







Languages
Pages
Legal


The Key to Success: INTERMACS Hospitals
• Site Utilization of INTERMACS Data and Reports for local QI
• Quality Assurance and data quality
• Evaluation of Site Data: Audits, Complete Enrollment, Complete Data, etc.
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

The Key to Success: INTERMACS
Hospitals!
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

The Key to Success: INTERMACS Hospitals
•Site Utilization of INTERMACS Data and Reports for local QI Naftel
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

Hospitals
• What services do the hospitals receive for their participation fee?• Services
• Meets CMS/Joint Commission requirement for Destination Therapy Certification
• Meets FDA required submission of Medical Device Reports (MDRs) by hospitals
• Provides clinical summaries of patients• Provides quality assurance reports• Provides electronic data transfer• Provides standardized datasets• Provides benchmarking• Provides training and continuing education units
INTERMACS A
nnual Meetin
g
March 2012

Hospitals (Continued)
• What benefits do the hospitals receive for their participation fee?• Benefits
• Fulfills CMS DT Certification requirement• Become part of the national dialogue on the evaluation
and evolution of MCSDs• Invited to participate in the INTERMACS Annual
Meeting• Invited to join the INTERMACS Committees
• Coordinators Council and other committees• Select Hospital Administrators will have the opportunity
to serve on the Business Advisory Committee
INTERMACS A
nnual Meetin
g
March 2012

The Key to Success: INTERMACS Hospitals
•Quality Assurance and data quality Naftel
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

Hospital Perspective – Deliverables
CoordinatorsClinical TeamQuality Assurance OfficerOffice of Risk ManagementFinancial Officers / AdministratorsOffice of AccreditationResearchers
Fifth Annual Meeting, April 12, 2011
INTERMACS A
nnual Meetin
g
March 2012

A Workshop for Researchers and INTERMACS Hospitals
QA Report
8 INTERMACS Data Workshop – April 12, 2011
INTERMACS A
nnual Meetin
g
March 2012
A Workshop for Researchers and INTERMACS Hospitals
QA Report
9 INTERMACS Data Workshop – April 12, 2011
INTERMACS A
nnual Meetin
g
March 2012

A Workshop for Researchers and INTERMACS Hospitals
10 INTERMACS Data Workshop – April 12, 2011
INTERMACS A
nnual Meetin
g
March 2012

A Workshop for Researchers and INTERMACS Hospitals
11 INTERMACS Data Workshop – April 12, 2011
INTERMACS A
nnual Meetin
g
March 2012

The Key to Success: INTERMACS Hospitals
•Evaluation of Site Data: Audits, Complete Enrollment, Complete Data, etc. Naftel
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012
1. Regulatory Requirements Regulatory requirements must be met. Assessment: UNOS collects and the DCC evaluates all regulatory documents Goal: 100% of participating hospitals meet all regulatory requirements Minimal Standard: 100%
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

133 Activated Sites (currently 131)
1,705 INTERMACS Personnel
1,267 IRB Approvals since 2006
1,590 Informed Consent, HIPAA, Revoke Authorization, Transfer, Blood / Tissue documents
1,490 Human Subjects Training Certificates
1,805 Financial Disclosure / Conflict of Interest
Coordinator Training, March 11, 2012
INTERMACS A
nnual Meetin
g
March 2012

