







Languages
Pages
Legal

Sean M Bagshaw, MD, MScDivision of Critical Care Medicine
University of Alberta
The Use of Diuretics in
Acute Kidney

Disclosure
1.Consulting:1.Alere, Baxter, Gambro, Spectral Diagnostics, Otsuka
2.Speaking:1.Alere, Gambro, Otsuka

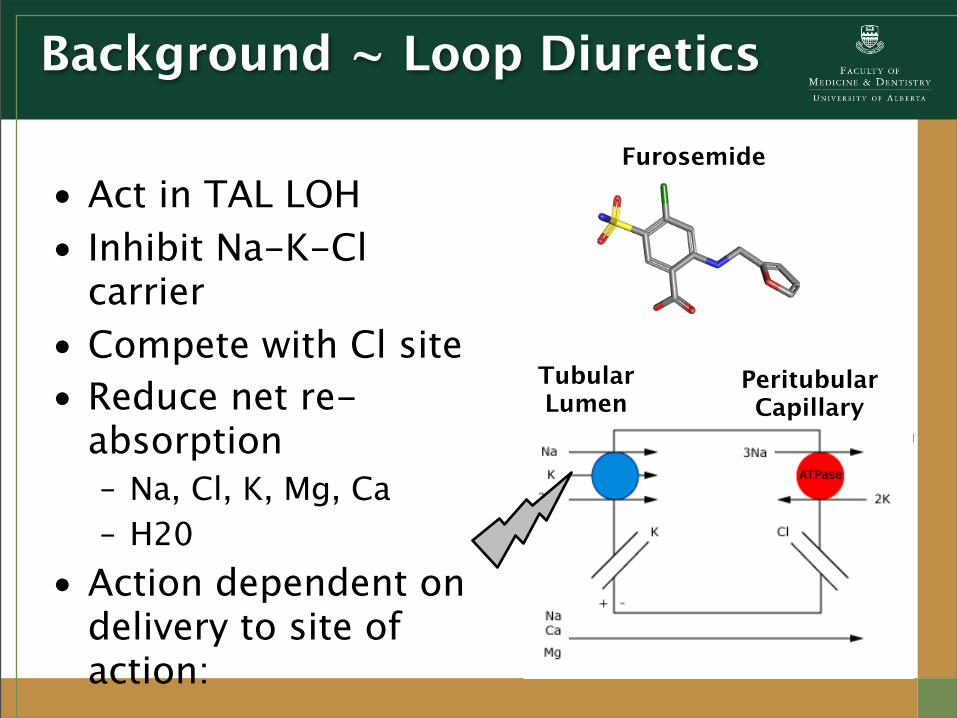
Background ~ Loop Diuretics
1.“Established AKI” in critical illness1.Few (if any) interventions2.Supportive
2.Many interventions require evidence:1.Better quality (i.e. randomized
trials)2.More applicable
Background ~ Loop Diuretics
• Act in TAL LOH• Inhibit Na-K-Cl
carrier• Compete with Cl site• Reduce net re-
absorption– Na, Cl, K, Mg, Ca– H20
• Action dependent on delivery to site of action:
Tubular Lumen
Peritubular Capillary
Furosemide

Rationale for Loop Diuretics
1.Direct renal vasodilator3.Attenuate medullary hypoxia by
inhibiting Na+/K+/2Cl- pump to reduce tubular O2 demand
5.Attenuate ischemic/reperfusion-induced apoptosis and associated gene transcription
7.Mitigate fluid overload/accumulationKramer et al KI 1980; Aravindan et al Ren Fail 2007; Aravindan et al Ren Fail 2006; Grams et al CJASN 2011

“Unload” the Stressed Kidney?
1.Acute renal failure = “acute renal success”
2.↓ in GFR (mediated by TGF) = ↓ reabsorptive work1.Preserve renal O2 supply/demand +
medullary oxygenation2.Mitigate ischemic/hypoxic injury
3.If protective - why do we apply strategies to ↑ GFR? Thurau et al Am J Med 1976

