







Languages
Pages
Legal


International Journal of Dermatology
2007,
46
, 976–981 © 2007
The International Society of Dermatology
976
Abstract
Although unwanted facial hair often leads to anxiety and avoidance of social situations,
evaluation of treatment outcomes in clinical trials has relied largely on measures external to the
patient such as the extent of hair growth or an expert physician’s assessment, neglecting to
include patient reported outcomes (PRO). To assess the level of bother caused by a
dermatological condition (hirsutism) and changes brought on by treatment, the instrument
ESTEEM was developed by expanding the Bother Assessment in Skin Conditions (BASC)
scale to six questions to cover the discomfort felt in four social situations and bother due to
removing facial hair. Each question elicits responses on a visual analog scale. Women
participating in two randomized clinical trials evaluated a new treatment (eflornithine 13.9%
cream). Analyses examined the level of bother at each visit, the changes with treatment, the
correlations with the Physician’s Global Assessment, and the effect size. Hirsutism bothers
patients considerably. The mean for overall bother was 89% and the mean discomfort in social
situations exceeded 80% in nearly all cases. Treatment led to significant reductions in bother
on all six items with effect sizes ranging from 0.46 to 1.62. Eflornithine is an effective treatment
for unwanted facial hair in women, as reported by the patients. ESTEEM addresses the specific
concerns of women with hirsutism.
Blackwell Publishing, Ltd.Oxford, UKIJDInternational Journal of Dermatology0011-9059© 2007 The International Society of Dermatology46
Clinical trial
Effect of eflornithine on bother due to hirsutism
Jackson
et al.
Clinical trial
The effect of eflornithine 13.9% cream on the bother and discomfort due to hirsutism
*
Joseph Jackson,
PhD
, J. Jaime Caro,
MDCM, FRCPC, FACP
, Graciela Caro,
MSc
, Frances Garfield,
PhD
, Ferdinand Huber,
BS
, Wenjiong Zhou,
PhD
, Chen-Sheng Lin,
PhD
, Douglas Shander,
PhD
, Kathy Schrode,
PhD
, and the Eflornithine HCl Study Group
From the Bristol Myers-Squibb Pharmaceutical Research Institute, Princeton, New Jersey, Caro Research Institute, Concord, Massachusetts, Division of General Internal Medicine, McGill University, Montreal, Canada, Gillette Advanced Technology Center, Needham, Massachusetts
Correspondence
J. Jaime Caro,
MDCM
,
FRCPC
,
FACP
336 Baker AvenueConcord, MA 01742E-mail: [email protected]
*Presented in part as posters at the 58th Annual Meeting of the American Academy of Dermatology, 10–15 March 2000, San Francisco, CA.
Introduction
Unwanted facial hair often leads to the avoidance of socialsituations and to symptoms of anxiety and depression.
1–4
Despite the intensely personal nature of the impact of thiscondition, evaluation of treatment outcomes in clinical trialshas relied largely on measures external to the patient, suchas the extent of hair growth or an expert physician’s assess-ment.
5,6
These assessments may not adequately addressaspects that are important to the patient, particularly whenthe condition’s main impact is psychosocial rather thanphysical, and the outcome depends entirely on the patient’sperceptions, not those of an observer.
7,8
Therefore, it isimportant to establish the effect of treatment as reported bythe patient.
Eflornithine HCl 13.9% cream is a topical treatment thatreduces the rate of hair growth. In two double-blind, vehicle-controlled studies, it has been shown to diminish significantlyunwanted facial hair and was to be tolerated.
9
This paper describes the results of patient-reported out-comes (PROs) measured in these two studies, using ESTEEM
(
E
xchanges of affection,
S
ocial interactions,
T
ime spentremoving facial hair,
E
ncountering new people,
E
ngaging inwork or school,
M
inimizing overall bother with facial hair),an instrument that addresses the bother and discomfort feltby women with unwanted facial hair.