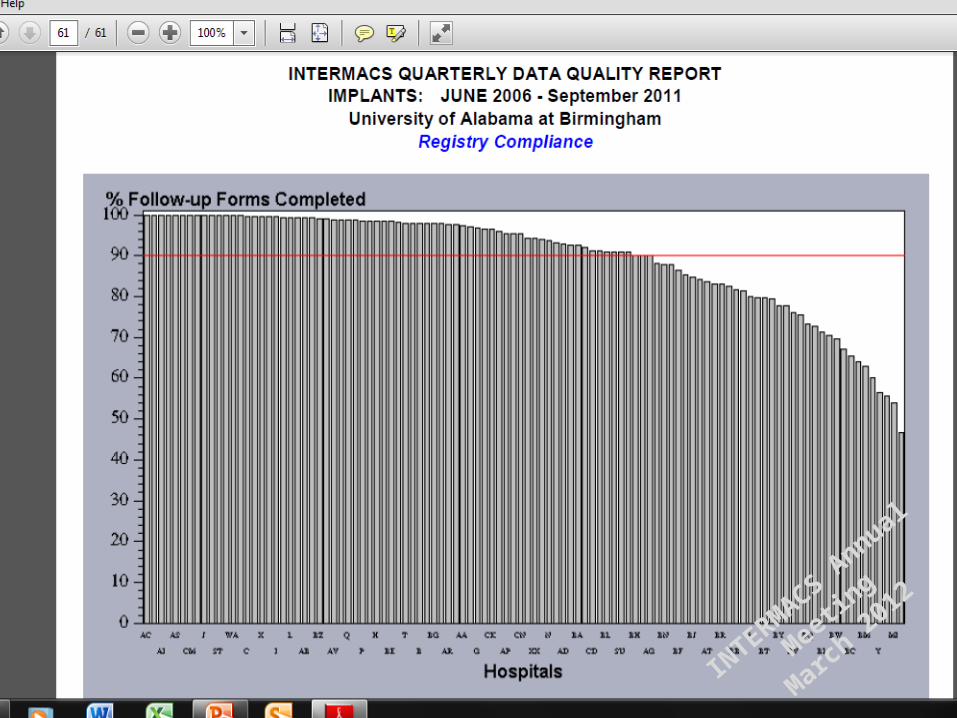
2. Timely Follow-up data Assessment: will focus on submission of follow-up forms. Goal: 100% of follow-up forms submitted within 30 days of the date of expected follow-up. Minimal Standard: 90% of follow-up forms must be submitted within 30 days of the date of expected follow-up
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012
Coordinator Training Session: March 11, 2012
Overview of Data Entry Naftel
16
INTERMACS A
nnual Meetin
g
March 2012

3. All Device Implants Complete Accounting of all eligible device implants. Assessment: Matching hospital enrollment to industry counts. Goal: 100% of eligible devices enrolled. Minimal Standard: 90% of eligible devices enrolled. Note1: All eligible DT devices must be entered. Note2: Informed consent is a barrier to the minimal standard.
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

Days from Implant to Entry into INTERMACS
Jun 2006 – Dec 2011
Sixth Annual Meeting, March 12, 2012
Median (days) n %< 30 50 40%30 – 59 30 24%60 – 89 13 10%90 – 119 6 5%> 120 26 21%Total hospitals 125 100%
INTERMACS A
nnual Meetin
g
March 2012

Days from Implant to Entry into INTERMACS
Jun 2006 – Dec 2011
Sixth Annual Meeting, March 12, 2012
Median (days) n %< 30 50 40%30 – 59 30 24%60 – 89 13 10%90 – 119 6 5%> 120 26 21%Total hospitals 125 100%
INTERMACS A
nnual Meetin
g
March 2012

4. Completeness of data elements
Assessment: The web-based application requires that all elements be addressed (either a data value entered or “not done” selected) before the form can be submitted. The proportion of captured data values will be calculated. Goal: 100% completion of data elements. Minimal Standard: To be determined after consultation with HSC.
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

Completeness of Quality of Life Data will be addressed by
Dr. Grady
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

The Key to Success: INTERMACS Hospitals
•Risk adjustment:
Will require an in-depth, collaborative effort among the INTERMACS Collaborators including hospital representatives. The approach will be modeled after the SRTR evaluation of post heart transplant survival.
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

Update on New INTERMACS/NIH Initiatives
• MedaMACS• PumpKIN• PediMACS• IMACS• Revive-IT
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

Update on New INTERMACS/NIH Initiatives
• MedaMACS (15 min) Stewart
Sixth Annual Meeting, March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

MEDAMACS Update 2012:MEDAMACS Update 2012:
Medical Arm of Mechanical Medical Arm of Mechanical Circulatory SupportCirculatory Support
INTERMACS - 6th Annual Meeting
March 12, 2012
INTERMACS A
nnual Meetin
g
March 2012

