






Languages
Pages
Legal

The journey of HPV vaccine : From Study to Real world experience

Burden of HPV-related diseases
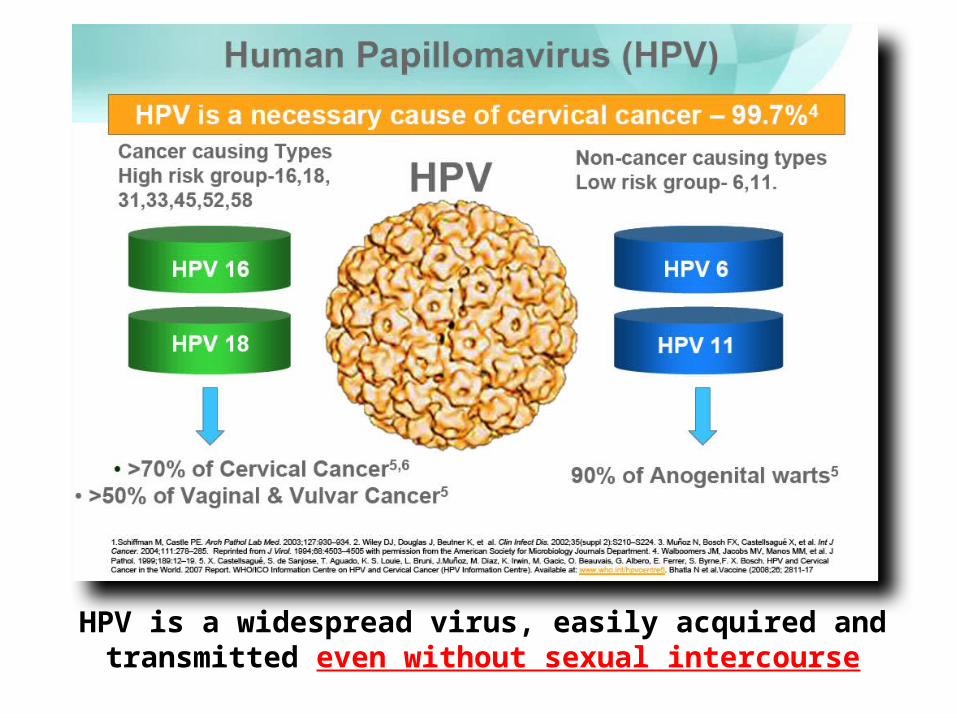
HPV is a widespread virus, easily acquired and transmitted even without sexual intercourse

High HPV Disease Burden AmongMales and Females Globally
Male Female
Penile cancer 1 10,500
19,960 Vulvar & vagina cancer 2
Head and neck cancer 2 Head and neck cancer 2
529,800
Anal cancer 1 Anal cancer 1
Cervical cancer 2
8,500,000High-grade
cervical dysplasia 3
22,800,000Low-grade
cervical dysplasia 3
17,600,000 14,400,000 Genital warts 4Genital warts 4
13,000 14,300
42,000 18,000
Estimated annual new HPV-related disease cases in males and females globally
1. Parkin DM et al. Vaccine. 2006;24(Suppl 3):S3/11–S3/25. 2. WHO/ICO Information Centre on HPV and Cervical Cancer (HPV Information Centre). Human Papillomavirus and Related Cancers in World. Summary Report 2010. 3. World Health Organization. Geneva, Switzerland:
World Health Organization; 1999:1–22. 4. World Health Organization (WHO). Executive summary: the state of world health. 1995. http://www.who.int/whr/1995/media_centre/executive_summary1/en/index3.html#. Accessed June 7, 2012.
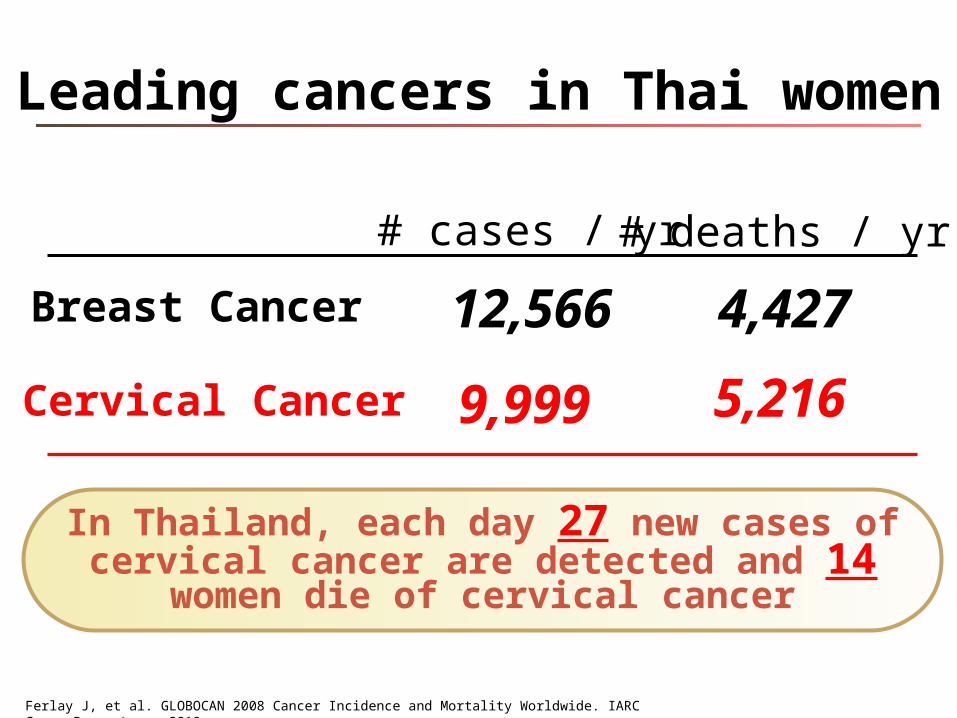
Leading cancers in Thai women
Breast Cancer
Cervical Cancer
# cases / yr # deaths / yr
12,566 4,427
9,999 5,216
Ferlay J, et al. GLOBOCAN 2008 Cancer Incidence and Mortality Worldwide. IARC CancerBase; Lyon, 2010.
In Thailand, each day 27 new cases of cervical cancer are detected and 14 women die of cervical cancer

