







Languages
Pages
Legal


The disease and Panbio product training
HHV-6

Overview• First isolated in 1986 from patients with AIDS• The main clinical syndrome associated with the virus,
roseola infantum, was first reported in 1913• It wasn’t until 1988 that the link between HHV-6 and
roseola infantum was established.[1]• Ubiquitous virus which causes disease in both normal
and immunocompromised individuals• HHV-6 is a viable candidate as a possible etiological
agent in multiple sclerosis.

Infectious Agent• Belongs to the Betaherpesvirus subfamily and
genetically similar to HHV-7 and CMV– cross reactivity between HHV-6 and CMV is quite
common[2].
• Two distinct variants - HHV-6A and HHV-6B– Can be differentiated using monoclonal antibodies and PCR
• Incubation period about 10 days

Epidemiology• Approximately 90% of normal children are infected
during infancy, with the peak age of 6-9 months.[1] • In Western populations most children are infected by
the age 3 years, and the majority of these with HHV6-B.[2]
• Transmission via saliva from infected individuals, blood transfusion and organ transplantation.[4]
• Incidence is greatest in Spring

Pathogenesis• CD4+ T-lymphocytes are the preferential cell for HHV-
6 to infect, with the surface marker CD46 acting as part of a co-receptor for infection.[5] This in turn results in a number of significant effects on the immune system.
• HHV-6 infection persists for an extended period, with the virus able to establish latency in a number of different cells and organs.

Clinical NotesInfection in childhood• Exanthema subitum (Roseola infantum or sixth
disease)– Occurs in infants
– High fever that lasts 3-5 days
– Maculopapular rash (Physicians can mistake these signs for allergic reactions to antibiotics.[1] )
– Associated with febrile convulsions in 12-15 month old children.
– Febrile form usually self-limiting and does not require specific therapeutic intervention

Clinical infection
Immunocompromised patients• Reactivation of HHV-6 infection may result in fever,
skin rash, pneumonitis, encephalitis and even bone marrow suppression.
• Reactivation in bone marrow transplant patients has a particularly high incidence of 48%.[1]
• High frequency of HIV-infected patients that suffer from HHV-6 reactivation resulting in pneumonitis and encephalitis.
• HHV-6 has been increasingly associated with conditions such as MS and malignancies such as Hodgkin’s disease, non-Hodgkin’s lymphoma, acute lymphoblastic leukaemia, oral carcinoma and cervical carcinoma.

Antibody Response• Although many newborns maternally acquire HHV-6
antibodies they become seronegative by 6 months.• Antibody levels may be elevated in patients with
infectious mononucleosis (IM), chronic fatigue, Hodgkin's disease & oral and cervical carcinoma.
• Primary infection– IgM detectable 5-7 days after febrile phase of Roseola
– IgG appears 7-10 days after the febrile phase of Roseola and usually persists for life.

Diagnosis• Clinically may be confused with measles and rubella
because of similar rash.• Laboratory confirmation essential to ensure
effectiveness of measles and rubella surveillance programs.
• Diagnostic tests– IFA
– Viral isolation
– PCR
– ELISA

Why Test for HHV-6?• Ubiquitous virus that causes a wide range of disease.• Because it is common, immunocompromised patients are
more likely to come into contact with individuals who are suffering from primary HHV-6 infection.
• Transplant patients who are being medicated against graft rejection are particularly susceptible.
• HIV-infected individuals are also susceptible.• Whilst HHV-6 usually causes a benign, self-limiting disease
in children, there are a number of cases that progress to serious life-threatening states of the disease.
• As IgM to HHV-6 can cross react with a number of other viral antigens such as CMV and EBV, testing of both HHV-6 IgG and IgM affords the physician with a clearer picture as to whether an individual preparing to undergo transplantation is at risk of reactivation or primary infection.

Diagnostic Tests• Virus isolation
– has been successful in primary infections, usually when rash is present.
– time-consuming
• PCR– useful for variant discrimination
– useful in viremic part of disease - usually first 3-4 days after illness only
• IFA– useful for confirmation and small scale testing
• ELISA – for IgG and IgM antibodies
– use in conjunction with IFA for confirmation

Diagnostic Tests
Virus IsolationPCR
IgM ELISA or IFA
IgGELISA or IFA
Panbio HHV-6 IFA Products• HHV-6 IgG IFA kit 120T Cat# I-HV601G• HHV-6 IgG IFA kit 40T Cat# I-HV603G• HHV-6 IgM IFA kit 120T Cat# I-HV601M• HHV-6 IgM IFA kit 40T Cat# I-HV603M• HHV-6 IFA Slides 10x10well Cat# I-HV601X


