






Languages
Pages
Legal

Strategic Risk Report
1 March 2018

Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
2 1.3.18
Introduction The Strategic Risk Report (historically known as the Board Assurance Framework) evidences Haringey Clinical Commissioning Group’s control over the delivery of its strategic objectives listed above. This report directly underpins the Annual Governance Statement (AGS) and is the subject of annual enquiry by Internal and External Audit.
Function of the Strategic Risk Report This report is a tool for the Governing Body corporately to assure itself (gain confidence, based on evidence) about successful delivery of the organisation’s strategic objectives. The framework is designed to focus the Governing Body on controlling principal risks threatening the delivery of those objectives. It aligns principal risks, key controls and assurances on controls alongside each objective. Oversight of the management of individual risks is assigned to relevant Governing Body Committees. Where gaps are identified and key controls and assurances are insufficient to reduce the risk of non-delivery of objectives, action plans will be created where appropriate and overseen by the responsible committee. The Senior Management Team and the Audit Committee routinely review all risk on the Risk Register, whereas the Governing Body receives a more high-level Strategic Risk Report, containing risks rated 12 and above. The purpose of the Strategic Risk Report may be summarised as: To provide:
a comprehensive method for the effective and focused management of the principal risks to achieving strategic objectives; and
a basis for the preparation of a fair and representative Annual Governance Statement.
Governing Body responsibility for the Strategic Risk Report
It is the responsibility of the Governing Body as the corporate head of the CCG to: Establish strategic objectives. Identify the principal risks that threaten the achievement of these objectives. Identify and evaluate the design of key controls intended to manage these principal risks. Set out the arrangement for obtaining assurance on the effectiveness of key controls across all areas of principal risk Evaluate the assurance across all areas of principal risk. Identify positive assurances and areas where there are gaps in controls and / or assurances Ensure that plans are put in place to take corrective action where gaps have been identified in relation to principal risks and receive
assurance Maintain dynamic risk management arrangements including, crucially, a well-founded risk register. Open risks and recently closed risks are set out in pages 6-17.
Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
3 1.3.18
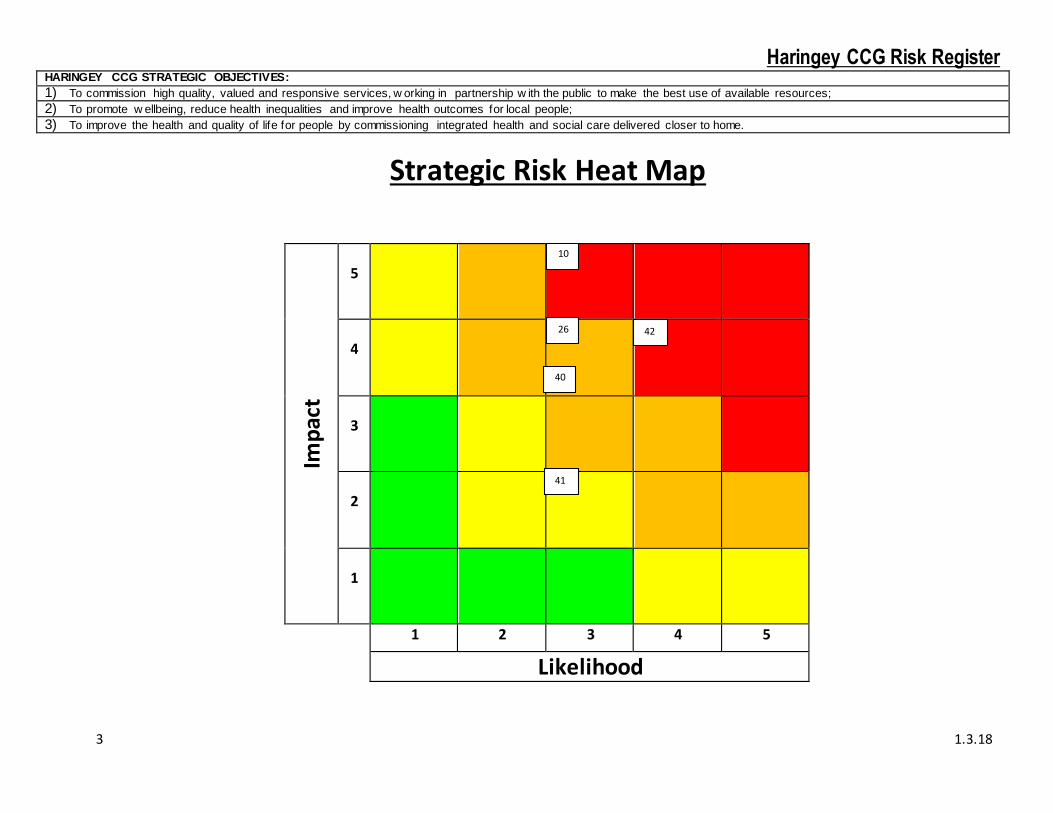
Strategic Risk Heat Map
Imp
act
5
4
3
2
1
1 2 3 4 5
Likelihood
10
26
=
40
41
42
Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
4 1.3.18
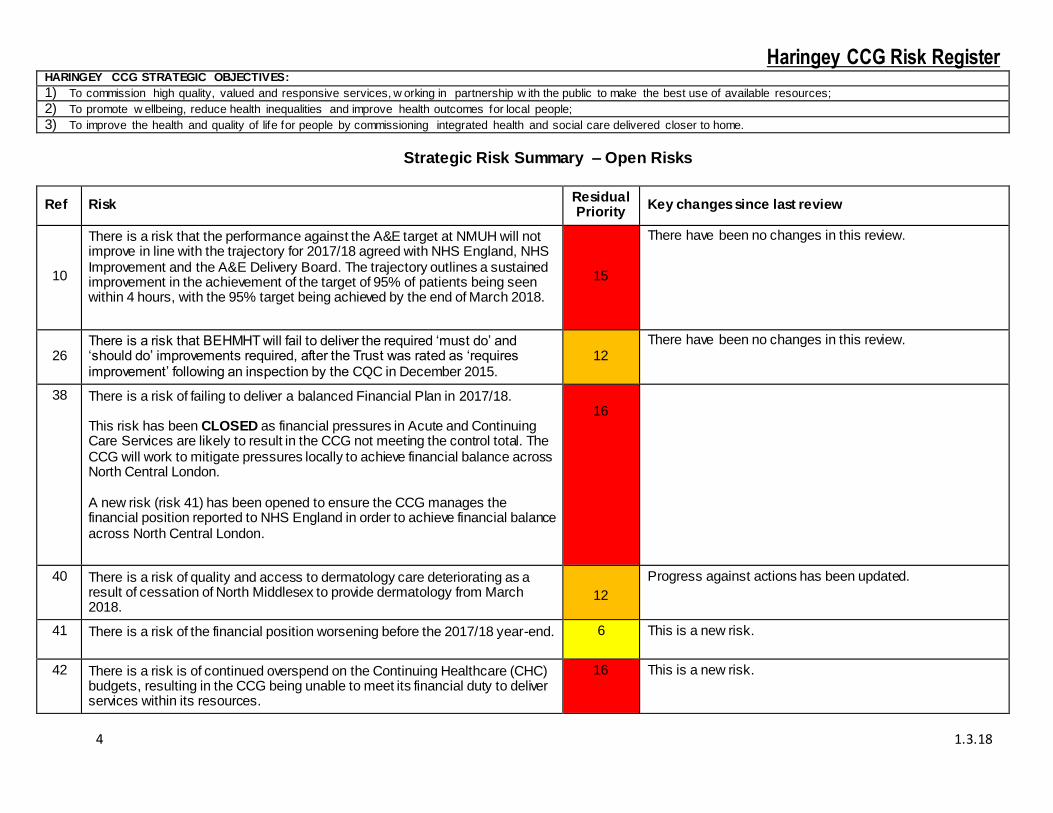
Strategic Risk Summary – Open Risks
Ref Risk Residual Priority
Key changes since last review
10
There is a risk that the performance against the A&E target at NMUH will not improve in line with the trajectory for 2017/18 agreed with NHS England, NHS Improvement and the A&E Delivery Board. The trajectory outlines a sustained improvement in the achievement of the target of 95% of patients being seen within 4 hours, with the 95% target being achieved by the end of March 2018.
15
There have been no changes in this review.
26 There is a risk that BEHMHT will fail to deliver the required ‘must do’ and ‘should do’ improvements required, after the Trust was rated as ‘requires improvement’ following an inspection by the CQC in December 2015.
12 There have been no changes in this review.
38 There is a risk of failing to deliver a balanced Financial Plan in 2017/18. This risk has been CLOSED as financial pressures in Acute and Continuing Care Services are likely to result in the CCG not meeting the control total. The CCG will work to mitigate pressures locally to achieve financial balance across North Central London. A new risk (risk 41) has been opened to ensure the CCG manages the financial position reported to NHS England in order to achieve financial balance across North Central London.
16
40 There is a risk of quality and access to dermatology care deteriorating as a result of cessation of North Middlesex to provide dermatology from March 2018.
12
Progress against actions has been updated.
41 There is a risk of the financial position worsening before the 2017/18 year-end.
6 This is a new risk.
42 There is a risk is of continued overspend on the Continuing Healthcare (CHC) budgets, resulting in the CCG being unable to meet its financial duty to deliver services within its resources.
16 This is a new risk.

Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
5 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
10
1,2,3 (Background: NHS England‘s expectation is that all NHS Trust’s performance against the
4 hour target will show month on month improvement).
There is a risk that the performance against the A&E
target at NMUH will not improve in line with the trajectory for 2017/18 agreed with NHS
England, NHS Improvement and the A&E Delivery Board. The
trajectory outlines a sustained improvement in the achievement
of the target of 95% of patients being seen within 4 hours, with
the 95% target being achieved by the end of March 2018.
Risk Owner
Tony Hoolaghan, Chief Operating Officer
Lead Committee Finance and Performance
Committee and Quality Committee
Risk reworded in its current form
4.4.17
Causes
Poor patient flow throughout the Trust and back in to the
community
Too much reliance on inpatient beds and
admitting patients.