Variable Control Furosemide p-valueCardiac output (L/min) 5.6 6.1 <0.001Mean arterial pressure (mmHg)
80.2 80.6 NSRenal plasma flow (mL/min)
802 779 NSGFR (mL/min) 89.1 78.5 <0.001
Na reabsorption (mmol/min)
12.0 7.7 <0.001FeNa (%) 1.8 29.4 <0.001Urine flow (mL/min) 2.4 23.3 <0.001RVO2 consumption (mL/min)
11.1 7.9 <0.001O2 extraction (renal) (%) 10.5 8.5 <0.05
Sward et al ICM 2005
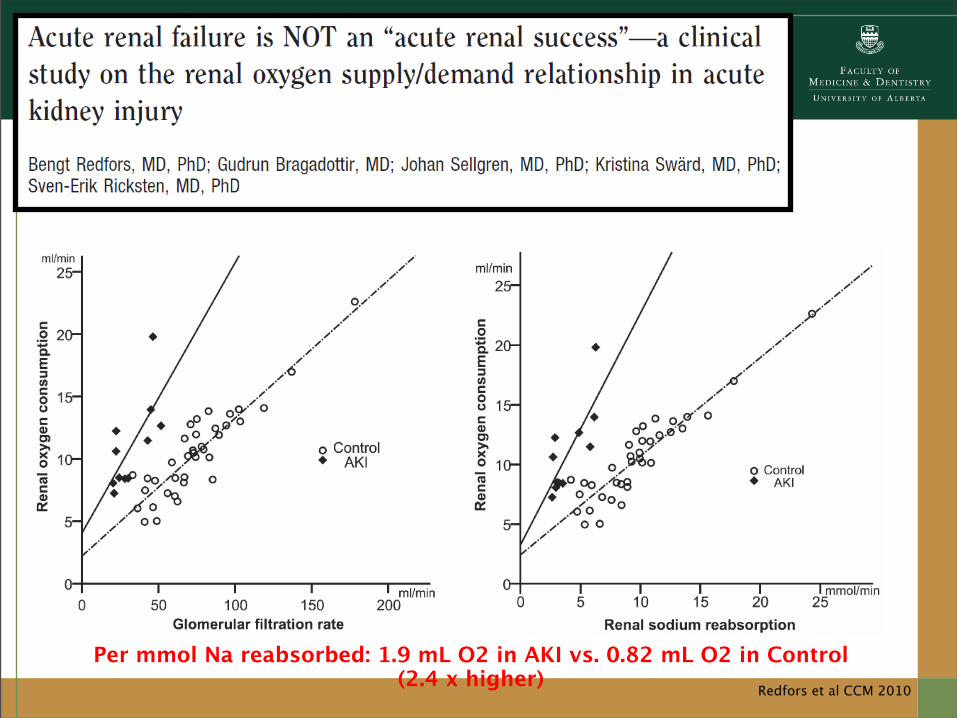
Redfors et al CCM 2010
Per mmol Na reabsorbed: 1.9 mL O2 in AKI vs. 0.82 mL O2 in Control (2.4 x higher)