Methods
Study design
Two multicenter, double-blind, randomized, vehicle-controlled,
parallel-group studies were conducted at 18 centers (17 in the
USA and one in Spain). Ethical committee approval and patient
informed consent were obtained. The main inclusion criteria were
as follows: women of at least 16 years of age with a clinical
diagnosis of facial hirsutism; an average hair density of at least
five hairs per square centimeter on both the chin and upper lip
as assessed by video image analysis; customary frequency of
hair removal of at least twice per week; good general health;
a negative serum or urine pregnancy test for women of
child-bearing age; and a score of at least 20 on a visual analog
scale (VAS) ranging from 0 (not bothered) to 100 (extremely

© 2007
The International Society of Dermatology International Journal of Dermatology
2007,
46
, 976–981
977
Jackson
et al. Effect of eflornithine on bother due to hirsutism
Clinical trial
bothered) for the question: “How much are you bothered by your
facial hair?”.
Subjects were randomized to receive either active treatment or
vehicle, in a 2 : 1 ratio, twice daily for 24 weeks, on the affected
areas of the face and adjacent areas of the neck. An 8-week no-
treatment period followed. During the entire 32 weeks, subjects
were permitted to continue their normal hair removal method;
however, shaving and cutting were not permitted within 24 h of
the first day of a scheduled study visit, plucking within 48 h, or
bleaching within 1 week of the first day of a scheduled visit.
Each scheduled visit (see below) comprised two observations
separated by 48 h. Subjects shaved on the first of these two
observation days and no hair removal was permitted prior to
the second observation when PRO, the Physician’s Global
Assessment (PGA), and video analysis were conducted.
The primary efficacy endpoint was PGA (observable changes in
facial hair vs. baseline using the scale: Grade 0, no improvement/
worse; Grade 1, improved; Grade 2, marked improvement;
Grade 3, clear/almost clear). The last two grades were classified
as “success.” Photograph-aided assessments were performed at
weeks 2, 4, 8, 16, and 24 during treatment and at 8 weeks after
treatment. Subjects were not allowed to wear make-up during
evaluations.
PRO was conducted at baseline, at weeks 8, 16, and 24 during
the treatment period, and at 8 weeks after the end of treatment.
A baseline photograph of each subject was provided to remind
them of the severity of their condition. PGA was not revealed to the
subject.
Instrument for PRO
The PRO measure, ESTEEM, is a modification of the Bother
Assessment in Skin Conditions (BASC) instrument, which was
developed and used in a study on the impact of hyperpigmentation.
10
PRO incorporates the BASC concepts of bother and discomfort,
which ask subjects to report the degree to which the skin condition
bothers them on a 100-mm VAS, with one end indicating “not
bothered” and the other indicating “extremely bothered” or
“extremely uncomfortable.” The distance (mm) between the
subject’s mark and the left (“not bothered” or “not uncomfortable”)
end of the scale was read as the percentage of extreme bother
experienced by the subject. To complement the bother scale for
this condition, several questions were added to the instrument
to ascertain under what social settings the condition was
bothersome, and how much the subjects were bothered by their
time masking the condition from the public. This approach parallels
that used previously,
11
where a series of questions concerning
pain intensity were combined with questions concerning pain
interference with normal activities. The following items were
included in the ESTEEM instrument:
•
How much are you bothered by your facial hair?
•
How uncomfortable does your facial hair make you feel:
•
When you meet new people?
•
When you go to work or class?
•
When you go to social gatherings, dine out in a public restaurant, go to the supermarket or other public place?
•
In exchanges of affection (such as in an intimate situation withyour partner)?
•
How much are you bothered by the time you spend removinghair?