How to evaluate HPV vaccineefficacy in clinical trials

Disease prevention (CIN 2, 3 & AIS) is the only accepted clinically relevant measure of efficacy
Regulatory Agency
Persistent HPV
InfectionCIN 1
CIN 2/3 or AIS
USA FDA NO NO YES
EU NO NO YES
WHO NO NO YES
No mention about antibody level !!!
WHO guideline 2006

Seropositivity*
Efficacy against HPV 18-related CIN 2/3 or AIS
*Seropositivity to HPV 18 neutralising antibodies to a single neutralising epitope measured by cLIA
99%
71% 68%60%
100% 100% 100%
0
20
40
60
80
100
6-10 months 2 year 3 year 4 year
%No correlation between antibody level vs efficacy
seen in HPV4 clinical trial
Joura A, et al. Vaccine. 2008;26:6844-51
Efficacy in women
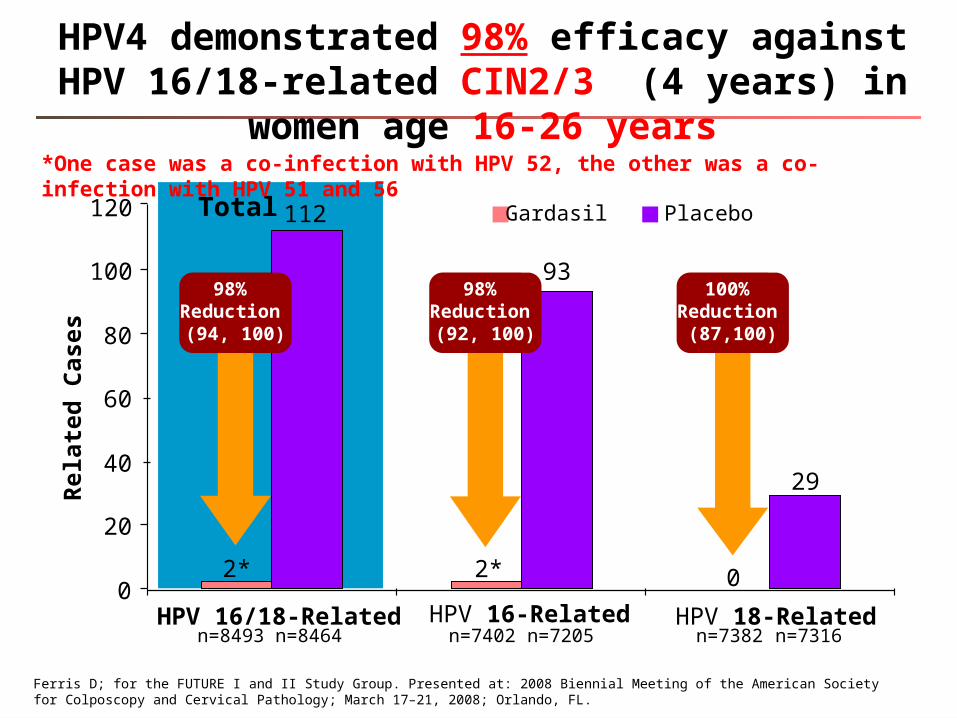
93
29
02* 2*
98% Reduction (92, 100)
100% Reduction
(87,100)
n=7402 n=7205 n=7382 n=7316n=8493 n=8464
0
20
40
60
80
100
HPV 16/18-Related HPV 16-Related HPV 18-Related
Gardasil Placebo120 112
Rel
ated
Cas
es
Total
Ferris D; for the FUTURE I and II Study Group. Presented at: 2008 Biennial Meeting of the American Society for Colposcopy and Cervical Pathology; March 17–21, 2008; Orlando, FL.
*One case was a co-infection with HPV 52, the other was a co-infection with HPV 51 and 56
HPV4 demonstrated 98% efficacy against HPV 16/18-related CIN2/3 (4 years) in women age 16-26 years
98% Reduction (94, 100)