The MEDAMACS MissionThe MEDAMACS Mission
• Map terrain of ambulatory advanced heart failure
• Improve selection and timing of MCS by studying outcomes with medical therapy
• Support IOM mandate for patient-centered care and shared decision making
• Design integrated endpoints that move beyond survival alone
• Define a broader context for the next generation of MCS clinical trials
INTERMACS A
nnual Meetin
g
March 2012

Evolution of MEDAMACS
INTERMACSSpecific Aim
2006, 2011
MEDAMACSMEDAMACSStudyStudy
2012-20152012-2015
n=350n=35012 centers12 centers
2 yrs follow-up2 yrs follow-up
Screening PilotScreening Pilot
2010-122010-12
n=168n=16810 centers10 centers
1 yr follow-up1 yr follow-up
INTERMACS A
nnual Meetin
g
March 2012

Brigham and Women’s U. of Alabama Birm. U. of PittsburghCedars-Sinai U. of Colorado U. of PennsylvaniaCleveland Clinic U. of Iowa U. of South FloridaDuke U. of Michigan U. of Texas Southwestern
MEDAMACS Study Sites
INTERMACS A
nnual Meetin
g
March 2012

MEDAMACSMEDAMACS ROADMAPROADMAP11 REVIVE-ITREVIVE-IT22
SizeSize 350 100 ~50
DesignDesign Prospective observational,
OMM only
Prospective observational,
Thoratec HM2 vs. OMM
Randomized trial,
Heartware HVAD vs. OMM
Inclusion Inclusion CriteriaCriteria
HF symptoms >12m
NYHA III-IV
Optimal med rx
≥1 HF admission in 12m
AND one
1.) Additional HF Hosp
2.) Peak VO2 <16 men, or <14 women
3.) BNP >1000
4.) 6MW <300m
5.) SHF Score ≥ 1.5
EF ≤35%
Can be eligible for transplant, but not listed
NYHA IIIB-IV
≥1 HF hospitalization in 12m, or 2 unscheduled EW visits for HF
6MW <300m
EF ≤25%
Not currently listed, not planned in 12m
HF symptoms >12m
NYHA III for 3m
Optimal med rx
≤1 HF hosp within 6m, no admit in 30d
CRT if QRS >120
Peak VO2 < 16men, <14women
6MW <350m
SHF Score ≥ 1.5
EF ≤35%
Not a transplant candidate
LVAD candidate by CMS criteria
1. clinicaltrials.gov/NCT014528022. clinicaltrials.gov/NCT01369407IN
TERMACS Annual M
eeting
March 2012

MEDAMACSMEDAMACS ROADMAPROADMAP11 REVIVE-ITREVIVE-IT22
Exclusion Exclusion criteriacriteria
Non-cardiac diagnosis limits prognosis ≤2 yrs
Current inotrope use
Listed for transplant
QRS >120 and planned CRT, or CRT within 3m
Other condition that limits survival to ≤2 yrs
Inotrope in 30d
Listed for transplant
Inability to perform 6MW
Severe illness limiting prognosis to ≤2 yrs
STEMI within 3m
Inotrope within 3m
GFR <30, cerebrovasc dz
A transplant candidate
Plt <100K, alb <3, PVD
CRT if QRS >120 must have been >90d previously
Liver, pulm dysfunction
Mechanical AVR
PVR >6 Wood units
EndpointsEndpoints Primary at 1 yr
Integrated endpoint of survival, requirement for advanced therapies, functional capacity, QOL, patient preferences
Primary at 1yr
Survival at 1yr with improvement of at least 75m in 6MW
Actuarial survival and survival free of stroke
Primary at 2 yrs
Composite of survival, freedom from moderately disabling stroke, and 6MW improvement >75m
1. clinicaltrials.gov/NCT014528022. clinicaltrials.gov/NCT01369407IN
TERMACS Annual M
eeting
March 2012