Analyses
Analyses of the data from each study were conducted according
to the protocol; the primary time point was at the end of treatment
(week 24) on an intention-to-treat basis, and an assessment of
active treatment vs. vehicle was performed. Patients with baseline
responses and at least one observation after baseline had their
last observation carried forward; only subjects with answers to all
six questions were included. For each study, the null hypothesis
that eflornithine and its vehicle had equal effects on all PROs was
tested first (
P
≤
0.05) using a multivariate analysis of variance
(SAS – PROC GLM,
MANOVA
option), including treatment and
investigational site, as it was anticipated that the responses to the
six questions in ESTEEM would be correlated. Baseline values
were included in the model for questions with imbalanced baseline
values between active treatment and vehicle groups. The
interaction term between the treatment and investigational site
was not significant and thus was dropped from the model. If the
overall null hypothesis was rejected (Wilk’s criterion), each
question was then evaluated on its own. The individual question
evaluations were considered as exploratory; no multiplicity
adjustments were planned. Given, however, that the individual
question would be evaluated only if the overall hypothesis
that eflornithine and its vehicle had equal effects on all PROs
was rejected, and given that the
P
values on some of the
individual questions were extremely small (< 0.005), statistical
significance may still be claimed for those questions by Bonferroni
adjustment.
The analyses of covariance (
ANCOVA
) on the changes from
baseline for each question, the cumulative distribution of changes
from baseline, the effect size, and the concordance between PRO
responses and PGA and hair length were conducted outside the
protocol-defined analyses to help assess the observed differences
on the ESTEEM measures.
ANCOVA
was performed using
treatment, investigational site, and its baseline as factors in the
model. The data from each study were analyzed, as well as the
pooled results. The “effect size” was defined as the mean change
from baseline for eflornithine HCl 13.9% cream minus the mean
change from baseline for vehicle divided by the standard deviation
at baseline. Concordance was analyzed by re-categorizing PRO
responses into five categories (0–20, 20–40, 40–60, 60–80, 80–
100), followed by Kendall’s tau-b method.
12
Results
Of the 594 treated subjects (age range, 18–83 years), 508(90% and 87% of subjects treated with eflornithine HCl andvehicle, respectively) were included in this assessment.

International Journal of Dermatology
2007,
46
, 976–981 © 2007
The International Society of Dermatology
978 Clinical trial
Effect of eflornithine on bother due to hirsutism
Jackson
et al.
Subjects tended to be somewhat overweight (71–96 kg), acharacteristic of women who suffer with facial hirsutism;63% were white. Nearly half (49.5%) of the women onlyshaved their facial hair, 20.7% only plucked, 29.5% didboth, and 0.4% used other methods of hair removal duringthe 2 weeks prior to the study. There were no significant dif-ferences between the study groups.
Subjects reported that unwanted facial hair bothered themconsiderably. The distributions of values at baseline wereheavily skewed towards the extreme end for all questions,with mean values ranging from 79 to 89% (overall bother). Inone of the two studies, the mean value at baseline was higherin subjects randomized to vehicle for the items: “Discomfortat work or class” (88% vs. 82%,
P
= 0.006) and “Discomfortat social gatherings” (88% vs. 83%,
P
= 0.035). None of theother differences were statistically significant in either trial.All group differences were taken into account in subsequentanalyses.
Subjects receiving active treatment reported less bother anddiscomfort at 24 weeks than those receiving vehicle (multi-variate analysis,
P
= 0.0297 and
P
= 0.0027 in Studies 1 and2, respectively). Each PRO was also examined individually;all differences were highly statistically significant in each trial(
P <
0.02), and were pooled (Table 1).