Per-Protocol Efficacy Population
22 0 0
227
193
28 23
0
50
100
150
200
250
HPV 6/11/16/18-Related EGL
GenitalWarts
VIN 1,VaIN 1
VIN 2/3,VaIN 2/3
99% Reduction (96, 100)
100% Reduction
(86,100)
100% Reduction
(83,100)
Haupt RM. ACIP. February 27, 2008. Available at: http://www.cdc.gov/vaccines/recs/ACIP/downloads/mtg-slides-feb08/14-3-hpv.pdf. Accessed July 11, 2008.
n=9075 n=9075
Rel
ated
Cas
es
Gardasil PlaceboTotal
HPV4 demonstrated 99% efficacy against HPV6/11/16/18-related EGL (4 years) in women age 16-26 years
99% Reduction (97, 100)
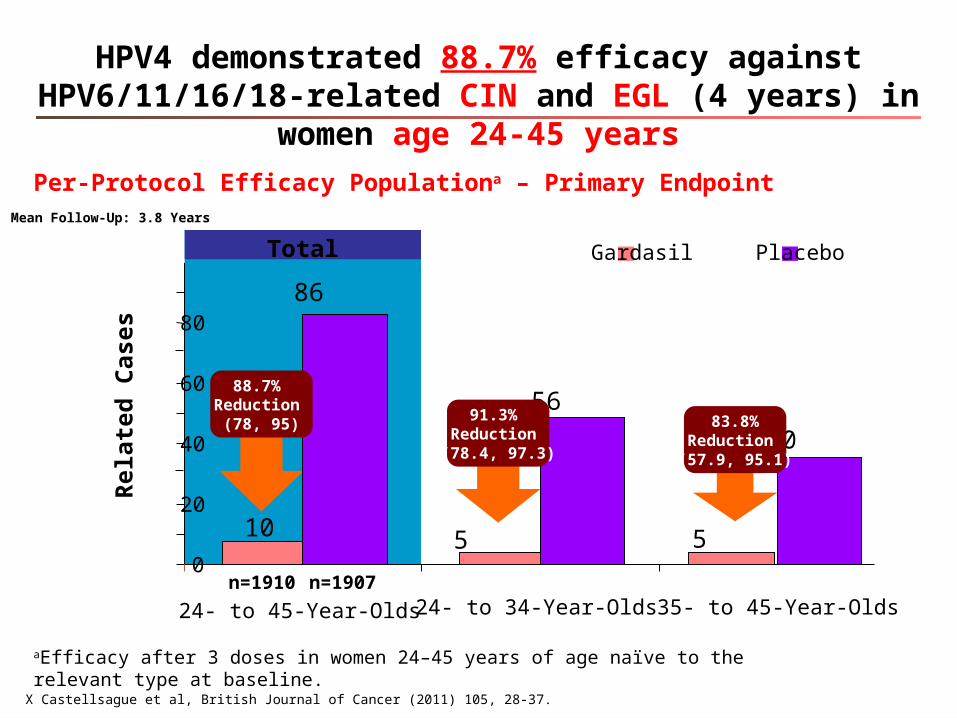
aEfficacy after 3 doses in women 24–45 years of age naïve to the relevant type at baseline.
Per-Protocol Efficacy Populationa – Primary Endpoint
5510
86
56
30
0
20
40
60
80
24- to 45-Year-Olds 24- to 34-Year-Olds 35- to 45-Year-Oldsn=1910 n=1907
88.7% Reduction
(78, 95)91.3%
Reduction (78.4, 97.3)
83.8%Reduction (57.9, 95.1)
Gardasil PlaceboTotal
X Castellsague et al, British Journal of Cancer (2011) 105, 28-37.
Mean Follow-Up: 3.8 Years
Rel
ated
Cas
es
HPV4 demonstrated 88.7% efficacy against HPV6/11/16/18-related CIN and EGL (4 years) in women age 24-45 years
Efficacy in men aged 16-26 years

