation
• Bone-specific alkaline phosphatase (BSAP)
• Osteocalcin (OC)
• Propeptide of type I collagen (P1NP)
Resorption• N-telopeptide of type I
collagen (NTX)
• C-telopeptide of type I collagen (CTX).
Bone Health and Osteoporosis: A Report of the Surgeon General.
Rockville, Md: US Department of Health and Human Services; 2004:187-217.

Biochemical Markers of Bone Turnover: Benefits Elevated bone turnover markers (BTMs)
predict more rapid rates of bone loss in certain groups of patients
Increased BTMs are associated with increased fracture risk independent of BMD at menopause and in elderly women
BTM markers respond quickly to therapeutic intervention
Changes in BTMs have been associated with bone response to therapy and reduction in fracture riskAmerican Association of Clinical Endocrinologists Guidelines for Clinical
Practice for the Diagnosis and Treatment of Postmenopausal Osteoporosis © 2010

Biochemical Markers of Bone Turnover: Limitations Limited by high in vivo and assay
variability (resorption markers) Poor predictive ability in individual
patients Lack of evidence-based threshold for
clinical decision making
American Association of Clinical Endocrinologists Guidelines for Clinical Practice for the Diagnosis and Treatment of Postmenopausal Osteoporosis © 2010

Biochemical Markers of Bone Turnover: Possible Uses Assessment of fracture risk in elderly
patients when elevated levels would influence the decision to begin pharmacotherapy
Early indicator of therapeutic response to anabolic or antiresorptive therapy
Evaluation of patients losing BMD despite antiresorptive therapy
Assessment of medication compliance, drug absorption, or therapeutic efficacy
American Association of Clinical Endocrinologists Guidelines for Clinical Practice for the Diagnosis and Treatment of Postmenopausal Osteoporosis © 2010

How often should Follow-up DXA be obtained? AACE Guidelines 2010: Obtain a baseline DXA Repeat DXA every 1 to 2 years until
findings are stable. Continue with follow-up DXA every 2
years or at a less frequent intervals. Follow-up of patients should be in the
same facility, with the same machine, and, if possible, with the same technologistAmerican Association of Clinical Endocrinologists Guidelines for Clinical
Practice for the Diagnosis and Treatment of Postmenopausal Osteoporosis © 2010

How often should Follow-up DXA be obtained? NEJM: Jan 19, 2012 4957 women, 67 years of age or
older, with normal BMD (T score at the femoral neck and total hip, −1.00 or higher) or osteopenia (T score, −1.01 to −2.49) followed prospectively for up to 15 years.
No history of hip or clinical vertebral fracture
No treatment for osteoporosisGourlay M et al. NEJM 366;3.

How often should Follow-up DXA be obtained? NEJM: Jan 19, 2012 Found that osteoporosis would develop in
less than 10% of older, postmenopausal women with DXA rescreening intervals of : 15 years for women with normal BMD or
mild osteopenia (T score greater than −1.49)
5 years for women with moderate osteopenia (T score −1.50 to −1.99)
1 year for women with advanced osteopenia (T score, −2.00 to −2.49).
Gourlay M et al. NEJM 366;3.

OSTEOPOROSISConclusion

Pharmacotherapy for osteoporosisSummary Antiresorptive and anabolic
therapies are available to manage osteoporosis
All have unique mechanisms to reduce fracture risk
Individual clinical trials may show differences in efficacy, however, the lack of head-to-head fracture trials prevents claiming superiority of one therapy over another

Pharmacotherapy for osteoporosisSummary Both oral as well as intravenous
bisphosphonates are available.
Bisphosphonates can reduce the risk for vertebral, nonvertebral, and hip fractures
IV bisphosphonates allow delivery without GI side effects, and assures drug delivery to bone in circumstances where absorption of oral bisphosphonates is uncertain

Pharmacotherapy for osteoporosisSummary Denosumab is an human monoclonal
antibody which is an antiresorptive through a different mechanism than bisphosphonates
Teriparatide stimulates bone formation and is especially useful in patients at high risk for fractures or who have not “responded” to alternative osteoporosis pharmacologic agents

The future of osteoporosis therapy• Improved understanding of the
regulators of bone remodeling and mediators of bone resorption and formation
• Modulate bone remodeling in ways that optimize skeletal health
• New agents that prevent bone loss and/or restore lost bone mass and bone quality that occurs due to age and disease

Thomas Repas DO FACP FACOI FNLA FACE CDE
Thank You!
Regional Medical Clinic- EndocrinologyAspen Centre640 Flormann Street- 3rd FloorRapid City, South Dakota 57701Office: 605 718 3300Email: [email protected] Blog: http://www.endocrinetoday.com/blogs.aspx
Top Related