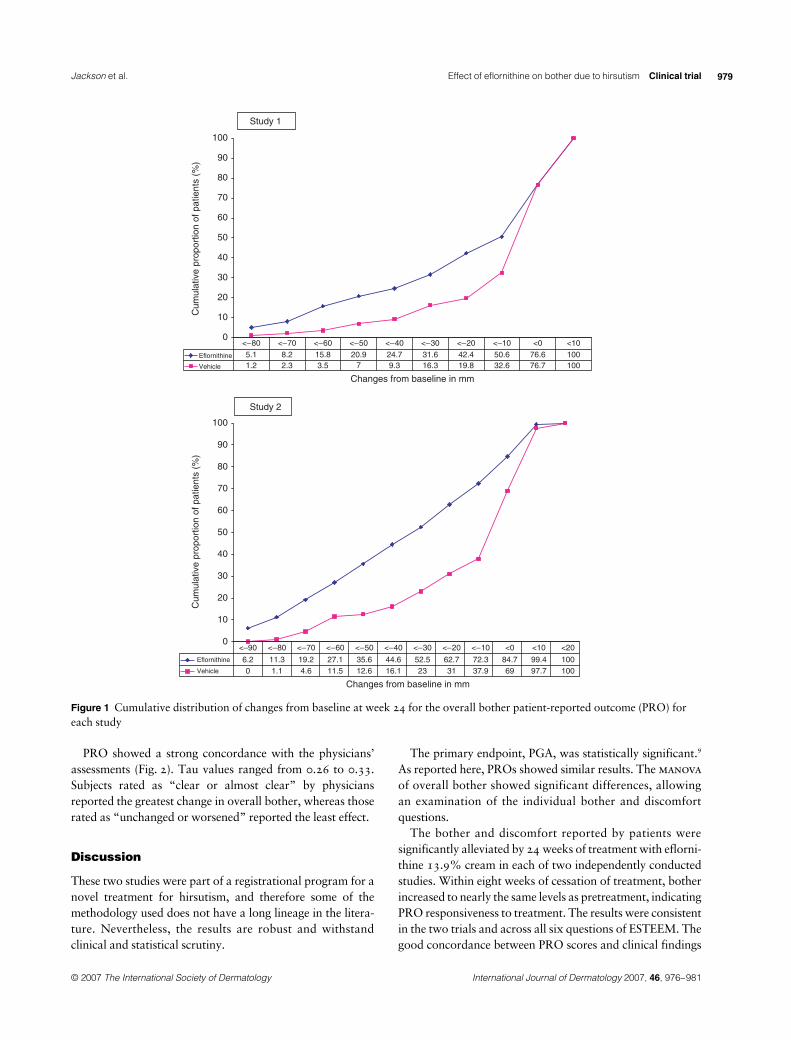
Figure 1 presents the cumulative distribution of the differ-ence from baseline in Question 1, at 10-mm intervals, for eachstudy. At each improvement score, there were consistentlymore subjects in the eflornithine HCl cream group than in thevehicle group reporting at least that level of improvement. Allof the other questions in both studies showed similar responsepatterns for each treatment group. At week 24, nearly two-thirds (50.6% and 72.6%, respectively, for each study) ofsubjects receiving eflornithine had achieved a decrease inoverall bother of at least 10 points, compared with only one-third (32.6% and 37.9%, respectively) of subjects on vehicle.More than half (42.4% and 62.7%, respectively) achieved animprovement of at least 20 points on active treatment, com-pared with only one-quarter (19.8% and 21.0%, respec-tively) of vehicle subjects. Regardless of the cut-off used, allcomparisons were statistically significant (
P <
0.001).The changes for each question from baseline to the end of
treatment were compared across treatments (Table 1). Thedecreases in bother and discomfort were more than twofoldgreater vs. baseline with eflornithine than with vehicle.
The effect size for each PRO ranged from 0.46 to 1.62(Table 2). Eight weeks after the end of treatment, the meanlevels of bother and discomfort had increased again, reachingnearly equal values to those reported by participants on vehicle.