Inconsistent
implementation of agreed new ways of working in the
department.
Lack of senior clinical
leadership within the Emergency
Department (ED).
Consultant and middle grade vacancies
leading to inconsistent senior cover for ED
Workforce challenges within the A&E department are
impacting on the trust’s ability to deliver high
quality care.
Effects
Too many patients waiting an unacceptably long time
for assessment and
I = 4
L = 5
20
1. The Trust is acting on
recommendations from the Emergency Care Improvement
Programme to improve streaming and patient flow through the
department, particularly at times of pressure.
2. Embedding of the “ Safer, Faster Better” (SFB) work via four
workstreams.
3. Refresh of A&E Delivery Board governance in October 2017. The
Trust CEO now chairs the Delivery Board.
4. Use of the quality surveillance process to escalate emerging
concerns about quality and safety and ensure a single shared view of
risks to quality and safety in the A&E department.
5. In 2017/18 a programme of CCG led Insight Visits to NMUH
will be informed by CQC recommendations and the Trust
Improvement Plan.
1/2. CCG (and partners) to continue to review
SFB programme progress at monthly A&E
Delivery Board meetings. The Director of
Performance, Planning and Delivery attends Safer, Faster, Better
steering group.
1/2. Bespoke programme
governance created to oversee the programme
and link to wider Trust improvement
programme.
1/2. Dedicated
Programme resource in place.
3. A&E Delivery Board minutes provide
evidence that performance
improvement and target recovery are overseen effectively and
appropriate challenge is made.
I = 5
L = 3
15
Actions
1. CCG acting as convenor and lead for
Out of Hospital workstream of the SFB
programme. Weekly project team
meetings set up and partner organisation
membership agreed.
Action owner Marco Inzani,
Head of Integrated Commissioning (Adults)
Implementation date
From 30.5.16
2. Recovery target
agreed and managed as part of the STF
(Sustainability and Transformation Fund) arrangements for
2017/18.
1/2.
Haringey CCG priorities are:
1. Preventing people from being admitted to
the Trust.
Primary care hub appointments available 7
days a week and blocked appointments held
specifically for patients being redirected form the
acute Trust.
Additional winter resilience funding for additional staff
to support admission avoidance activity.
A senior CCG nurse has
been based in the Trust four days a week since
September 2017 to support the discharge work.
2. Moving patients out of the hospital as soon as
they are well enough to be discharged.
Haringey and Enfield have
increased the number of patients going through our
Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
6 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
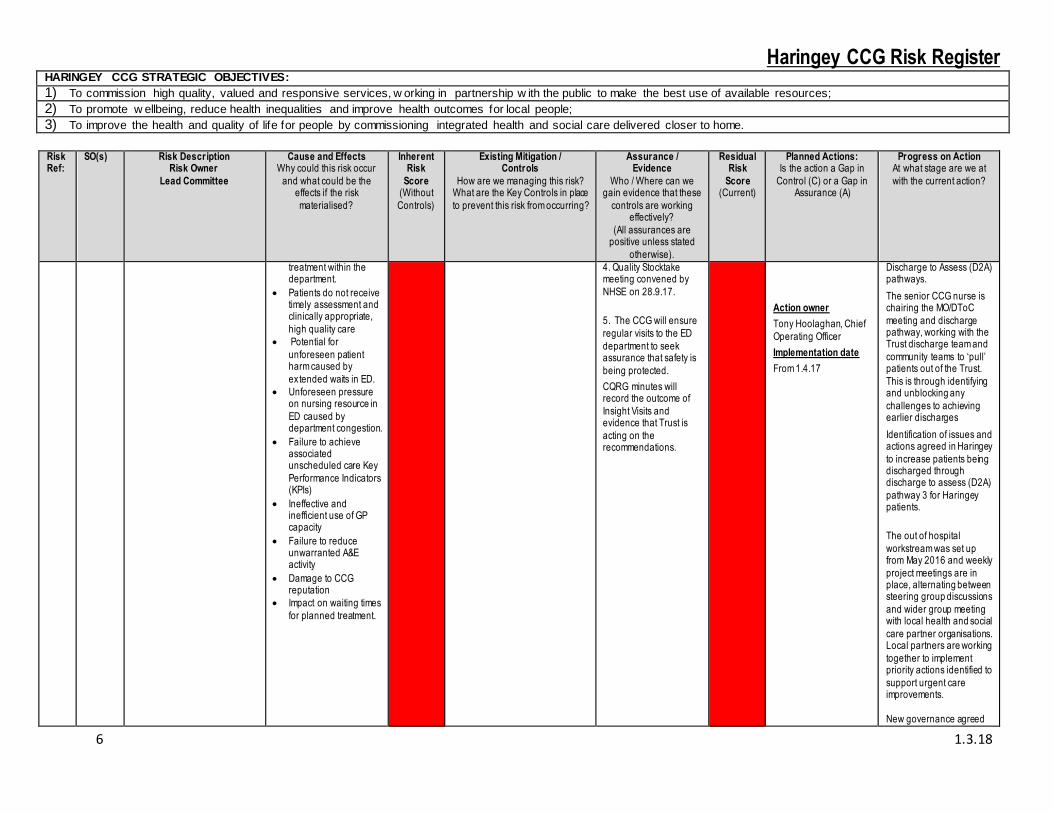
treatment within the department.