HPV IN MALES
CancerHPV
prevalence (%)
HPV 16/18 among HPV positive (%)
Cervix 100% 70%
Vulva 40% 80%
Vagina 64-91% 80%
Anus 90% 75-90%
Penis 40% 60%
Susanne Krüger Kjær, Presented at Eurogin 2010, Monte-Carlo:France
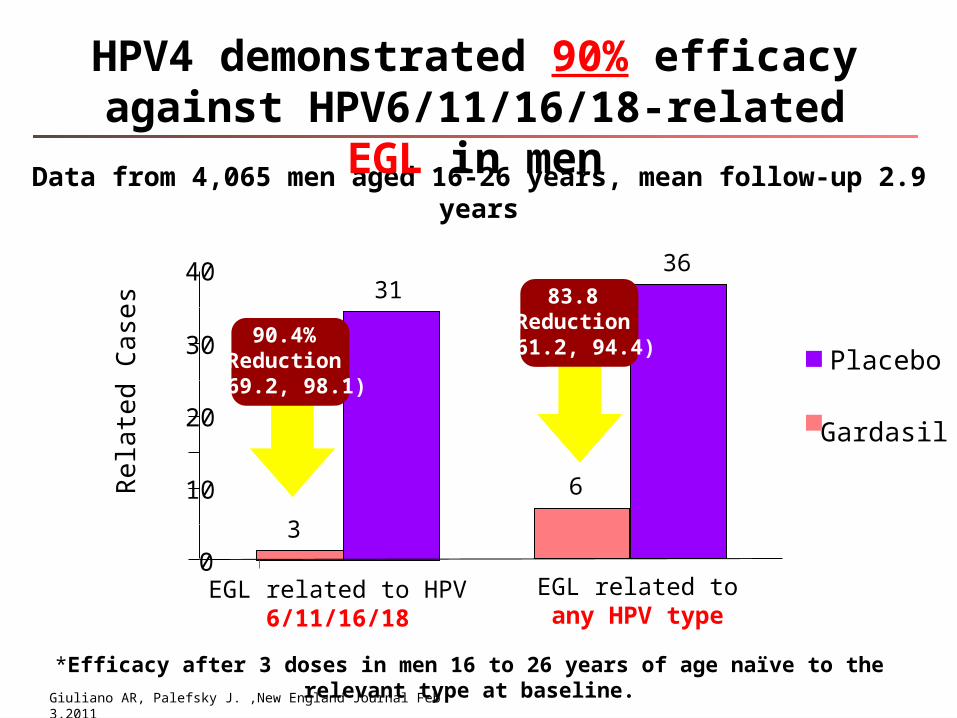
*Efficacy after 3 doses in men 16 to 26 years of age naïve to the relevant type at baseline.
Gardasil
Placebo
Rela
ted
Case
s
Data from 4,065 men aged 16-26 years, mean follow-up 2.9 years
3
31
0
10
20
30 90.4% Reduction (69.2, 98.1)
EGL related to HPV 6/11/16/18
HPV4 demonstrated 90% efficacy against HPV6/11/16/18-related EGL in men
40
6
3683.8
Reduction (61.2, 94.4)
EGL related to any HPV type
Giuliano AR, Palefsky J. ,New England Journal Feb 3,2011
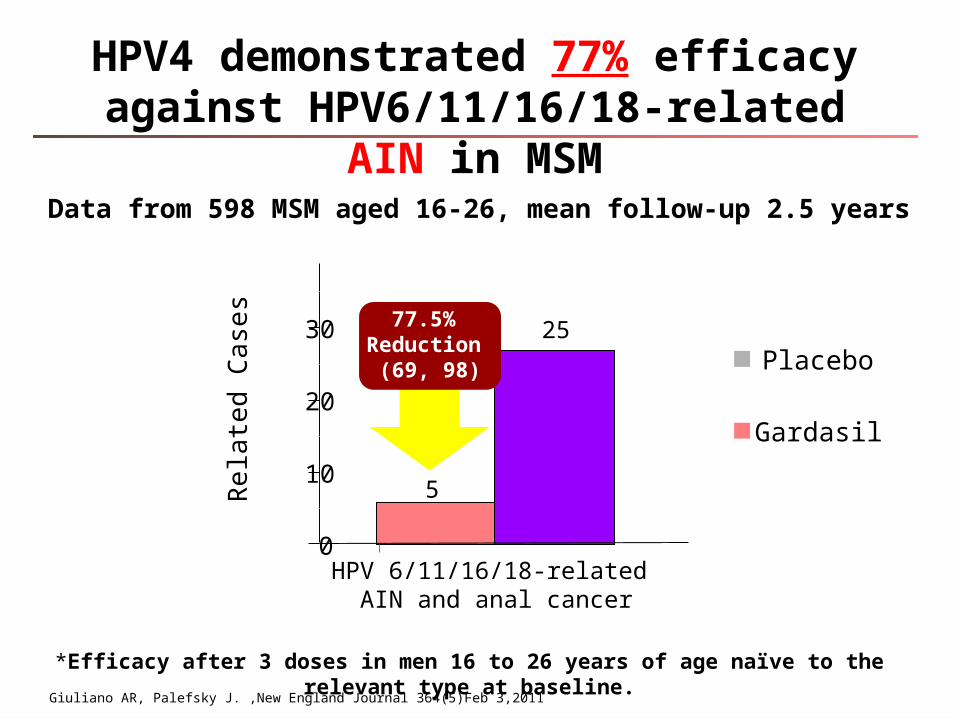
*Efficacy after 3 doses in men 16 to 26 years of age naïve to the relevant type at baseline.
Gardasil
Placebo
Rela
ted
Case
sData from 598 MSM aged 16-26, mean follow-up 2.5 years
5
25
0
10
20
30 77.5% Reduction
(69, 98)
HPV 6/11/16/18-related AIN and anal cancer
Giuliano AR, Palefsky J. ,New England Journal 364(5)Feb 3,2011
HPV4 demonstrated 77% efficacy against HPV6/11/16/18-related AIN in MSM
The rationale for HPV immunization in males
• Immunization in males provides direct benefit to males, including prevention of genital warts and anal cancer
• Immunization in males is expected to provide indirect benefit for females through herd immunity (reduced transmission of HPV)