Redfors et al CCM 2010
Per mmol Na reabsorbed: 1.9 mL O2 in AKI vs. 0.82 mL O2 in Control (2.4 x higher)
Mehta et al JAMA 2002
• Secondary retrospective analysis from the Project to Improve Care in Acute Renal Disease (PICARD) database:• Population: 552 (64%) critically ill patients
with AKI (defined as BUN>40 mg/dL, sCr>2 mg/dL or sustained rise >1 mg/dL above baseline)
• Intervention/Exposure: Diuretic use at any time in 7 days following nephrology consultation
• Outcome: Death, non-recovery, composite
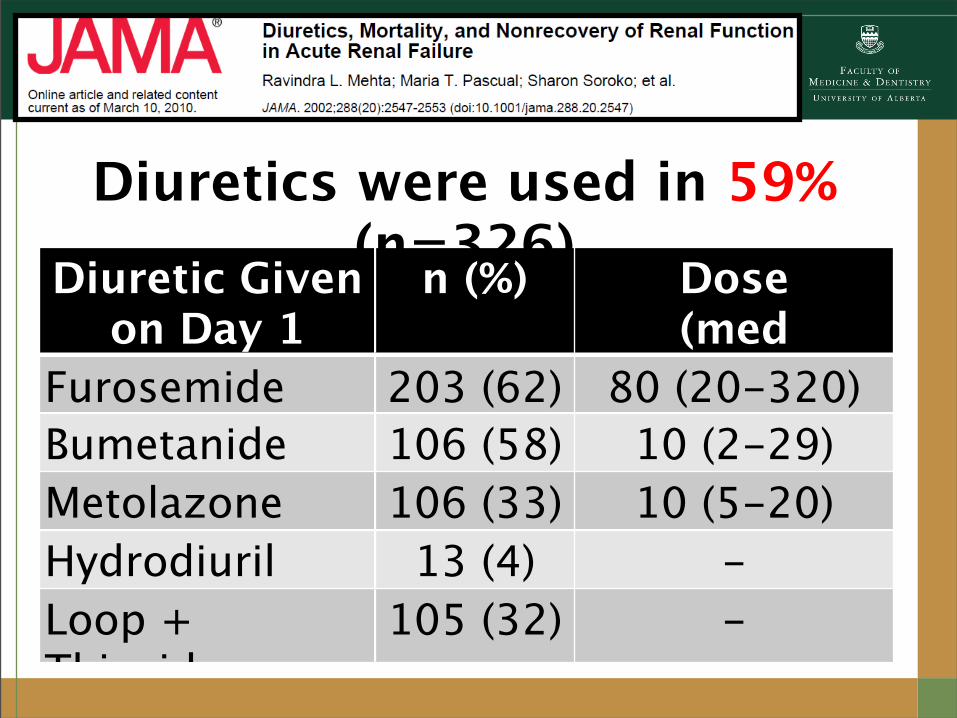
Diuretic Given on Day 1
n (%) Dose (med
[10-90th])Furosemide 203 (62) 80 (20-320)Bumetanide 106 (58) 10 (2-29)Metolazone 106 (33) 10 (5-20)Hydrodiuril 13 (4) -Loop + Thiazide
105 (32) -
Diuretics were used in 59% (n=326)

Mehta et al JAMA 2002
Variable Diuretic(n=226)
No Diuretic(n=326)
p
Age (yr) 58.1 (17.1)
53.8 (18.0)
<0.01History of CHF (n, %) 87 (27) 30 (13) <0.01Nephrotoxic (n, %) 61 (19) 28 (12) 0.05Respiratory Failure (n, %) 241 (74) 143 (64) 0.01Cardiac Failure (n, %) 148 (45) 75 (33) <0.01BUN (mg/dL) 61.6
(34.6)72.3
(43.4)<0.01
sCr (mg/dl) 3.6 (1.9) 4.1 (3.3) <0.01

Variable Crude OR (95% CI)
Adjusted OR
(95% CI)
Propensity-Adjusted
OR (95% CI)In-Hospital
Mortality1.37
(0.97-1.92)
1.65 (1.05-2.58)
1.68 (1.06-2.64)
Non-Recovery 1.53 (1.08-2.15
)
1.70 (1.14-2.53)
1.79 (1.19-2.68)
Composite 1.48 (1.02-2.12
)
1.74(1.12-2.68)
1.77 (1.14-2.76)
Composite (Ever/Never, n=416)
2.01 (1.26-3.20
)
3.15 (1.74-5.62)
3.12 (1.73-5.62)

Mehta et al JAMA 2002
Furosemide dose-equivalent (mg/mL urine output/d) as surrogate for “diuretic responsiveness” – median 0.34 mg/mL
DE (dark circle) > 1.0 mg/mL – OR 2.94 (1.6-5.4) DE (triangle) < 1.0 mg/mL
– OR 1.15 (0.8-1.7)

Mehta et al JAMA 2002

“The risk was borne largely by patients who
were relatively unresponsive to
diuretics”…and this
Mehta et al JAMA 2002