6MWGait speed
Euroqol+KCCQVAD Survey
EventsRisk ScoresTreatments
BaselineB
MEDAMACS Encounters
Inpt oroutpt
1 MonthRe-Look Baseline
6 mosPhone
Interview
1 YrFace-to-face
18m 2 Yrs PhoneInterview
outptA B
CTimeZero
D
Telephone ContactTelephone Contact
6MWGait speed
Euroqol+KCCQVAD SurveyRisk Scores
6MWGait speed
Euroqol+KCCQVAD Survey
EventsTreatments
BaselineA
6MWGait speed
Euroqol+KCCQVAD Survey
EventsRisk ScoresTreatments
Study Site Phone Calls 6 and 18 mosEvents (hosp, stroke, transplant, vad, inotropes, death)
Meds, Euroqol, NYHA/INTERMACS profile
Onemonth
Consent 1mo. 12mos 24mos
Fac
e-to
-fac
e
enco
un
ters
End1-Yr Visit
C2-Yr Visit
D
INTERMACS A
nnual Meetin
g
March 2012

MedaMACS Pilot
2012 2013 2014 2015
EnrollmentN=350 x 12sites
Design MedaMACS 2.0
2016
OS
MB
Re
vie
w &
DC
C I
RB
(11
-12
/20
11
)
6M Telephone 18M Telephone
1 Year Visit
2 Year Visit & Closeout
WB
DE
Pro
gra
mm
ing
Do
ub
le B
as
eli
ne
sC
om
ple
ted
DA
TA
BA
SE
CL
OS
ED
1 Y
r D
ata
C
om
ple
te
IRB
ST
UD
Y S
ITE
S
TU
DY
SIT
E
DC
C +
ST
EE
RIN
GD
CC
+ S
TE
ER
ING
MEDAMACS Timeline
Pil
ot
Co
mp
lete
La
te-B
rea
kin
gS
ub
mis
sio
n
Ba
se
lin
e D
ata
IS
HL
T/A
CC
Fin
al P
ilo
t A
nal
ysis
SpringTraining
Annual Mtg@ISHLT
Annual Mtg@ISHLT
Annual Mtg@ISHLT
La
te-B
rea
kin
gS
ub
mis
sio
n
6M D
ata
Co
mpl
ete
Estimated # Active Pts 0 90 160 250 270 260 250 235 210 180 150
ISHLT
INTERMACS A
nnual Meetin
g
March 2012
MEDAMACS at ISHLT 2012:Screening Pilot Data
• High Event Rates in Medically Managed Advanced Heart Failure Patients Followed at VAD Centers (Stewart et al.)
• Prediction of Events in Patients with Advanced Heart Failure: Application of the Seattle Heart Failure Model to the Medamacs Population (Teuteberg et al.)
• Patients with INTERMACS 4-7 Heart Failure Have Reduced Quality of Life (Patel et al.)
• Uric Acid Elevation is Associated with Severity of Congestion in Advanced Heart Failure (Guglin et al.)
• Tricuspid Regurgitation is a Measure of Right Heart Dysfunction and is Associated with Event Free Survival in Stage D Heart Failure (Testani et al.)
INTERMACS A
nnual Meetin
g
March 2012

Ev
ent-
Fre
e S
urv
iva
l
0
25
50
75
100
0 2 4 6 8
Months since Enrollment
Death
Death, Transplant,or VAD
Death, Transplant,VAD or Inotrope
68%
64%
84%
Event-Free Survival in AmbulatoryAdvanced Heart Failure
Event of Interest
Stewart et al. ISHLT 2012INTERMACS A
nnual Meetin
g
March 2012

Su
rviv
al F
ree
of
VA
D o
r T
ran
spla
nt
0
25
50
75
100
0 2 4 6 8
Months since Enrollment
INTERMACS Profiles Risk Stratify AmbulatoryAdvanced Heart Failure Patients
INTERMACS 6/7
INTERMACS 5
INTERMACS 4
P<0.001
Stewart et al. ISHLT 2012INTERMACS A
nnual Meetin
g
March 2012

0
20
40
60
80
100
Eve
nt-
free
su
rviv
al (
%)
0 3 6 9
Months post-enrollment
SHFM < 1.5 SHFM 1.5-2.5 SHFM > 2.5
p = 0.0003
by Seattle HFM categoryEvent-free Survival
Teuteberg et al. ISHLT 2012REVIVE-IT INTERMACS A
nnual Meetin
g
March 2012