Duration of Protection
19
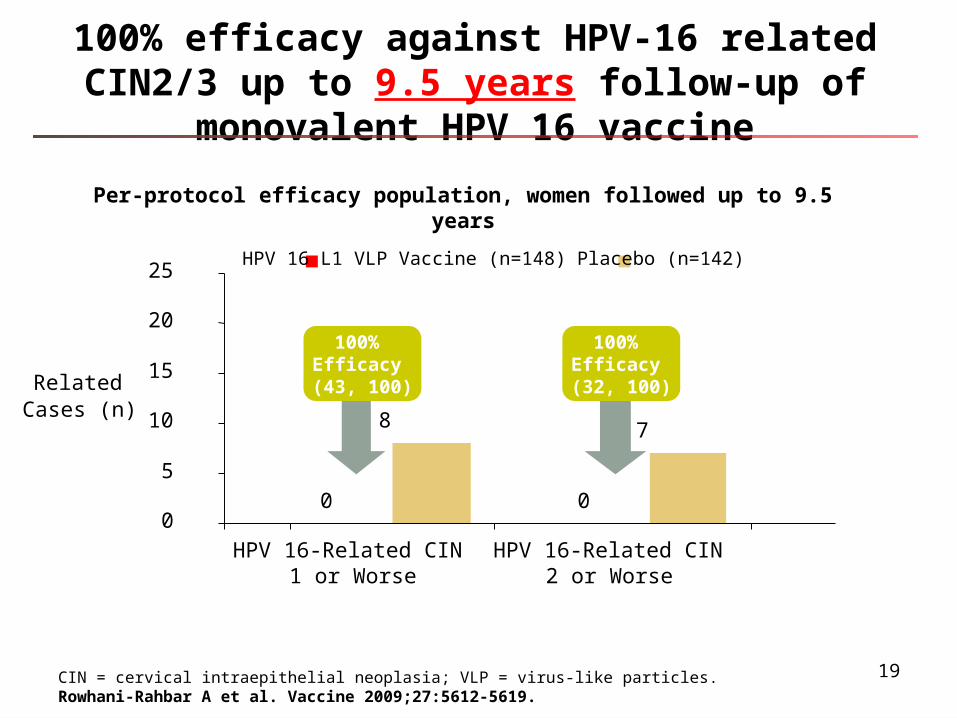
100% efficacy against HPV-16 related CIN2/3 up to 9.5 years follow-up of monovalent HPV 16 vaccine
CIN = cervical intraepithelial neoplasia; VLP = virus-like particles. Rowhani-Rahbar A et al. Vaccine 2009;27:5612-5619.
Per-protocol efficacy population, women followed up to 9.5 years
0 0
8 7
0
5
10
15
20
25
HPV 16-Related CIN1 or Worse
HPV 16-Related CIN2 or Worse
Related Cases (n)
HPV 16 L1 VLP Vaccine (n=148) Placebo (n=142)
100% Efficacy (32, 100)
100% Efficacy (43, 100)
20
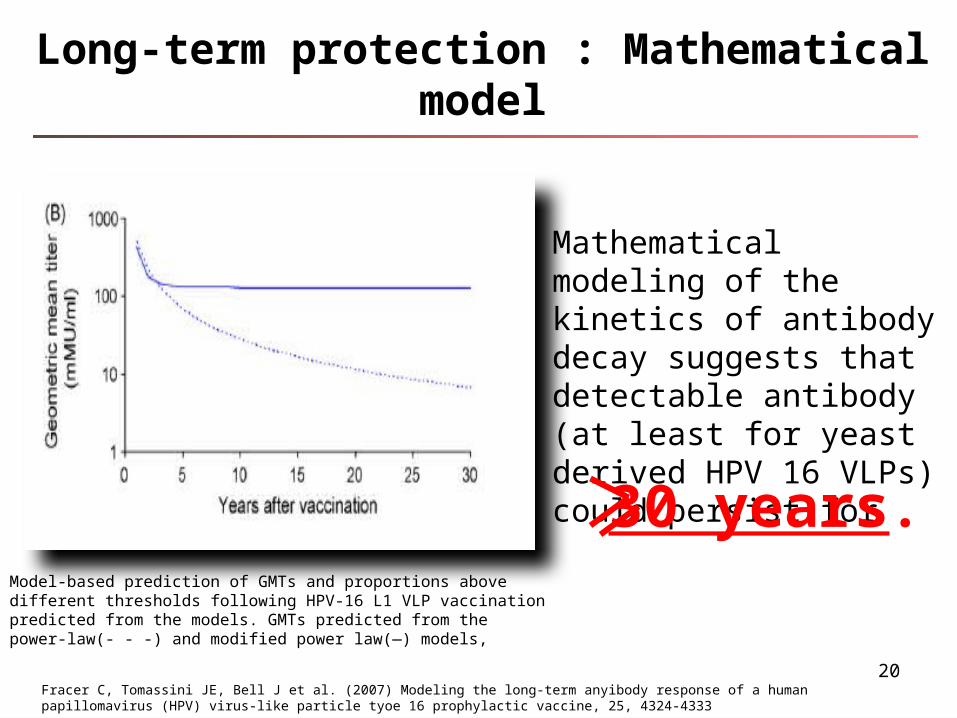
Long-term protection : Mathematical model
Mathematical modeling of the kinetics of antibody decay suggests that detectable antibody (at least for yeast derived HPV 16 VLPs) could persist for
Fracer C, Tomassini JE, Bell J et al. (2007) Modeling the long-term anyibody response of a human papillomavirus (HPV) virus-like particle tyoe 16 prophylactic vaccine, 25, 4324-4333
Model-based prediction of GMTs and proportions above different thresholds following HPV-16 L1 VLP vaccination predicted from the models. GMTs predicted from the power-law(- - -) and modified power law(—) models,
30 years.

Surveillance: e.g. In the Nordic countries• Long-term follow-up study: 14 years of follow-up• Evaluation of 5500 women aged 16–23years from FUTURE
II
Denmark Norway Iceland Sweden
IIKruger KjaerEUROGIN 2010, 19. Feb, 17h30-19h,SS5-2, Auditorium Prince Pierre
Evaluation of HPV4 Duration of Protection

HPV4 demonstrated 100% effectiveness against HPV 16/18-related CIN 2 or worse (8 years)
0 0 00
20
40
60
80
100
Zero number
of cases
Vaccine
Effectiveness
Vaccine
Effectiveness
Vaccine
Effectiveness
(N=1,080) (N=921) (N=1.032)
HPV 16/18-Related CIN 2 or Worse
HPV 16-Related CIN 2 or Worse
HPV 18-Related CIN 2 or Worse
Zero number
of cases
Zero number
of cases
*Vaccine effectiveness measures the relative reduction of the disease incidence in vaccine recipients compared to the baseline incidence rate of 0.0287 per 100 person-years established from the incidence rate in an unvaccinated cohort and under the assumption vaccine efficacy is 90%.
Per Protocol Efficacy Population (N=1724)Longest follow up: 8 years
VE:100 % VE:100 % VE:100 %
Vacc
ine
Effec
tiven
ess*
(VE)
Pe
rcen
tage
No Breakthrough cases of Disease through 8 years