Patients do not receive timely assessment and clinically appropriate,
high quality care
Potential for
unforeseen patient harm caused by
extended waits in ED.
Unforeseen pressure on nursing resource in
ED caused by department congestion.
Failure to achieve associated unscheduled care Key
Performance Indicators (KPIs)
Ineffective and inefficient use of GP capacity
Failure to reduce unwarranted A&E activity
Damage to CCG reputation
Impact on waiting times
for planned treatment.
4. Quality Stocktake meeting convened by
NHSE on 28.9.17.
5. The CCG will ensure
regular visits to the ED
department to seek assurance that safety is
being protected.
CQRG minutes will record the outcome of
Insight Visits and evidence that Trust is
acting on the recommendations.
Action owner
Tony Hoolaghan, Chief
Operating Officer
Implementation date
From 1.4.17
Discharge to Assess (D2A) pathways.
The senior CCG nurse is chairing the MO/DToC
meeting and discharge pathway, working with the Trust discharge team and
community teams to ‘pull’ patients out of the Trust.
This is through identifying and unblocking any
challenges to achieving earlier discharges
Identification of issues and actions agreed in Haringey
to increase patients being discharged through discharge to assess (D2A)
pathway 3 for Haringey patients.
The out of hospital
workstream was set up from May 2016 and weekly
project meetings are in place, alternating between steering group discussions
and wider group meeting with local health and social
care partner organisations. Local partners are working
together to implement priority actions identified to
support urgent care improvements.
New governance agreed

Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
7 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
3. The NCL Accountable Officer and Director of
Nursing and Quality to work with regulators and the Trust to ensure the
safety concerns which led to a quality stock take
meeting in September 2017 are addressed.
Action owner
Jennie Williams Director of Nursing and Quality
Implementation date
From 28.9.17
4. CCG to ensure that
quality and safety within A&E are being protected
during this period of
and implemented for the SFB programme in
2017/18, with oversight continuing to be part of the
A&E Delivery Board responsibilities.
This includes development
of a steering group where work stream leads from the
4 areas ensure the system is working together to
deliver key priorities.
3. There is a robust approach in place to
ensure improvements required by the GMC are evidenced, which includes
oversight by the CCG at a weekly meeting.
It is anticipated that a further quality stocktake
meeting will be convened in January 2018 to provide
the system with assurance that the broader quality issues have been
addressed.
4. The NMUH Medical Director provides a near-
time brief on the protection

Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
8 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
increased risk and enhanced surveillance.
Action owner
Jennie Williams Director
of Nursing and Quality
Implementation date
From February 2018
5. The CCG to ensure
that quality and safety within A&E are being protected during this
period of increased risk and enhanced
surveillance.
of quality and safety at every CQRG meeting.
The CCG undertook an assurance visit on 7.12.17
with NHS England and NHS Improvement to review progress with the
implementation of the quality and safety checklist.
The Emergency Care
Improvement Plan (ECIP) has reported that it
continues to support the Trust to embed the
checklist. The CCG Director of
Nursing and Quality and the Trust Medical Director
will work to develop an ED dashboard which the ED
team will embed. This will be used for
assurance at CQRG. The estimated time for
production of the dashboard is 6 weeks.
5. The Director of Nursing and Quality undertakes
regular visits to ED during the week and weekends.
The primary purpose is to ensure safety is being
protected and safe staffing is in place.

Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
9 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
Action owner
Jennie Williams Director of Nursing and Quality
Implementation date
From February 2018
The Chair of the CCG will undertake a visit to ED on
19.02.18 accompanied by the Assistant Direction of
Quality and Patient Safety.
26 1,2 There is a risk that BEHMHT will fail to deliver the required ‘must do’ and ‘should do’
improvements required, after the Trust was rated as ‘requires
improvement’ following an inspection by the CQC in
December 2015.
Risk Owner
Jennie Williams – Director of Nursing and Quality
Lead Committee
Quality Committee
Risk reworded in its current
form 15.6.15
Causes
Lack of capacity/ capability to deliver the required
improvements
The Trust is unable to make the
necessary improvements to
services provided out of the St Anne’s site
due to unsatisfactory environment.
Effect
There will be a further
deterioration in the quality and safety of services and
BEHMHT will be deemed not to meet regulatory
standards in respect of CQC outcomes.
I = 4
L = 4
16
1. The delivery of the BEHMHT CQC improvement action plan will
be overseen by the Clinical Quality Review Group (CQRG) bimonthly
from April 2017.
2. Haringey CCG will ensure the
CQC improvement plan gives appropriate focus to improved
outcomes for patients accessing services in Haringey.
3. Appropriate escalation to CCG
Quality Committee and Commissioning and Finance and
Performance meetings where funding issues impact on quality.
