





Languages
Pages
Legal


The Diagnostic Evaluation and Treatment of Recurrent Pregnancy Loss
Ashim Kumar, M.D.Ashim Kumar, M.D.Reproductive Endocrinology and InfertilityReproductive Endocrinology and Infertility
Clinical Assistant Professor, Clinical Assistant Professor, UCLA School of MedicineUCLA School of Medicine
Fertility & Surgical Associates of California,
Encino & Thousand Oaks, CA

Luteal SupportLuteal Support
Progesterone +/- EstradiolProgesterone +/- Estradiol Start after ovulation or egg retrievalStart after ovulation or egg retrieval Continue until 10 weeks gestational Continue until 10 weeks gestational
ageage

Early PregnancyEarly Pregnancy
ReassuranceReassurance UltrasoundsUltrasounds Pelvic rest as neededPelvic rest as needed As IndicatedAs Indicated
Monitor TSHMonitor TSH Monitor BPMonitor BP

Prenatal TestingPrenatal Testing ScreeningScreening
11stst Trimester – Nuchal Fold + Serum Trimester – Nuchal Fold + Serum 22ndnd Trimester – Triple/Quadruple Screen Trimester – Triple/Quadruple Screen
DiagnosticDiagnostic 11stst Trimester – Chorionic Villus Sampling Trimester – Chorionic Villus Sampling 22ndnd Trimester – Amniocentesis Trimester – Amniocentesis

Recurrent Pregnancy LossRecurrent Pregnancy Loss SAB: involuntary loss of pregnancy before SAB: involuntary loss of pregnancy before
20wk GA20wk GA RPL: Three or more pregnancy losses in the RPL: Three or more pregnancy losses in the
first trimesterfirst trimester
Indications to evaluate after 2 or more consecutive losses: + FCA in prior loss Normal Karyotype on prior loss Female > 35yr Infertility
Emotional Support is critical

Risk of RPL in Young WomenRisk of RPL in Young Women# of Prior SAB’s# of Prior SAB’s % Risk of SAB % Risk of SAB
in Next in Next PregnancyPregnancy
h/o prior h/o prior livebornliveborn
00 12%12%
11 24%24%
22 26%26%
33 32%32%
44 26%26%
66 53%53%
No livebornNo liveborn 2 or more2 or more 40-45%40-45%

Early Pregnancy LossEarly Pregnancy Loss Clinically unrecognized (less than 8wk GA)Clinically unrecognized (less than 8wk GA) 30-60% of all pregnancies end in SAB30-60% of all pregnancies end in SAB
At least ½ are early losses (go unnoticed)At least ½ are early losses (go unnoticed) ~75% of embryos with chromosomal ~75% of embryos with chromosomal
abnormalities abnormalities 90% are numerical (aneuploidy/polyploidy)90% are numerical (aneuploidy/polyploidy) Rest are structural or mosaicismRest are structural or mosaicism 2/3 of the remaining 25% with normal 2/3 of the remaining 25% with normal
karyotype exhibit gross structural karyotype exhibit gross structural abnormalitiesabnormalities

EtiologyEtiology Uterine Defect (~30%)Uterine Defect (~30%)
Congenital Congenital AcquiredAcquired
ThrombophiliaThrombophilia CongenitalCongenital Immunologic (~3-5%)Immunologic (~3-5%)
GeneticGenetic Meiotic NondisjunctionMeiotic Nondisjunction Balanced Translocation (5%)Balanced Translocation (5%)
General EndocrineGeneral Endocrine

Uterine DefectUterine Defect CongenitalCongenital
SeptumSeptum Bicornuate / UnicornuateBicornuate / Unicornuate T-Shaped UterusT-Shaped Uterus
AcquiredAcquired Submucosal LeiomyomaSubmucosal Leiomyoma Endometrial PolypEndometrial Polyp SynechiaSynechia AdenomyosisAdenomyosis

Uterine EvaluationUterine Evaluation
UltrasoundUltrasound Sonohysterogram Sonohysterogram
(saline ultrasound)(saline ultrasound) HysterosalpingogramHysterosalpingogram MRIMRI HysteroscopyHysteroscopy