Table 1 Patient-reported levels of bother and discomfort, pooling the two studies
PRO and treatment group n
Baseline mean (SD)
24-week mean (SD)
Decrease from baseline* mean (SE)
Adjusted decrease from baseline mean (SE)
Estimated difference† (P)
95% CI limits Relative change‡Upper Lower
Bothered by facial hairEflornithine 335 89.0 (13.0) 58.3 (31.4) 30.7 (1.7) 29.6 (1.5) 15.8 10.8 20.8 2.1Vehicle 173 89.2 (12.6) 74.8 (26.3) 14.4 (1.6) 13.8 (2.1) (< 0.01)
Discomfort when meeting new peopleEflornithine 335 84.7 (19.6) 57.2 (32.8) 27.5 (1.7) 26.6 (1.5) 15.7 10.8 20.5 2.4Vehicle 173 86.0 (18.9) 74.3 (27.4) 11.7 (1.5) 11.0 (2.1) (< 0.01)
Discomfort at work or classEflornithine 335 83.4 (19.8) 54.9 (32.8) 28.5 (1.7) 27.9 (1.5) −15.5 10.5 20.4 2.3Vehicle 173 86.4 (16.2) 73.0 (26.4) 13.4 (1.6) 12.4 (2.1) (< 0.01)
Discomfort at social gatheringsEflornithine 335 83.8 (19.7) 55.6 (32.8) 28.2 (1.7) 27.3 (1.5) 14.9Vehicle 173 86.3 (16.2) 72.7 (27.2) 13.5 (1.7) 12.4 (2.1) (< 0.01) 9.9 19.9 2.2
Discomfort in exchanges of affectionEflornithine 335 82.1 (23.6) 55.7 (34.4) 26.4 (1.7) 25.4 (1.5) 14.7Vehicle 173 83.4 (22.9) 71.9 (30.0) 11.6 (1.6) 10.7 (2.1) (< 0.01) 9.8 19.6 2.4
Bothered by time spent removing hairEflornithine 335 81.8 (23.2) 53.1 (33.4) 28.6 (1.7) 27.5 (1.6) 16.6Vehicle 173 80.3 (24.4) 68.7 (30.1) 11.6 (1.9) 11.3 (2.2) (< 0.01) 11.1 21.3 2.4
CI, confidence interval; SD, standard deviation; SE, standard error; PRO, patient-reported outcome.*Decrease from baseline = baseline value − on-therapy value.†Estimated difference = adjusted mean change for active group − adjusted mean change for vehicle group; for treatment effect from the analysis of covariance model: change = baseline site treatment.‡Relative change = eflornithine change/vehicle change.
© 2007
The International Society of Dermatology International Journal of Dermatology
2007,
46
, 976–981
979
Jackson
et al. Effect of eflornithine on bother due to hirsutism
Clinical trial
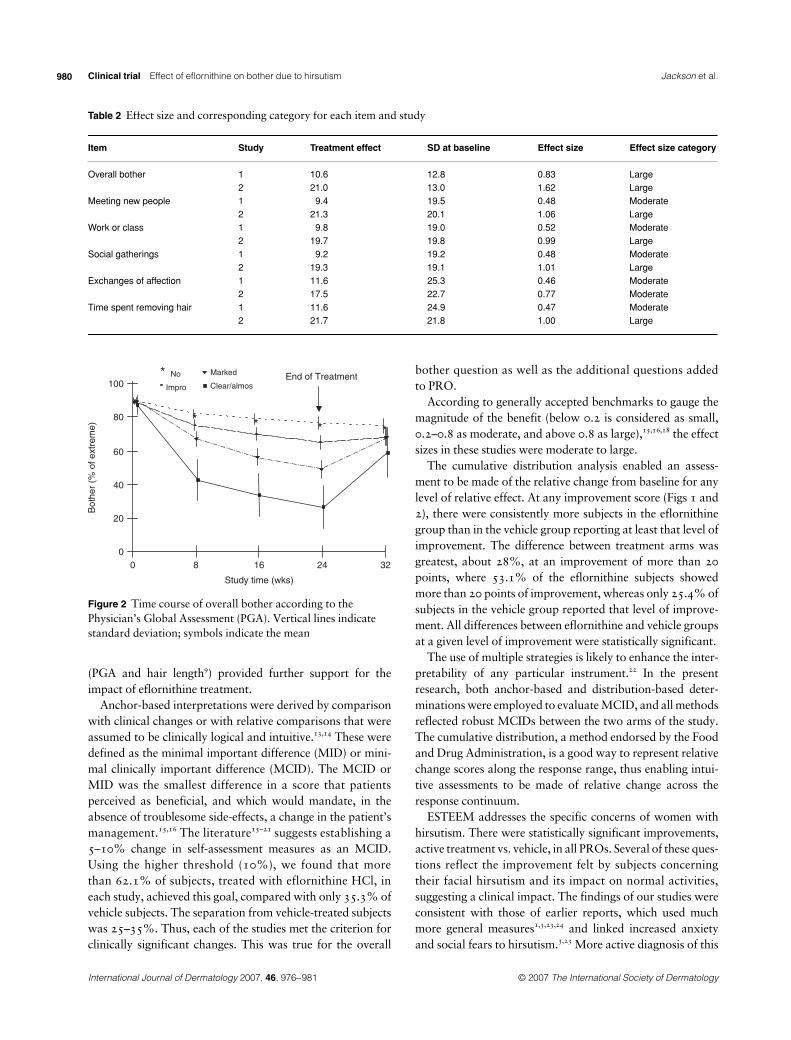
PRO showed a strong concordance with the physicians’assessments (Fig. 2). Tau values ranged from 0.26 to 0.33.Subjects rated as “clear or almost clear” by physiciansreported the greatest change in overall bother, whereas thoserated as “unchanged or worsened” reported the least effect.
Discussion
These two studies were part of a registrational program for anovel treatment for hirsutism, and therefore some of themethodology used does not have a long lineage in the litera-ture. Nevertheless, the results are robust and withstandclinical and statistical scrutiny.