1. Secondary analysis of the Beginning and Ending Support Therapy (BEST) for the Kidney database:1. Population: 1,731 critically ill patients with
AKI (defined by: need for RRT; BUN>86 mg/dL, K>6.5 mmol/L; oliguria <200mL/12hr; anuria)
2. Intervention/Exposure: Diuretic use after study enrolment
3.Outcome: In-hospital death

Diuretic Use n (%)
Any diuretic use 1,117 (60.8)Furosemide 1,098 (98.3)Other loop diuretic 29 (2.6)Mannitol 22 (2.0)Metolazone 19 (1.7)Spirolactone 18 (1.6)Thiazides 14 (1.3)Other 14 (1.3)

Mehta et al JAMA 2002
Variable Diuretic(n=1,117)
No Diuretic(n=626)
Length of ICU stay 11 (5-22) 9 (4-20)
Length of Hospital stay
23 (12-45) 21 (9-44)
ICU Mortality (%) 53.4 48.2
Hospital Mortality (%)*
62.4 57.1
Discharge Dialysis 32.7 38.2
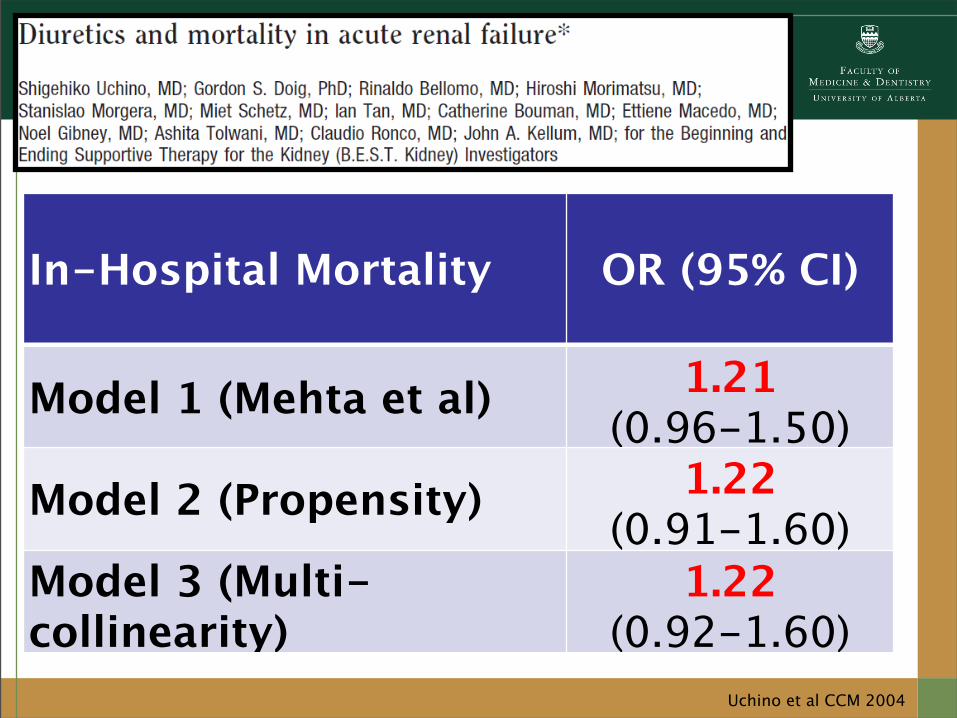
Uchino et al CCM 2004
In-Hospital Mortality OR (95% CI)
Model 1 (Mehta et al) 1.21(0.96-1.50)
Model 2 (Propensity) 1.22 (0.91-1.60)
Model 3 (Multi-collinearity)
1.22 (0.92-1.60)
PICARD/BEST Studies
1.Caveats to consider to these studies:1. Observational → Confounding2. Selection/information bias3. Severe/advanced AKI at inclusion
(sCr>3.5)*4. No data on specifics of fluid
resuscitation5. No data on fluid overload/
accumulation6. No data on timing of diuretic use

