






Languages
Pages
Legal

1
Telemedicine and Health Reform
Jonathan Neufeld, PhDClinical Director
Upper Midwest Telehealth Resource Center

telehealthresourcecenters.org
• Links to all TRCs
• National Webinar Series
• Reimbursement, Marketing, and Training Tools
UMTRC Services
• Presentations & Trainings
• Consultation
• Technical Assistance
• Connections with other programs
• Program Design and Evaluation
• Information on current legislative and policy developments
Definitions and Concepts - I
Telehealth and Telemedicine
• Sometimes used interchangeably
• Two types of distinctions -
• Telemedicine = billable interactive clinical services
• Telehealth =• Broader field of distance health activities (CME, etc.)• Clinical remote monitoring (usually at home)
Basic Concept
TELEMEDICINE
Explosion of Health Services
• Patients, doctors, hospitals, pharmacies
• Nursing homes
• Specialty hospitals, surgery centers, etc.
• Purchasers, wellness services
• Internet, PDAs, cell phones
• Lifestyle drugs and services
• Social networks, ubiquitous communication
Any service, any place, any time.
Historical Snapshot of Telemedicine
• Used at Nebraska Psychiatric Institute in 1955
• Developed extensively by NASA in 1960’s
• VA started in 1990’s – CCHT Program• Pilot in VISN 8 in 2003 – 63% reduction in ER
visits, 88% reduction in SNF days
• 2012 Utilization: 0.5 M patients; 1.5 M episodes
• Added by Medicare in 1996 (multiple updates)
• Regulations requiring Medicaid and commercial coverage in states began about the same time
• Wave of equipment and program grants, projects
Definitions and Concepts - II
● TM is not a service, but a delivery mechanism for health care services– Most TM services duplicate in-person care– Some are made better or possible with TM– Reimbursement equal to “in-person” care
Definitions and Concepts - III● New payment model conundrum
– Many of the benefits of TM are only available under new payment models
– Motivations of FFS are “unaligned”● Example: Home Monitoring
– Increase adherence– Reduce re-hospitalizations– Improve outcomes
*** Billing FFS for monitoring fails ***
Getting “Value” from Telehealth
Strategies Dependent Upon:● Revenue Stream● Cost Avoidance● Shared Savings● Improved Quality
**Each may appeal to different stakeholders
Recent Headline
“Telemedicine helps hospitals
double revenue.”
A Better Type of Value
Triple Aim:
Better Care – Better Health – Lower Cost
• Patients have a better experience
• They (all) get healthier
• It all costs less (to everyone)
Future Health Care
● Outcome goal: population health– Overall and within target sub-populations
● Measure: inpatient days per 1000– Healthier people stay out of the hospital
● Intervention targets:– Patient engagement in self-care, bio trends– Pt knowledge, skills, attitudes, behaviors
Future Health Care
Providers will be accountable for patient behaviors
(or at least patient engagement)
How does Telemedicine fit in?
Telemedicine Reimbursement (FFS)● Medicare
– Limited CPTs– Rural areas
● Medicaid– State-specific– IN, IL, MI yes; OH no (but possible soon)
● Private Payers– Most provide coverage similar to Medicare
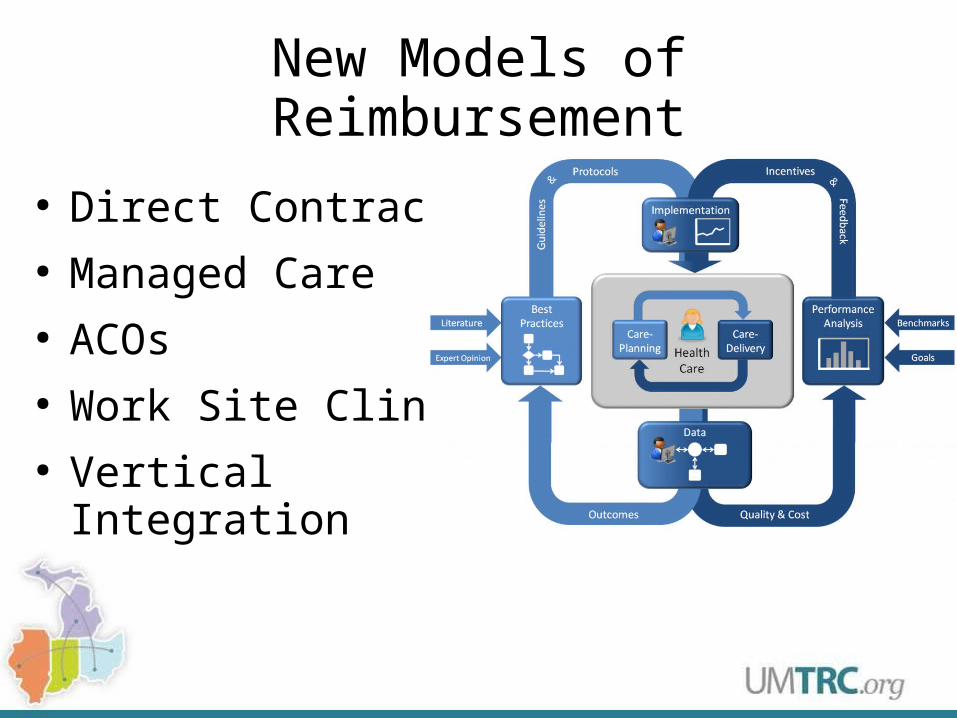
New Models of Reimbursement
● Direct Contracts● Managed Care● ACOs● Work Site Clinics● Vertical Integration
Re-ordering the Clinical Enterprise
Three Basic “Types” or Domains
Hospitals & Specialties
• Specialists see and manage patients remotely
Integrated Care
• Mental health and other specialists work in primary care settings (e.g., PCMH’s, ACO’s)
Transitions & Monitoring
• Patients access care (or care accesses patients) where and when needed to avoid complications and higher levels of care
“Value” Varies by Domain
Hospital & Specialty Care
• Market aggregation, using the long tail
Integrated Primary Care and Health Homes
• Service aggregation, one stop shopping
Transitions
• Continuity, engagement, momentum
Right service, right place, right time.
New Challenge
“Right service, right place, right time.”
Right for what? Or for whom?
Right Goal? Right Outcome Measure?
Maybe research can tell us…
Research Context
• 20+ years of rigorous research (varies)
• 11 current standards/guidelines documents
Summary of Findings:
When used appropriately, medical care delivered via telemedicine is
• as effective
• as satisfactory (to patients and providers)
• as efficient
as the same services delivered via traditional in-person medical care.
Research Context
Caveats:
1. Every telemedicine program is different
2. Some telemedicine services are novel (most are not)
3. Some services offset other services
4. Not all medical treatments are effective (but we still provide them)
“Value” Factors