The primary endpoint, PGA, was statistically significant.
9
As reported here, PROs showed similar results. The
manova
of overall bother showed significant differences, allowingan examination of the individual bother and discomfortquestions.
The bother and discomfort reported by patients weresignificantly alleviated by 24 weeks of treatment with eflorni-thine 13.9% cream in each of two independently conductedstudies. Within eight weeks of cessation of treatment, botherincreased to nearly the same levels as pretreatment, indicatingPRO responsiveness to treatment. The results were consistentin the two trials and across all six questions of ESTEEM. Thegood concordance between PRO scores and clinical findings
Figure 1 Cumulative distribution of changes from baseline at week 24 for the overall bother patient-reported outcome (PRO) for each study
International Journal of Dermatology
2007,
46
, 976–981 © 2007
The International Society of Dermatology
980 Clinical trial
Effect of eflornithine on bother due to hirsutism
Jackson
et al.
(PGA and hair length
9
) provided further support for theimpact of eflornithine treatment.
Anchor-based interpretations were derived by comparisonwith clinical changes or with relative comparisons that wereassumed to be clinically logical and intuitive.
13,14
These weredefined as the minimal important difference (MID) or mini-mal clinically important difference (MCID). The MCID orMID was the smallest difference in a score that patientsperceived as beneficial, and which would mandate, in theabsence of troublesome side-effects, a change in the patient’smanagement.
15,16
The literature
15–21
suggests establishing a5–10% change in self-assessment measures as an MCID.Using the higher threshold (10%), we found that morethan 62.1% of subjects, treated with eflornithine HCl, ineach study, achieved this goal, compared with only 35.3% ofvehicle subjects. The separation from vehicle-treated subjectswas 25–35%. Thus, each of the studies met the criterion forclinically significant changes. This was true for the overall
bother question as well as the additional questions addedto PRO.
According to generally accepted benchmarks to gauge themagnitude of the benefit (below 0.2 is considered as small,0.2–0.8 as moderate, and above 0.8 as large),
15,16,18
the effectsizes in these studies were moderate to large.