Bagshaw et al Crit Care Resusc 2007

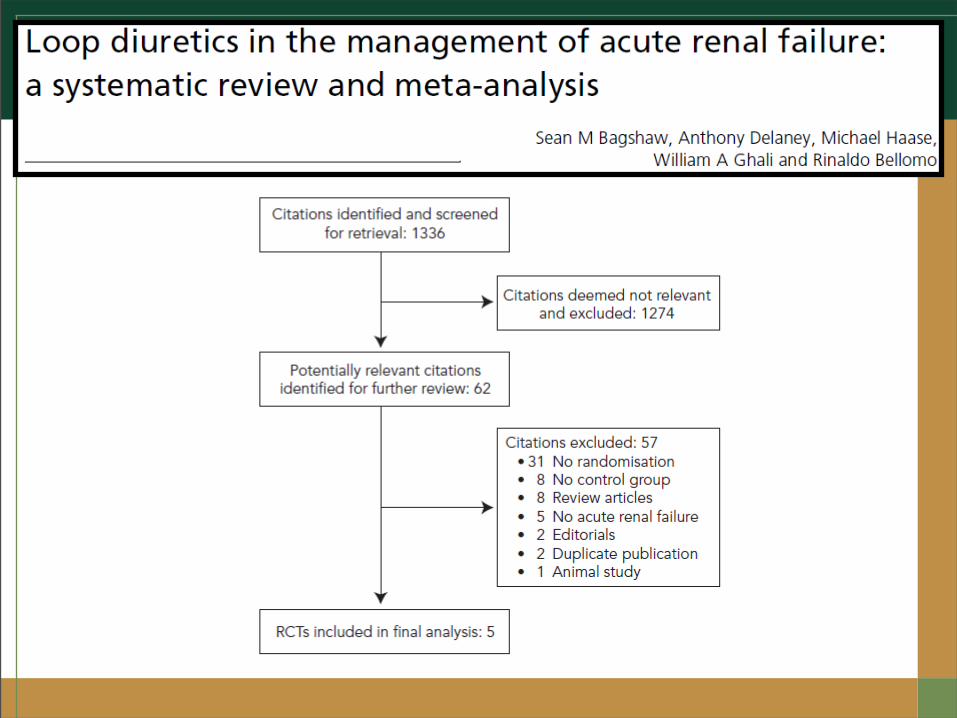
Mortality

Time to Normalize Creatinine/Urea
Time to Normalize SCr/Urea

Rate of Initiation of RRT
Rate of Initiation of RRT

Time to Achieve Diuresis >1500mL/day
Time to Achieve Diuresis >1500mL/day

Data generated from these trials:1. Low quality/reporting2. Single centre/small3. Co-interventions (dopamine, mannitol)4. Not all were critically ill5. Prolonged periods of oligo-anuria 6. Already receiving RRT7. High-dose bolus8. No titration to physiologic end-points

1.Questionable internal validity
3.Limited applicability to modern ICU practice
5.Low generalizability