Cross Protection

WHO Position Paper: Cross Protection
• BOTH vaccines appear to have partial efficacy against
infections caused by HPV 31 and 45, which are
phylogenetically related to HPV 16 and 18
• Differences among the efficacy trials of the quadrivalent
and bivalent vaccines in terms of choice of placebo
recipients or control subjects, immunological assays and
populations analysed PRECLUDE DIRECT
COMPARISON of results for the 2 vaccines
WHO position paper : Human Papillomavirus Vaccine 10 April 2009

Gender Neutral Vaccination

HPV4 is the onlyHPV vaccine approved
for males

• Optimal vaccine efficacy is derived if the vaccine is administered before onset of sexual activity
• Antibody responses are highest at age 9-15 years.
The rationale for routine HPV immunization at 11-12 years of is twofold
0
10
20
30
40
50
60
70
80
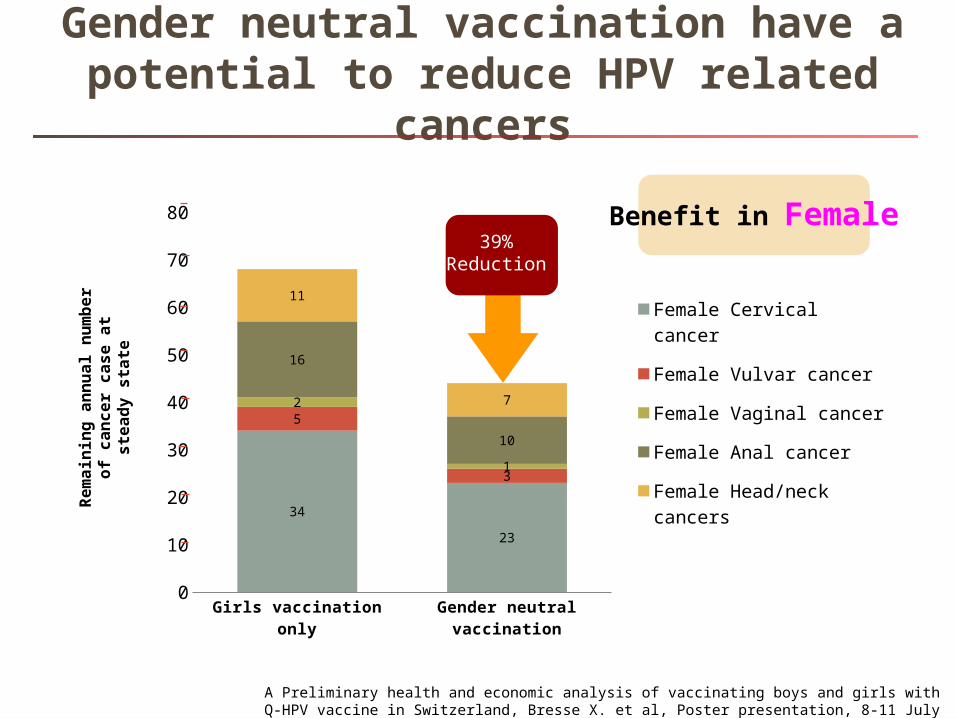
34
23
5
3
2
1
16
10
11
7
Female Cervical cancer
Female Vulvar cancer
Female Vaginal cancer
Female Anal cancer
Female Head/neck cancers
39% Reduction
Rem
ain
ing
ann
ual
nu
mb
er o
f ca
nce
r ca
se a
t st
ead
y st
ate
Benefit in Female
A Preliminary health and economic analysis of vaccinating boys and girls with Q-HPV vaccine in Switzerland, Bresse X. et al, Poster presentation, 8-11 July 2012, EUROGIN 2012, Czech Republic
Gender neutral vaccination have a potential to reduce HPV related cancers
Girls vaccination only
Gender neutral vaccination
0
10
20
30
40
50
60
70
80
90
100
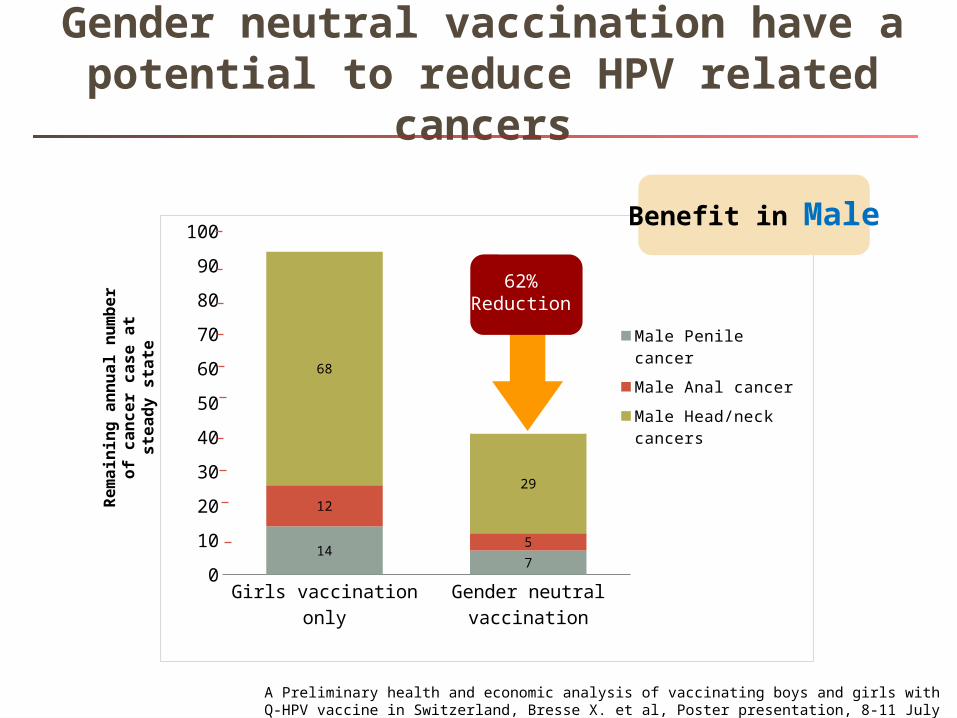
147
12
5
68
29
Male Penile cancer
Male Anal cancer
Male Head/neck cancers
Rem
ain
ing
ann
ual
nu
mb
er o
f ca
nce
r ca
se a
t st
ead
y st
ate
62% Reduction
Benefit in Male
A Preliminary health and economic analysis of vaccinating boys and girls with Q-HPV vaccine in Switzerland, Bresse X. et al, Poster presentation, 8-11 July 2012, EUROGIN 2012, Czech Republic
Gender neutral vaccination have a potential to reduce HPV related cancers