Euroqol VAS Score by HF SeverityEuroqol VAS Score by HF Severity
INTERMACS; Grady K, et al J Heart Lung Trans 2009;28:S269.MEDAMACS: Patel P, et al. ISHLT 2012.HF Action; Flynn K, et al. Am Heart J 2009;158:564-71.IN
TERMACS Annual M
eeting
March 2012
Investigator SiteAmrut Ambardekar U Colorado
Chetan Patel Duke
Eddie Rame U Penn
Frances Johnson U Iowa
Garrick Stewart Brigham and Women's
Jeffrey Testani U Penn
Jeffrey Teuteberg U Pitt
Jennifer M. Cowger U Michigan
JoAnn Lindenfeld U Colorado
Jon Kobashigawa Cedars-Sinai
Joseph Rogers Duke
Keith Aaronson U Michigan
Leslie Miller U South Florida
Lynne Stevenson - PILynne Stevenson - PI Brigham and Women's
Maria Mountis Cleveland Clinic
Mariell Jessup U Penn
Mark Drazner U Texas Southwestern
Maya Guglin U South Florida
Michele Hamilton Cedars-Sinai
Michelle Kittleson Cedars-Sinai
Parag Patel U Texas Southwestern
Randy Starling Cleveland Clinic
Salpy Pamboukhian U Alabama Birmingham
Team MEDAMACS
UAB/DCC UAB/DCC David NaftelMary Lynne ClarkSusan MyersCraig CollumKathryn Hollifield
NHLBI/NIHNHLBI/NIHMonica ShahTim BaldwinMarissa Miller
Thoratec CorporationThoratec Corporation
INTERMACS A
nnual Meetin
g
March 2012

Coordinator Training Session: March 11, 2012
pediMACS
David C. Naftel, PhD
39
INTERMACS A
nnual Meetin
g
March 2012

Coordinator Training Session: March 11, 2012
INTERMACS Re-Launch Status
Our Goals: Reduce the number of elements and forms Streamline the data entry process Clarify elements that were confusing in the past Examine the AE definitions for current clinical
relevance
40
• It became clear that the pediatric VAD patients needed a different web-based data entry system.
INTERMACS A
nnual Meetin
g
March 2012

Coordinator Training Session: March 11, 2012
pediMACS Launch Status
Pediatric Committee Betsy Blume, MD - Chair David Morales, MD David Rosenthal, MD Peter Wearden, MD Christopher Almond, MD Robert Jaquiss, MD Jonathan Chen, MD Dee Dee Epstein, RN Heidi Moses, MEd, CCRA David Naftel, PhD Tim Baldwin, PhD
41
INTERMACS A
nnual Meetin
g
March 2012

Coordinator Training Session: March 11, 2012
pediMACS Launch Status
42
We (Pediatric Committee, NIH, INTERMACS Co-PIs) have spent 1 year reviewing the WBDE in all aspects: AE definitions and other definitions Screens / Forms Data Elements Patient Flow through the WBDE
INTERMACS A
nnual Meetin
g
March 2012

Coordinator Training Session: March 11, 2012
pediMACS Launch Status
43
pediMACS will follow the structure of INTERMACS
A few important changes from INTERMACS: Pediatric patients (< 19 yrs. at time of implant) Includes both durable and temporary support
MCSDs Modifications of AE definitions Possible expansion of quality of life instruments
INTERMACS A
nnual Meetin
g
March 2012

Coordinator Training Session: March 11, 2012
pediMACS Launch Status
44
Target Live test site: July 1, 2012 Testing by INTERMACS Nurse Monitors Testing by the DCC Data Managers Testing by the INTERMACS Co-PIs Testing by 3 Hospitals (Beta Sites) Testing by Pediatric Committee
Target Launch Date: August 1, 2012 Online training will be available Training Session in September 2012
Target: Live Test Site
July 1, 2012
Target: LAUNCH Date
Aug 1, 2012Jul 1 - Jul 31
INTERMACS A
nnual Meetin
g
March 2012

Coordinator Training Session: March 11, 2012
pediMACS Launch Status
45
Training Session for pediMACS “Mechanical Cardiac Support in Pediatric Heart Disease –
State of the Art 2012”: September 20-22, 2012 The St. Louis Children’s and Washington University
Heart Center
INTERMACS A
nnual Meetin
g
March 2012
Top Related