






Languages
Pages
Legal


The Treasure Hunt—Keys to Unlocking Radiology Reimbursement
Patricia Kroken, FACMPE, CRARadiology Business Management Association (RBMA)

The cost of poor performance
Not unusual for a group with process inefficiencies to leave $250,000 - $500,000 on the table
Process problems raise the ante--$1 million
What would it mean if your group could increase the revenue per procedure by $3.00? $5.00?

How hard can it be?
Patient Information Entered
Insurance claim
submitted
Payment
•Front Desk•Scheduling •Billing

The Reality
Patient Information
Entered
Insurance claim
submitted
Claim denial for error
Denial assigned for follow-up
Research: pull film jacket and/or call
patient
Correct claim and resubmit
Payment
•Front Desk•Scheduling
•Billing

Where do practices lose money?
Charge captureCoding documentationClaims submission (clean claims)Insurance follow-upDenials managementPrivate pay follow-up

Charge capture
Sort and Match
Charge Entry
Coding
Demographics Radiology Reports
What happens when there is no match?
Reports with no demos
Demos with no reports

Charge capture
Usually a manual process The “stacks” build Reconciliation is very difficult
Technology is helping solve problems Document scanning Electronic “matching” Edit reports of missing information

Coding documentation
Dictation does not support codesMedical necessity denials
Need understanding of Medicare Local Coverage Determinations
Feedback from billing/coding to radiologists
Ensure credit for what was done—but if it isn’t documented, it did not happen!

Claims submission
Technology = success Edit reports Corrections of claims prior to submission
Must also be able to follow up on claims status Payor Clearinghouse Manual processes or lack of technology
problematic

Insurance follow-up
Most difficult process area to manageUsually dependent on the individual
Organization Work habits Ability to prioritize
Workloads frequently unrealistic Commercial insurance Workers comp, MVA, Medicaid

Insurance follow-up
More of an issue with hospital based practices Inherent poor quality of hospital information Denials for eligibility require
• Obtaining correct information• Refiling to the correct carrier• Completing the process within filing limits

Insurance follow-up
Insurance “correspondence” Often set aside due to workloads “Easy money”
A/R reports usually assigned by payor class Dollar amounts not necessarily
representative of work involved Number of claims

Insurance follow-up
Secrets to success Assign priorities
• Dollar amount• Age of account
– Balance working old and new A/R buckets
Work correspondence daily Document scanning
• Move work onto workstations and out of filing cabinets

Denials management
Phases of denials management Appeal of denied claims Root cause correct to reduce/eliminate
denials

Denial categories
Missing/incorrect informationPatient eligibilityPrior AuthorizationDuplicate claimsFiling deadlinesCoding
Bundled/unbundled claims Lack of specificity in ICD-9 coding Failure to “match” ICD-9 and CPT codes
Medical necessity/non-covered services

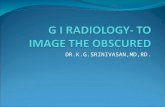
Denial trends
Internal Denial Tracking
Medical necessity16%
Duplicate10%
Missing/incorrect data35%
Other10%Pending
12%
Eligibility6%
Coding1%
Timely Filing10%

Denials management actions
Prioritize: which correction would result in the greatest impact?
Identify the source Work to correct operational problems
Training/resource issues Process “drops” Technology limitations Dictation/transcription

Drilling down denials
Distribution of denials by Type (timely filing, etc.) Site Modality Radiologist Referring physician Inpatient, outpatient, ER Time of day/day of week

Private pay follow-up
Often overlooked as revenue enhancement opportunity Patients “too expensive” to follow-up because they
“don’t pay their bills anyway”
Fertile ground for hospital-based group Patients classed as uninsured or private pay often
have insurance• Will ignore statements because “they provided that information
at the hospital”• Respond to collection letter—too late to file a claim

Passive collection processes
Passive = patient must do the work Respond to statement or letter
Series of statements mailedCollection lettersTurn to collection agency

Active collection processes work!
Initiate phone calls to hospital patients with balances in excess of $100 Do they have insurance? Would they like to pay by credit card? Would they like to be put on payment plan? Do they qualify for financial assistance?
Private pay collector can generate $250,000 or more per year May be able to set up “pass through” arrangement
with billing service

Process improvement
Radiology is comprised of a series of processes Scheduling/registration Performance of procedure Billing/collections
Correction of process problems will increase revenue…period.

To obtain copies of presentation
www.radconsultants.com

Thank you! Questions?
Patricia Kroken, FACMPE, CRA
Healthcare Resource Providers, LLC
P.O. Box 90190
Albuquerque, NM 87199
505/856-6128
www.radconsultants.com
Top Related