1. CQRG minutes will provide evidence of
review of the Trust’s quality and delivery plan
and the quality and safety dashboard, with
specific focus on safeguarding, patient
complaints and serious incidents.
2. The performance against key patient safety and experience metrics
for services delivered in Haringey will
demonstrate month on month improvements.
3. The CCG Quality Committee and Finance
and Performance Committee minutes
demonstrate escalation of concerns to
commissioning and finance colleagues where
I = 4
L = 3
12
Action
1. Commissioners to receive CQC improvement plan full
update 6-monthly at the CQRG meeting, with
bimonthly exception reporting of key risks and
remedial actions.
Action Owner
Jennie Williams, Director
of Nursing and Quality
Implementation date
By end of September
2016
1. In September 2017 the
CQC undertook a comprehensive inspection
of eight core mental health services and one
community service, with a return visit to inspect three
further areas.
On 12.1.18 the CQC published the inspection
report which gave the Trust an overall rating of
‘Requires Improvement’ with ‘Good ‘for caring,
responsive and well-led. The safe and effective
domains were rated as ‘Requires Improvement’
Immediately after the inspection in September
2017 the Trust was asked to take actions to address
issues relating to risk
Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
10 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
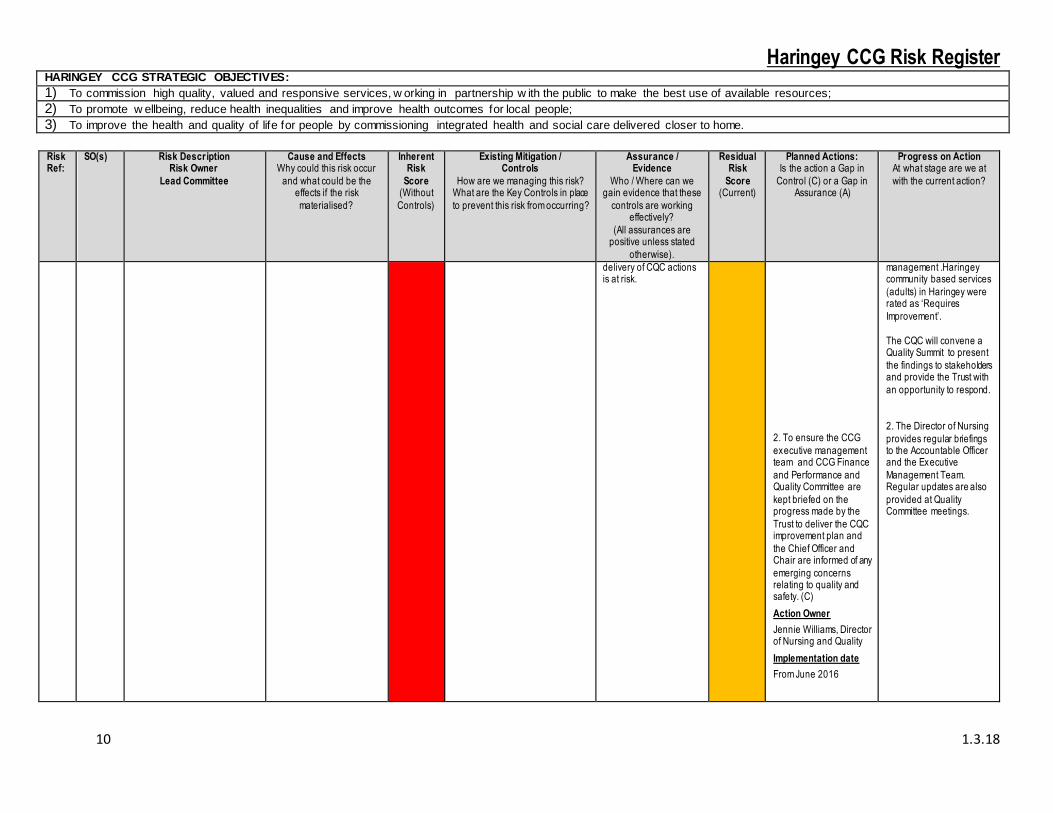
delivery of CQC actions is at risk.
2. To ensure the CCG
executive management team and CCG Finance
and Performance and Quality Committee are
kept briefed on the progress made by the
Trust to deliver the CQC improvement plan and
the Chief Officer and Chair are informed of any
emerging concerns relating to quality and safety. (C)
Action Owner
Jennie Williams, Director of Nursing and Quality
Implementation date
From June 2016
management .Haringey community based services
(adults) in Haringey were rated as ‘Requires
Improvement’.
The CQC will convene a Quality Summit to present
the findings to stakeholders and provide the Trust with
an opportunity to respond.
2. The Director of Nursing
provides regular briefings to the Accountable Officer and the Executive
Management Team. Regular updates are also
provided at Quality Committee meetings.

Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
11 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
38 1 There is a risk of failing to deliver a balanced Financial
Plan in 2017/18.