1. http://www.health.gov.au/internet/ministers/publishing.nsf/Content/59C397F61CACF02FCA257A390000C65A/$File/TP059.pdf2 www.thelancet.com/infection Published online November 9, 2010 DOI:10.1016/S1473-3099(10)70225-5, Quadrivalent human papillomavirus vaccination and trendsin genital warts in Australia: analysis of national sentinel surveillance data, . Basil Donovan
• On 12 July 2012, the Minister for Health, Australian Government announced funding for the Quadrivalent HPV Vaccine for 12 and 13 year old boys through school-based programs under the National Immunisation Program, start next school year- 2013. 1
• Year 9 boys will also be able to get the vaccine at school under a catch-up Program for the next two years. 1
• In April, 2007, the Australian Government initiated aprogramme to vaccinate all girls from the age of 12 years with the Quadrivalent HPV Vaccine existing school vaccination system and catch-up to all female Australian residents in thecommunity up to the age of 26 years 2
Update news – In a world first !
Today we can protect & against MOREHPV- related diseases as Gender Neutral Vaccination
Quadrivalent HPV vaccine
Real world experiences
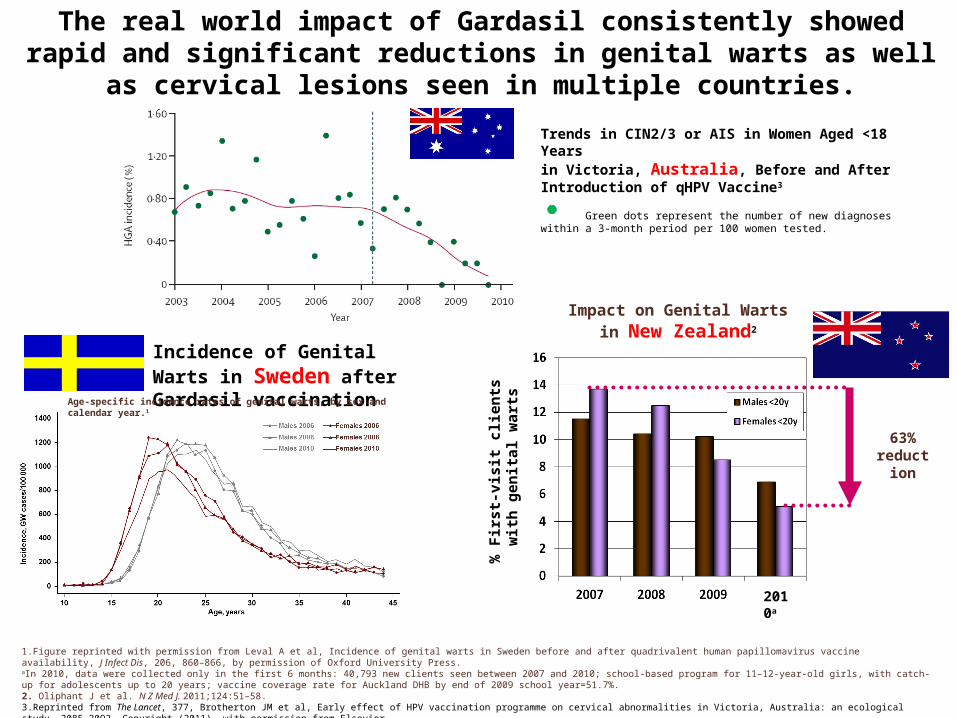
The real world impact of Gardasil consistently showed rapid and significant reductions in genital warts as well as cervical lesions seen in multiple countries.
63% reduction
% F
irst-
visi
t clie
nts
with
gen
ital w
arts
2010a
Incidence of Genital Warts in Sweden after Gardasil vaccination
Age-specific incidence rates of genital warts, by sex and calendar year.1
Impact on Genital Warts
in New Zealand2
1.Figure reprinted with permission from Leval A et al, Incidence of genital warts in Sweden before and after quadrivalent human papillomavirus vaccine availability, J Infect Dis, 206, 860–866, by permission of Oxford University Press. aIn 2010, data were collected only in the first 6 months: 40,793 new clients seen between 2007 and 2010; school-based program for 11–12-year-old girls, with catch-up for adolescents up to 20 years; vaccine coverage rate for Auckland DHB by end of 2009 school year=51.7%. 2. Oliphant J et al. N Z Med J. 2011;124:51–58.3.Reprinted from The Lancet, 377, Brotherton JM et al, Early effect of HPV vaccination programme on cervical abnormalities in Victoria, Australia: an ecological study, 2085–2092, Copyright (2011), with permission from Elsevier.
Trends in CIN2/3 or AIS in Women Aged <18 Years in Victoria, Australia, Before and After Introduction of qHPV Vaccine3
Green dots represent the number of new diagnoses within a 3-month period per 100 women tested.