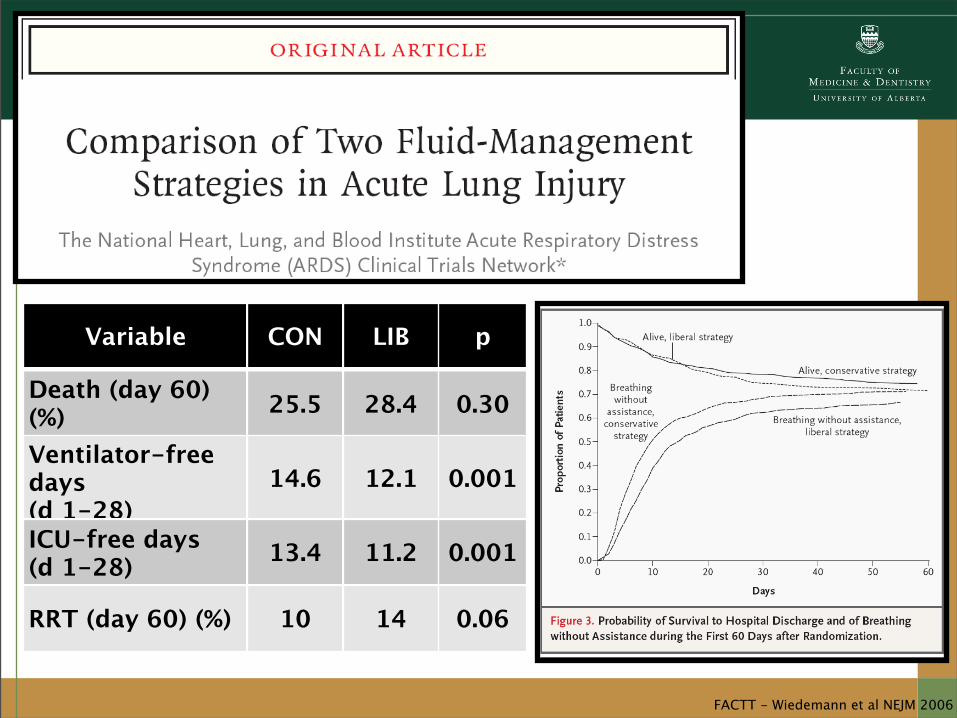
FACTT - Wiedemann et al NEJM 2006
Variable CON LIB p
Death (day 60) (%) 25.5 28.4 0.30
Ventilator-free days (d 1-28)
14.6 12.1 0.001
ICU-free days (d 1-28) 13.4 11.2 0.001
RRT (day 60) (%) 10 14 0.06

Grams et al CJASN 2011
Fluid balance (per L/day) on 60-day mortality
OR 1.61 (95% CI, 1.32-19.6, p<0.001)
CONSERVATIVE GROUP1. Less fluid!2. 0.9L vs. 2.2L per day,
p<0.0013. 6.0L vs. 10.2L 6-day
cumulative, p<0.001
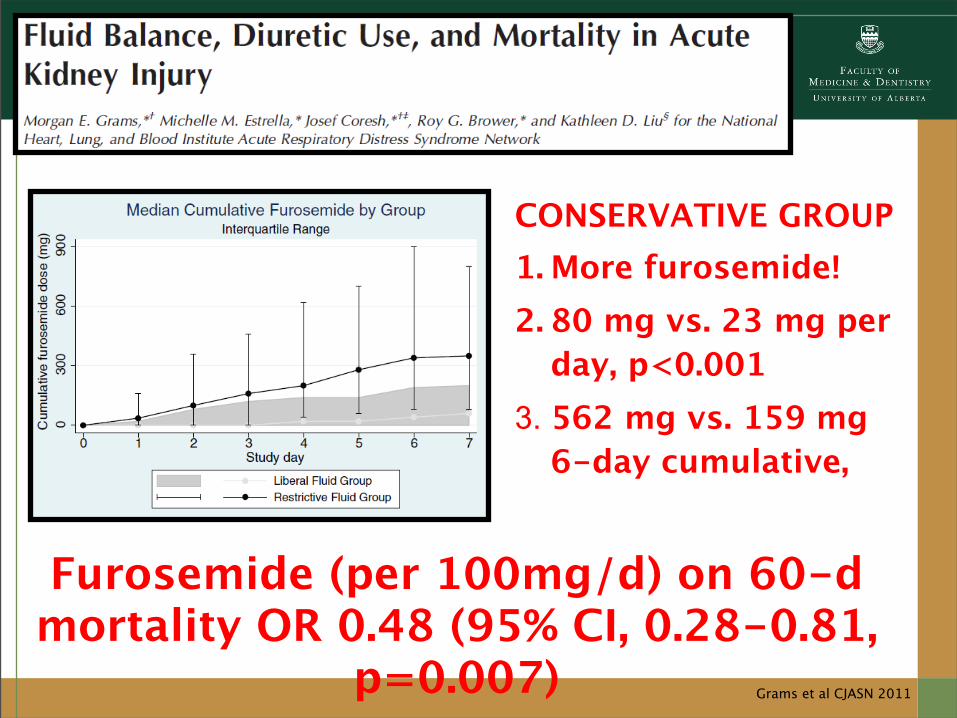
Grams et al CJASN 2011
Furosemide (per 100mg/d) on 60-d mortality OR 0.48 (95% CI, 0.28-0.81,
p=0.007)
CONSERVATIVE GROUP1. More furosemide!2. 80 mg vs. 23 mg per
day, p<0.0013. 562 mg vs. 159 mg
6-day cumulative,