Panbio HHV-6 IgG and IgM IFA• Bright green fluorescent staining = positive• Fluorescent staining pattern of HHV-6 infected cells is
variable.– Depending on the cell’s stage of infection, the fluorescent pattern
can vary from a small portion of the infected cell fluorescing to the whole cell fluorescing.
– Fluorescence can also range from granular to homogeneous.
• To provide an internal control, each well contains both HHV-6 infected and uninfected cells. Preparation of the slide in this manner is intentional.
– Uninfected cells, stained red by the counterstain, provide a contrasting background.
– Infectivity of the cells ranges from 20% - 60%.
• Absence of specific fluorescent staining of the infected cells denotes a negative reaction.
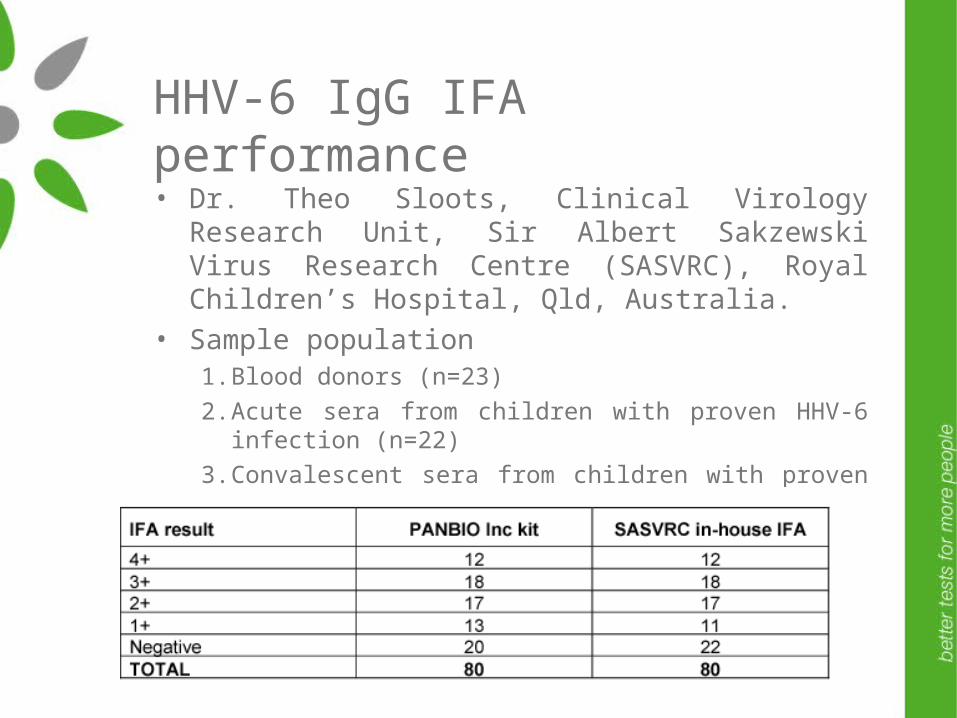
HHV-6 IgG IFA performance• Dr. Theo Sloots, Clinical Virology Research Unit, Sir
Albert Sakzewski Virus Research Centre (SASVRC), Royal Children’s Hospital, Qld, Australia.
• Sample population1. Blood donors (n=23)
2. Acute sera from children with proven HHV-6 infection (n=22)
3. Convalescent sera from children with proven HHV-6 infection (n=35)
• Agreement of 95% (76/80)

Panbio HHV-6 IgM ELISA• HHV-6 IgM ELISA Cat # E-HV601M• For the presumptive qualitative detection of IgM to
HHV-6 in serum as an aid in the clinical laboratory diagnosis of primary of reactivated HHV-6 infection in patients presenting clinical symptoms consistent with HHV-6 infection.


Panbio HHV-6 IgM ELISAPerformance• Package insert• Study 1
– 149 serum samples (98 Aust blood donors and 40 positives characterised by in-house IFA)
– Serological sensitivity = 52.5%
– Clinical specificity = 87.8%
– Relative agreement = 77.5%
• Cross reactivity– Cross reactivity observed with CMV and EBV primarily
Panbio HHV-6 IgG ELISA• HHV-6 IgG ELISA Cat # E-HV601G• For the qualitative detection of IgG to HHV-6 in serum
as an aid in diagnosis of recent or past exposure to HHV-6
• Paired sera required to determine recent infection if using IgG alone
Panbio HHV-6 IgG ELISAPerformance• Sloots et al., 1996, J. Clin. Micro
– Sensitivity 99.8%, Specificity 98.8%
• Package insert– 212 serum samples characterised by public hospital
lab’s in-house IFA
– Clinical sensitivity = 97.4%
– Serological specificity = 86.0%
– Serological agreement = 94.3%

Comments from Dr Sloots• The kit was easy to use and reagents were adequate• Good cell numbers were present per well• Strong apple-green fluorescence was present at 4+• The fluorescence of positive reactions (4+ to 1+) was
easily discriminated from the negative reaction• The percentage of infected cells per field was high
(70%)
Further performance data is found in the HHV-6 IgG IFA package insert

Promotional Resources• Clinical notes sheet• Colour brochure – in process of being updated• Publications
– General
– Panbio HHV-6 IgG ELISA

References1. Abdel-Haq, N.M., Asmar Basim, I. (2004). Human herpesvirus 6 (HHV6) infection.
The Indian Journal of Pediatrics. 71(1):89-96.2. Irving, W.L., et al. (1990). Dual antibody rises to cytomegalovirus and human
herpesvirus type 6: frequency of occurrence in CMV infections and evidence for genuine reactivity to both viruses. Journal of Infectious Diseases. 161(5): 910-916.
3. Caserta, M.T., Mock, D.J., Dewhurst, S. (2001). Human herpesvirus 6. Clinical Infectious Diseases. 33(6): 829-833.
4. Okuno, T., et al. (1989). Seroepidemiology of human herpesvirus 6 infection in normal children and adults. Journal of Clinical Microbiology. 27(4): 651-653.
5. Lau, Y.L., et al. (1998). Primary human herpes virus 6 infection transmitted from donor to recipient through bone marrow infusion. Bone Marrow Transplant. 21(10): 1063-1066.
6. Santoro, F., et al. (1999). CD46 is a cellular receptor for human herpesvirus 6. Cell. 99(7): 817-827.
7. Steeper, T.A., et al. (1990). The spectrum of clinical and laboratory findings resulting from human herpesvirus-6 (HHV-6) in patients with mononucleosis-like illnesses not resulting from Epstein-Barr virus or cytomegalovirus. American Journal of Clinical Pathology. 93(6): 776-783.
8. Dockrell, D.H., Paya, C.V. (2001) Human herpesvirus-6 and –7 in transplantation. Reviews in Medical Virology. 11(1): 23-36.

Top Related