Risk Owner
Simon Goodwin – Chief Finance
Officer
Lead Committee
Finance and Performance
Committee
Risk added to Register
17.1.17
This risk has been CLOSED as
financial pressures in Acute and Continuing Care Services are
likely to result in the CCG not meeting the control total. The
CCG will work to mitigate pressures locally to achieve
financial balance across North Central London.
Causes
1 Significant level of QIPP
required in financial plan.
2 Work needed to implement STP
interventions.
3 Limited capacity in CCG budget to mitigate financial
issues in 2017/18.
4 Impact of HRG+4.
I = 5
L= 4
20
1. Appropriate financial
governance systems in place
2. Review and ongoing scrutiny of
the CCG’s financial performance
by Finance and Performance Committee and Governing Body.
3. Review and identification of 2017/18 QIPP Plan at QIPP
Delivery Group and Finance and Performance Committee meetings.
4. 2017/18 budget setting process.
5. Approval of Financial Plan by Finance and Performance Committee and Governing Body.
6. Pan-NCL work to implement and
deliver the STP interventions.
1. Internal Audit reports
produced by Internal Audit which cover
financial procedures within the CCG.
2. Papers and minutes of
Finance and Performance Committee
and CCG Governing Body.
3. Papers and minutes of QIPP Delivery Group and
Finance and Performance Committee.
4. Budget holders to sign off their 2017/18 budgets
by March 2017.
5. Financial Plan to be
reviewed regularly by the Finance and
Performance Committee, following approval by the
Finance and Performance Committee
and the Governing Body.
6. Discussion of NCL
financial position at Financial and Activity
Modelling Group.
I = 4
L= 4
16
1. Implement STP interventions. (C)
Action owner:
Simon Goodwin – Chief Finance Officer
Implementation date:
March 2017.
2. Identify additional QIPP projects, both CCG
and NCL-wide. (C)
Action owner:
Simon Goodwin – Chief
Finance Officer
Implementation date:
Ongoing 2017/18.
3. Discussions with NHS
England and NHS Improvement regarding
overall NCL financial gap. (C)
Action owner:
Simon Goodwin – Chief Finance Officer
Implementation date:
Ongoing 2017/18.
1. STP QIPP interventions currently being delivered
and developed in conjunction with providers.
Updated Project Initiation Documents being produced with
implementation and delivery timelines agreed
with CCG commissioners.
2. Work is continuing to identify additional QIPP.
3. Ongoing monthly calls held with NHSE to ensure
`CCG and NCL plans remain on target. Financial
Strategy being developed for NCL CCGs to allow
some future mitigation in the event plans do not balance.
The control totals are now managed collectively
across NCL CCGs. The expectation is that the
NCL-wide control total will be achieved.
Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
12 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
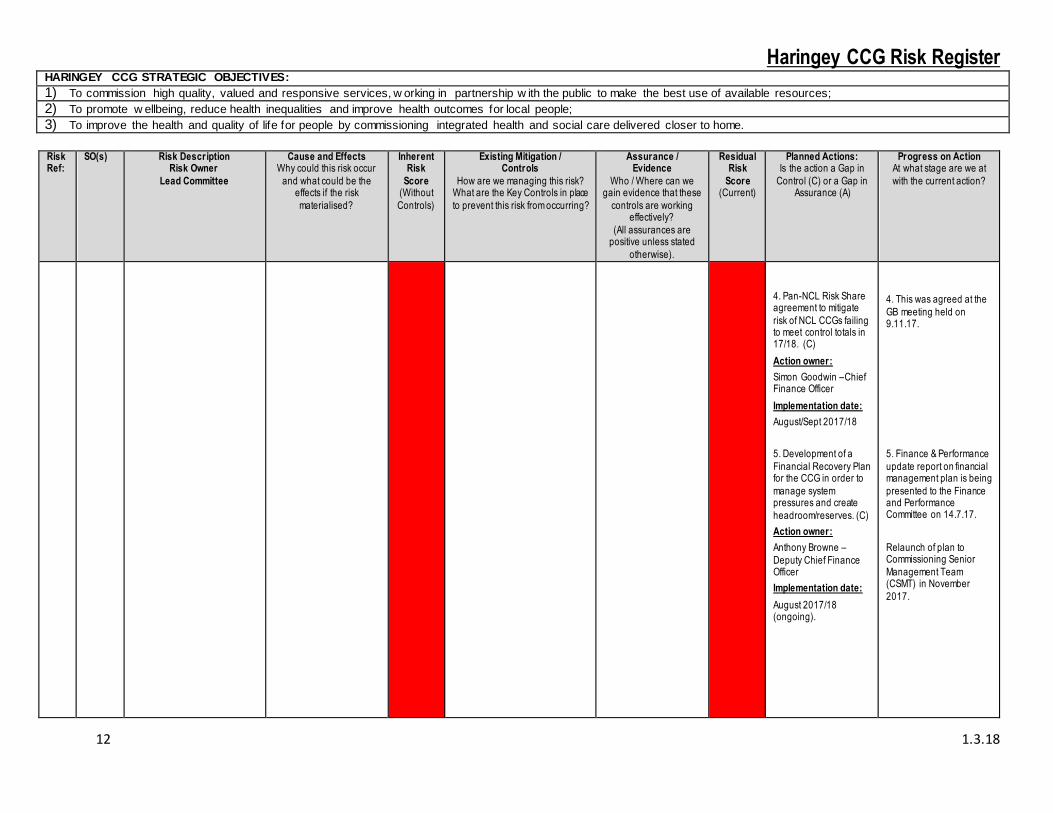
4. Pan-NCL Risk Share agreement to mitigate
risk of NCL CCGs failing to meet control totals in 17/18. (C)
Action owner:
Simon Goodwin –Chief Finance Officer
Implementation date:
August/Sept 2017/18
5. Development of a
Financial Recovery Plan for the CCG in order to
manage system pressures and create
headroom/reserves. (C)
Action owner:
Anthony Browne –
Deputy Chief Finance Officer
Implementation date:
August 2017/18 (ongoing).