Van der Voort et al CCM 2009
FUR(n=36)
PLAC(n=35
)p
Urine Output (mL/
hr)247 117 <0.0
1
Urine [Na](mmol/L) 73 37 <0.0
1
Recovery (%) 69.4 77.1 0.5
Iso-volemic furosemide infusion
(0.5 mg/kg/h)vs. placebo

Trial Design
The SPARK Study: A randomized controlled
trial of furoSemide in critically ill Patients with
eARly acute Kidney injuryClinicalTrials.gov Identifier:
NCT00978354
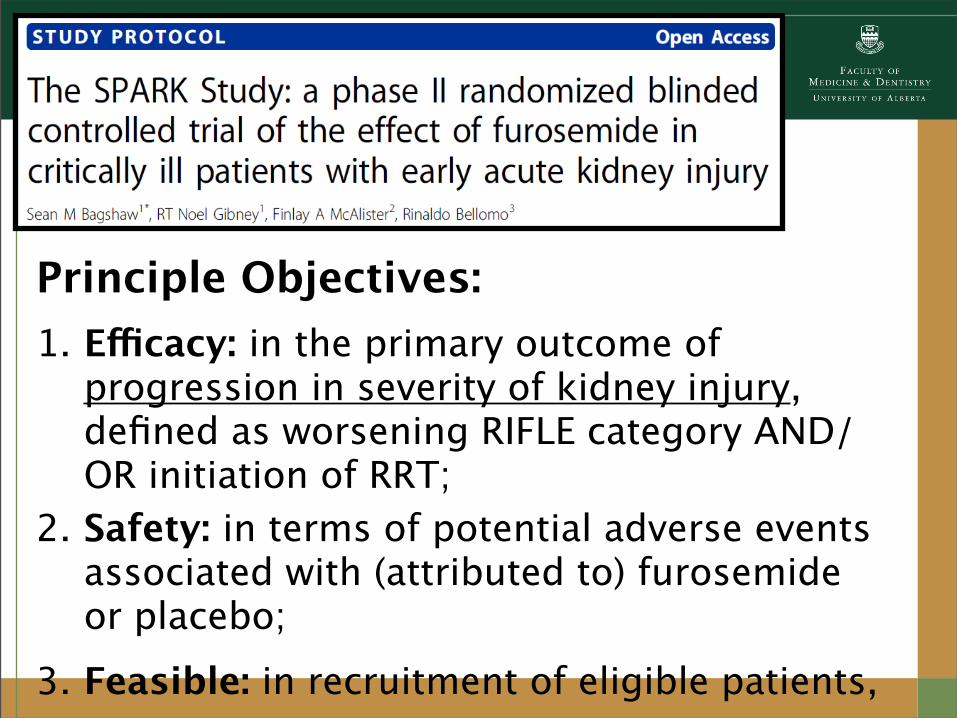
Principle Objectives:1. Efficacy: in the primary outcome of
progression in severity of kidney injury, defined as worsening RIFLE category AND/OR initiation of RRT;
2. Safety: in terms of potential adverse events associated with (attributed to) furosemide or placebo;
3. Feasible: in recruitment of eligible patients,
Secondary Clinical Objectives:1. Fluid balance, electrolyte and acid-base
homeostasis2. Duration of AKI3. Initiation of renal replacement therapy4. Composite of major adverse kidney events
[MAKE] ~ 1.Recovery of kidney function AND/OR2.New or worse chronic kidney disease (CKD) AND/
Summary
1.Furosemide use is common in AKI3.Data is conflicting on it efficacy5.There is misalignment between
evidence and clinical practice7.There is equipoise for a randomized
trial9.The SPARK Study proposes to
generate higher quality data to guide on this issue
Top Related