1. Payment: FFS vs. Risk-based/Alternative
2. Medical Staff: Salaried vs. Independent
3. Treatment Focus: Chronic vs. Acute Care
4. Temporal Horizon: Present vs. Future
Federal Telemedicine Law & PolicyProfessionals are regulated at the state level
(doctors, nurses, counselors, etc.)
Medicare: Pays for certain outpatient professional services (CPT codes) for patients accessing care in rural counties and HPSAs in rural census tracts.
*No regs; only conditions of payment.
Medicaid: Telemedicine is “a cost-effective alternative to the more traditional face-to-face way of providing medical care…that states can choose to cover.”
Indiana Telemedicine Law & Policy
Medical Board/Licensure
• Indiana medical license includes:
“Providing diagnostic or treatment services to a person in Indiana when the diagnostic or treatment services: are transmitted through electronic communications; and are on a regular, routine, and non-episodic basis or under an oral or written agreement to regularly provide medical services.”
Indiana Telemedicine Law & Policy
PrescribingExcept in institutional settings, on-call situations, cross-coverage situations, and [when supervising NPs],
a physician shall not prescribe, dispense, or otherwise provide, or cause to be provided, any legend drug that is not a controlled substance to a person who the physician has never personally physically examined and diagnosed
unless the physician is providing care in consultation with another physician who has an ongoing professional relationship with the patient, and who has agreed to supervise the patient's use of the drug or drugs to be provided.
Indiana Telemedicine Law & Policy
Medicaid Reimbursement (April 1, 2007)
• The member must be present and able to participate in the visit.
• The audio and visual quality of the transmission must meet the needs of the physician located at the hub site.
• When ongoing services are provided, the member should be seen by a physician for a traditional clinical evaluation at least once a year, unless otherwise stated in policy. In addition, the hub physician should coordinate with the patient’s primary care physician.
Indiana Telemedicine Law & Policy
Medicaid Reimbursable Codes
• Consultations – 99241 to 99245 and 99251 to 99255
• Office or other outpatient visit – 99201 to 99205 and 99211 to 99215
• Individual psychotherapy – 90832 to 90840
• Psychiatric diagnostic interview – 90791, 90792
• End stage renal disease services (ESRD) – G0308, G0309, G0311, G0312, G0314, G0315, G0317, and G0318
• 90862 deprecated; replaced by E&M codes
Indiana Telemedicine Law & Policy
Documentation
1. Documentation must indicate the services were rendered via telemedicine.
2. Documentation must clearly indicate the location of the hub and spoke sites.
3. All other IHCP documentation guidelines for services rendered via telemedicine apply, for example chart notes and start and stop times. Documentation must be available for post-payment review.
Indiana Telemedicine Law & Policy
Documentation
4. Providers must have written protocols for circumstances when the member must have a hands-on visit with the consulting provider. The member should always be given the choice between a traditional clinical encounter versus a telemedicine visit. Appropriate consent from the member must be obtained by the spoke site and maintained at the hub and spoke sites.
Indiana Telemedicine Law & Policy
Medicaid Special Conditions
• IHCP reimburses for telemedicine services, only when the hub and spoke sites are greater than 20 miles apart.
• Federally Qualified Health Centers (FQHC) or Rural Health Clinics (RHC) are only reimbursed for hands-on services and are therefore not permitted to bill for telemedicine services.
Indiana Telemedicine Law & Policy
EA 554 (effective July 1, 2013)
• Medicaid will reimburse home health agencies for “telehealth services”
• “Use of telecommunications and information technology to provide access to health assessment, diagnosis, intervention, consultation, supervision, and information across a distance.”
• Medicaid will reimburse FQHCs and RHCs for telemedicine services
• Medicaid will reimburse regardless of distance between provider and patient
Review of Key Points
• TM is a delivery mechanism, not a service
• TM usually replicates in-person care
• TM provides multiple types of value
• TM value is embedded in larger movements in health care
• Reimbursement is now available for Indiana RHCs and FQHCs (awaiting regs)
• Licensed home health agencies will be reimbursed for “telehealth” (monitoring) services.

Contact Information
Jonathan Neufeld, PhD
(574) 606-5038
www.telehealthresourcecenters.org
Top Related