4. This was agreed at the
GB meeting held on 9.11.17.
5. Finance & Performance
update report on financial management plan is being
presented to the Finance and Performance Committee on 14.7.17.
Relaunch of plan to Commissioning Senior
Management Team (CSMT) in November
2017.

Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
13 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
40 1,2, 3 There is a risk of quality and access to dermatology care
deteriorating as a result of cessation of North Middlesex
Hospital (NMUH) to provide dermatology from March 2018.
Risk Owner
Clare Henderson, Director of Commissioning, Haringey CCG
Lead Committee
Quality Committee and Finance and Performance Committee.
Risk added to register
22.9.17
Causes
Ongoing failure to recruit to Consultant
dermatology posts at NMUH, leading to non-
viability of this service continuing to be
provided by the Trust.
Effects
NMUH is unable to treat patients.
I – 4
L – 5
20
1. Establishment of joint task-and-finish group with NMUH to develop
and evaluate options.
2. Clinical partnership with Royal
Free Hospital (RFH) dermatology department is being explored
3. Performance is routinely monitored at Contract Review
Group meetings.
1. Updates at CQRG and Contract Review Group
2. Regular progress review through Task and Finish Group
3. Minutes of Contract Review Group meetings.
L – 4
I – 3
12
1. Director of
Commissioning to oversee development of
longer-term approach, including one which mitigates risks at RFH.
Action owner
Clare Henderson, Director of
Commissioning
Implementation date
July 2018
2. NMUH to subcontract
service to Concordia from 8.1.18 for 12 months.
Action owner
Clare Henderson, Director of
Commissioning
Implementation date
8.1.18
1. Commissioners are taking an options paper to
the Joint Commissioning Committee on 1.3.18.
Commissioners continue to
meet regularly to oversee progress and development
of future model
2. The Concordia service has now been commissioned and is
delivering services from NMUH.

Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
14 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
41 1 There is a risk of the financial position worsening before year
end 17/18.
Risk Owner
Simon Goodwin – Chief Finance
Officer
Lead Committee
Finance and Performance
Committee
Risk added to Register
19.2.18
Causes
1. Financial Pressures with
Acute Contracting, national pressures on Prescribing
stock availability and Continuing Health Care cost and volume pressures
2. Lack of CCG reserves /
contingency to stabilise financial position should
costs increase over contract value
3. Significant level of QIPP required in financial plan.
4. Impact of HRG+4 tariff increases and changes to
responsible commissioner identification rules.
I = 4
L= 3
12
1. Appropriate financial
governance systems in place
2. Review and ongoing scrutiny of
the CCG’s financial performance
by Finance and Performance Committee and Governing Body.
3. Review and identification of 2017/18 QIPP Plan at QIPP
Delivery Group and Finance and Performance Committee meetings.
4. Pan-NCL work to implement and deliver the STP interventions.
1. Internal Audit reports
produced by Internal Audit which cover
financial procedures within the CCG.
2. Papers and minutes of
Finance and Performance Committee
and CCG Governing Body.
3. Papers and minutes of QIPP Delivery Group and
Finance and Performance Committee.
4. Financial Plan to be reviewed regularly by the
Finance and Performance Committee,
following approval by the Finance and
Performance Committee and the Governing Body.
5. Discussion of NCL financial position at
Financial and Activity Modelling Group.
I = 3
L= 2
6
1. Financial Management Plan in place (C)
Action owner:
Anthony Browne – Deputy Chief Finance
Officer
Implementation date:
Ongoing 2017/18
2. Increased QIPP governance and
monitoring to identify and mitigate slippage, both
CCG and NCL-wide. (C)
Action owner:
Simon Goodwin – Chief Finance Officer
Implementation date:
Ongoing 2017/18.
3. Discussions with NHS
England and NHS Improvement regarding
overall NCL financial gap. (C)
Action owner:
Simon Goodwin – Chief Finance Officer
Implementation date:
Ongoing 2017/18.
1. F&P Committee approved Finance
Management Plan. Review of actions on a monthly
basis.
2. Senior level finance, executive and clinical
engagement through QIPP Leads meeting Work is
continuing to identify areas of slippage and begin
18/19 QIPP schemes in Q4 1718 where appropriate.