Quadrivalent HPV vaccine
Worldwide recommendation
34
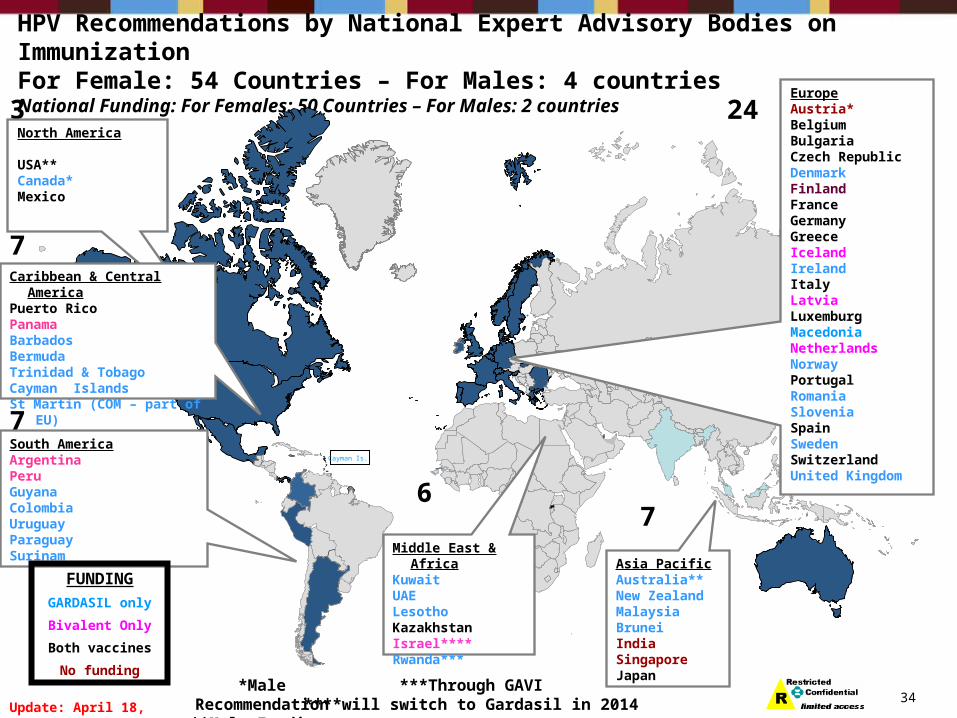
HPV Recommendations by National Expert Advisory Bodies on ImmunizationFor Female: 54 Countries – For Males: 4 countriesNational Funding: For Females: 50 Countries – For Males: 2 countries
Update: April 18, 2013
Cayman Is.
3North America
USA**Canada* Mexico
7South AmericaArgentina PeruGuyanaColombiaUruguayParaguaySurinam
6
Middle East & AfricaKuwaitUAELesothoKazakhstanIsrael****Rwanda***
7
Asia PacificAustralia**New ZealandMalaysiaBruneiIndiaSingaporeJapan
24EuropeAustria*BelgiumBulgariaCzech RepublicDenmarkFinlandFranceGermanyGreeceIcelandIrelandItalyLatviaLuxemburgMacedoniaNetherlandsNorwayPortugalRomaniaSloveniaSpainSwedenSwitzerlandUnited Kingdom
Caribbean & Central AmericaPuerto Rico PanamaBarbadosBermuda Trinidad & Tobago Cayman IslandsSt Martin (COM – part of EU)
7
FUNDING
GARDASIL only
Bivalent Only
Both vaccines
No funding*Male Recommendation
**Male Funding ***Through GAVI
****will switch to Gardasil in 2014

The Department of Healthhas decided to change the vaccine it uses to protect girls against cervical cancer throughout the UK
http://www.bbc.co.uk/news/health-15879222
UK switched to HPV4 in Sep 2012

Bhutan • Free HPV immunization for 12 – 18 year old girls and
young women starting since 2010-2014 (QHPV)
Malaysia • Free HPV immunization to 13 years old girls starting
2010-2011 (BHPV) and switch to QHPV in 2012
Thailand• On process
ASIAN Focus: National HPV Vaccination program

• HPV infection is common, leading to many diseases, such as cervical, vulvar, vaginal, anal cancers, and genital warts
• Disease prevention (CIN2/3, AIS) is still the only accepted way to measure efficacy of HPV vaccines
• HPV4 is the only HPV vaccine that has demonstrated high efficacy in a variety of populations (males & females)
• Cross protection with HPV vaccines may exist but magnitude and duration of protection is still unknown
Take home messages
• ‘Gender Neutral Vaccination’ will help reduce more disease burden related to HPV infection (only HPV4 is approved in males )
• Recent data have shown that HPV4 is more cost effective than bivalent vaccine
• Many countries have chosen to include HPV4 into their national immunization program
Take home messages

Thank you
Top Related