The cumulative distribution analysis enabled an assess-ment to be made of the relative change from baseline for anylevel of relative effect. At any improvement score (Figs 1 and2), there were consistently more subjects in the eflornithinegroup than in the vehicle group reporting at least that level ofimprovement. The difference between treatment arms wasgreatest, about 28%, at an improvement of more than 20points, where 53.1% of the eflornithine subjects showedmore than 20 points of improvement, whereas only 25.4% ofsubjects in the vehicle group reported that level of improve-ment. All differences between eflornithine and vehicle groupsat a given level of improvement were statistically significant.
The use of multiple strategies is likely to enhance the inter-pretability of any particular instrument.
22
In the presentresearch, both anchor-based and distribution-based deter-minations were employed to evaluate MCID, and all methodsreflected robust MCIDs between the two arms of the study.The cumulative distribution, a method endorsed by the Foodand Drug Administration, is a good way to represent relativechange scores along the response range, thus enabling intui-tive assessments to be made of relative change across theresponse continuum.
ESTEEM addresses the specific concerns of women withhirsutism. There were statistically significant improvements,active treatment vs. vehicle, in all PROs. Several of these ques-tions reflect the improvement felt by subjects concerningtheir facial hirsutism and its impact on normal activities,suggesting a clinical impact. The findings of our studies wereconsistent with those of earlier reports, which used muchmore general measures
1,3,23,24
and linked increased anxietyand social fears to hirsutism.
3,23
More active diagnosis of this
Table 2 Effect size and corresponding category for each item and study
Item Study Treatment effect SD at baseline Effect size Effect size category
Overall bother 1 10.6 12.8 0.83 Large2 21.0 13.0 1.62 Large
Meeting new people 1 9.4 19.5 0.48 Moderate2 21.3 20.1 1.06 Large
Work or class 1 9.8 19.0 0.52 Moderate2 19.7 19.8 0.99 Large
Social gatherings 1 9.2 19.2 0.48 Moderate2 19.3 19.1 1.01 Large
Exchanges of affection 1 11.6 25.3 0.46 Moderate2 17.5 22.7 0.77 Moderate
Time spent removing hair 1 11.6 24.9 0.47 Moderate2 21.7 21.8 1.00 Large
Figure 2 Time course of overall bother according to the Physician’s Global Assessment (PGA). Vertical lines indicate standard deviation; symbols indicate the mean

© 2007
The International Society of Dermatology International Journal of Dermatology
2007,
46
, 976–981
981
Jackson
et al. Effect of eflornithine on bother due to hirsutism
Clinical trial
condition by general physicians is now warranted to reduceits unnecessary burden.
Eflornithine HCl 13.9% cream is marketed under the tradename Vaniqa® Cream.
Eflornithine Study Group
Wilma F. Bergfeld,
md
; Francisco Camacho,
md
; AdrianS. Dobs,
md
; Frank Dunlap,
md
; Maria Hordinsky,
md
; H.Irving Katz,
md
; Mark Lebwohl,
md
; Amy McMichael,
md
;Elise A. Olsen,
md
; David M. Pariser,
md
; Daniel Piacquadio,
md
; Vera Price,
md
; Geoffrey P. Redmond,
md
; DavidRodriguez,
md
; Marty E. Sawaya,
md
,
p
h
d
; Jonathan S.Weiss,
md
; David A. Whiting,
md
; David C. Wilson,
md
;John E. Wolf Jr,
md
.
Acknowledgments
This work was supported in part by a grant from Bristol-Myers Squibb.
References
1 Barth JH, Catalan J, Cherry CA,
et al.
Psychological morbidity in women referred for treatment of hirsutism.
J Psychosom Res
1993;
37
: 615–619.2 Sonino N, Fava GA, Fallo F,
et al.
Psychological distress and quality of life in endocrine disease.
Psychother Psychosom
1990; 54: 140–144.