Bicornuate or SeptateBicornuate or Septate

Endometrial PolypEndometrial Polyp

ThrombophiliasThrombophilias CongenitalCongenital
Factor V Leiden MutationFactor V Leiden Mutation Protein C / Protein S DeficiencyProtein C / Protein S Deficiency Prothrombin Gene MutationProthrombin Gene Mutation Methylenetetrahydrofolate Reductase Methylenetetrahydrofolate Reductase
(MTHFR) – homocysteine(MTHFR) – homocysteine Antithrombin IIIAntithrombin III
Immunologic - Antiphospholipid Immunologic - Antiphospholipid SyndromeSyndrome Anticardiolipin AntibodiesAnticardiolipin Antibodies Lupus AnticoagulantLupus Anticoagulant

Virchow’s TriadVirchow’s Triad
Stasis (Decrease flow in placental vessels)Stasis (Decrease flow in placental vessels) Damaged VasculatureDamaged Vasculature Hypercoagulable StateHypercoagulable State
CancerCancer Pregnancy (Elevated Estradiol leads to Pregnancy (Elevated Estradiol leads to
increased hepatic production of clotting increased hepatic production of clotting factors)factors)
CongenitalCongenital ImmunologicImmunologic

GeneticGenetic Meiotic NondisjunctionMeiotic Nondisjunction
Risk of miscarriage increases with Risk of miscarriage increases with advancing reproductive ageadvancing reproductive age
Balanced Translocation (5% of couples)Balanced Translocation (5% of couples) RobertsonianRobertsonian ReciprocalReciprocal
OthersOthers MosaicismMosaicism InversionInversion
Chromosomally abnormal sperm do not Chromosomally abnormal sperm do not play a role in RPLplay a role in RPL

Meiotic NondisjunctionMeiotic Nondisjunction

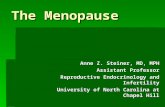
Age and Miscarriage RiskAge and Miscarriage Risk

Risk of Chromosomal AbnormalityRisk of Chromosomal Abnormalityin Newborns by Maternal Agein Newborns by Maternal Age
Maternal Age (years)
Risk for Down Syndrome
Total Risk for Chromosomal Abnormalities
20 1/1,667 1/52625 1/1,250 1/47630 1/952 1/38535 1/378 1/19240 1/106 1/6641 1/82 1/5342 1/63 1/4243 1/49 1/3344 1/38 1/2645 1/30 1/2146 1/23 1/1647 1/18 1/1348 1/14 1/1049 1/11 1/8
Maternal Fetal Medicine: Practice and Principles. Maternal Fetal Medicine: Practice and Principles.
Creasey and Resnick 1994Creasey and Resnick 1994

Preimplantation Genetic DiagnosisPreimplantation Genetic Diagnosis

Preimplantation Genetic DiagnosisPreimplantation Genetic Diagnosis

Preimplantation Genetic DiagnosisPreimplantation Genetic Diagnosis

Robertsonian TranslocationRobertsonian Translocation

Reciprocal TranslocationReciprocal Translocation

General EndocrineGeneral Endocrine
Diabetes (Fasting Glucose)Diabetes (Fasting Glucose) Thyroid Disease (TSH)Thyroid Disease (TSH) Hyperprolactinemia (Prolactin)Hyperprolactinemia (Prolactin) Polycystic Ovary SyndromePolycystic Ovary Syndrome Luteal Phase Deficiency Luteal Phase Deficiency
(Supplement Everyone)(Supplement Everyone)

TreatmentTreatment Provide Emotional SupportProvide Emotional Support Uterus Uterus
Resect lesionResect lesion Hypercoagulable State Hypercoagulable State
HeparinHeparin AspirinAspirin FolateFolate
Genetic Genetic PGDPGD
General Endocrine General Endocrine Correct hormonal imbalanceCorrect hormonal imbalance

What Does Not WorkWhat Does Not Work
Alloimmune DisordersAlloimmune Disorders TestingTesting
HLA testingHLA testing Mixed lymphocyte Mixed lymphocyte
cultureculture Natural killer cell assayNatural killer cell assay
TreatmentTreatment Paternal leukocyte Paternal leukocyte
immunizationimmunization Intravenous Intravenous
immunoglobulins (IVIG)immunoglobulins (IVIG)
GeneticGenetic PGDPGD
Hypercoagulable Hypercoagulable StateState GlucocorticoidsGlucocorticoids
UterusUterus MetroplastyMetroplasty

ConclusionConclusion
The likelihood of successful delivery is The likelihood of successful delivery is very high. The challenge is to do it an a very high. The challenge is to do it an a cost-effective fashion while being sensitive cost-effective fashion while being sensitive to the emotional sequelae.to the emotional sequelae.
Top Related