3 Rabinowitz S, Cohen R, Le Roith D. Anxiety and hirsutism. Psychol Rep 1983; 53: 827–830.
4 Consoli SM, Vexiau P, Consoli SG, et al. Acceptability, tolerance and quality of life impact of cyproterone acetate treatment in female hirsutism. Comparison of 2 protocols in combination with oral or transdermal estradiol. Contracept Fertil S 1994; 22: 783–787.
5 Kramer AM. Rehabilitation care and outcomes from the patient’s perspective. Med Care 1997; 35 (6 Suppl.): JS48–JS57.
6 Phillips C. Patient-centered outcomes in surgical and orthodontic treatment. Semin Orthod 1999; 5: 223–230.
7 Abetz L, Jacoby A, Baker GA, et al. Patient-based assessments of quality of life in newly diagnosed epilepsy patients: validation of the NEWQOL. Epilepsia 2000; 41: 1119–1128.
8 Kosinski M, Zhao SZ, Dedhiya S, et al. Determining minimally important changes in generic and disease-specific health-related quality of life questionnaires in clinical trials of rheumatoid arthritis. Arthritis Rheum 2000; 43: 1478–1487.
9 Wolf JE, Shander D, Huber F, et al., and Eflornithine HCl Study Group. Randomized, double-blind clinical evaluation of the efficacy and safety of topical eflornithine HCl 13.9% cream in the treatment of women with facial hair. Int J Dermatol 2007; 46: 94–98.
10 Caro JJ, Caro G, O’Brien JA, et al. Assessing quality of life implication of depigmentation: the BASC scale. Available at: http://gateway.nlm.nih.gov/MeetingAbstracts/102222508.html
11 Cleeland C. Assessment of pain in cancer: measurement issues. Adv Pain Res Ther 1990; 16: 47–55.
12 Goodman LA, Kruskal WH. Measures of association for cross-classification IV: simplification of asymptotic variances. J Am Statist Assoc 1972; 67: 415–421.
13 Lohr KN, Aaronson NK, Alonso J, et al. Evaluating quality-of-life and health status instruments: development of scientific review criteria. Clin Ther 1996; 18: 979–992.
14 Lydick E, Epstein RS. Interpretation of quality of life changes. Qual Life Res 1993; 2: 221–226.
15 Jaeschke R, Singer J, Guyatt GH. Measurement of health status: ascertaining the minimal clinically important difference. Control Clin Trials 1989; 10: 407–415.
16 Juniper EF, Guyatt GH, Willan A, et al. Determining a minimal important change in a disease specific quality of life questionnaire. J Clin Epidemiol 1994; 47: 81–87.
17 Osoba D, Rodrigues G, Myles J, et al. Interpreting the significance of changes in health-related quality-of-life scores. J Clin Oncol 1998; 16: 139–144.
18 Samsa G, Edelman D, Rothman ML, et al. Determining clinically important differences in health status measures, a general approach with illustration to the health utilities index mark II. Pharmacoeconomics 1999; 15: 141–155.
19 Guyatt GH, Juniper EF, Walter SD, et al. Interpreting treatment effects in randomised trials. Br Med J 1998; 316: 690–693.
20 Juniper EF, Guyatt GH, Ferrie PJ, Griffith LE. Measuring quality of life in asthma. Am Rev Respir Dis 1993; 147: 832–838.
21 Ware JE, Snow KK, Kosinski M, et al. SF-36 Health Survey: Manual and Interpretation Guide. Town/state: The Health Institute, New England Medical Center, Boston, MA, 1993.
22 Guyatt GH, Osoba D, Wu AW, et al. Methods to explain the clinical significance of health status measures. Mayo Clin Proc 2002; 77: 371–383.
23 Sonino N, Fava GA, Mani E, et al. Quality of life of hirsute women. Postgrad Med J 1993; 69: 186–189.
24 Fava GA, Grandi S, Savron G, et al. Psychosomatic assessment of hirsute women. Psychother Psychosom 1989; 51: 96–100.
Top Related