3. Ongoing monthly calls held with NHSE to assure
CCG and NCL plans. Control totals are now
managed collectively across NCL CCGs. The
expectation is that the NCL-wide control total will
be achieved.
Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
15 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
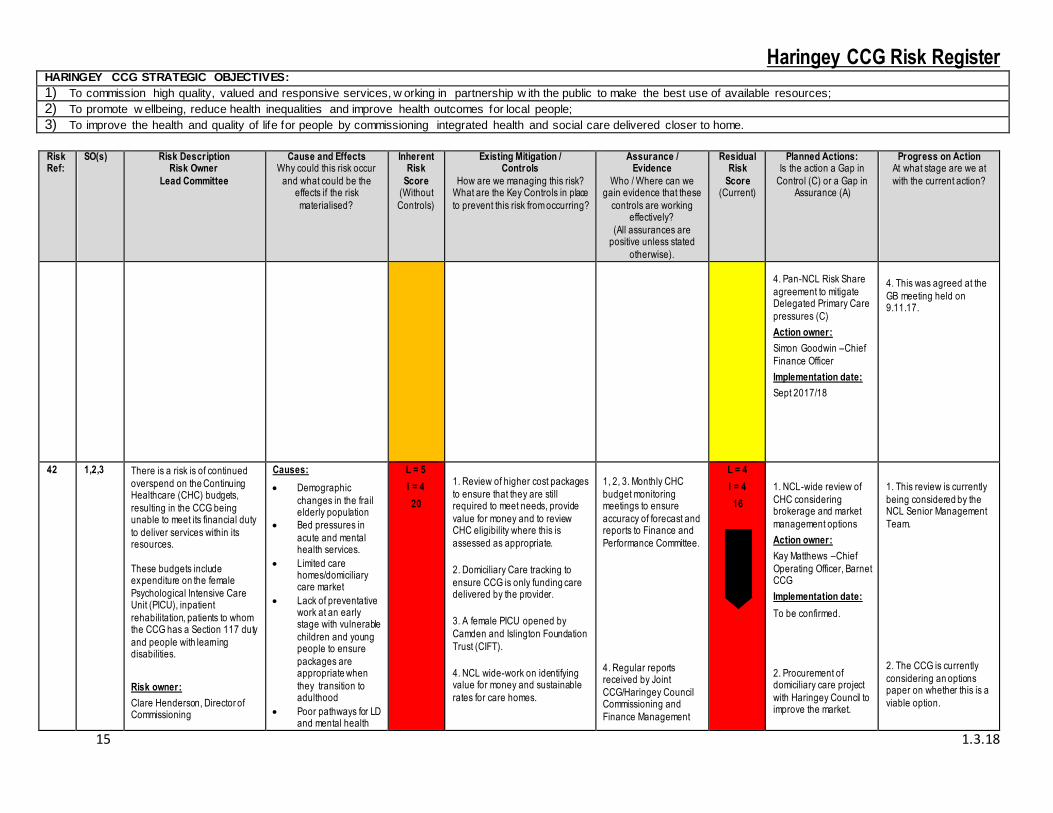
4. Pan-NCL Risk Share
agreement to mitigate Delegated Primary Care
pressures (C)
Action owner:
Simon Goodwin –Chief
Finance Officer
Implementation date:
Sept 2017/18
4. This was agreed at the
GB meeting held on 9.11.17.
42 1,2,3 There is a risk is of continued
overspend on the Continuing Healthcare (CHC) budgets,
resulting in the CCG being unable to meet its financial duty
to deliver services within its resources.
These budgets include expenditure on the female
Psychological Intensive Care Unit (PICU), inpatient
rehabilitation, patients to whom the CCG has a Section 117 duty
and people with learning disabilities.
Risk owner:
Clare Henderson, Director of Commissioning
Causes:
Demographic
changes in the frail elderly population
Bed pressures in
acute and mental health services.
Limited care homes/domiciliary care market
Lack of preventative work at an early stage with vulnerable
children and young people to ensure
packages are appropriate when
they transition to adulthood
Poor pathways for LD and mental health
L = 5
I = 4
20
1. Review of higher cost packages
to ensure that they are still required to meet needs, provide
value for money and to review CHC eligibility where this is
assessed as appropriate.
2. Domiciliary Care tracking to
ensure CCG is only funding care delivered by the provider.
3. A female PICU opened by
Camden and Islington Foundation
Trust (CIFT).
4. NCL wide-work on identifying value for money and sustainable
rates for care homes.
1, 2, 3. Monthly CHC
budget monitoring meetings to ensure
accuracy of forecast and reports to Finance and
Performance Committee.
4. Regular reports received by Joint
CCG/Haringey Council Commissioning and
Finance Management
L = 4
I = 4
16
1. NCL-wide review of
CHC considering brokerage and market
management options
Action owner:
Kay Matthews –Chief
Operating Officer, Barnet CCG
Implementation date:
To be confirmed.
2. Procurement of domiciliary care project
with Haringey Council to improve the market.
1. This review is currently
being considered by the NCL Senior Management
Team.
2. The CCG is currently
considering an options paper on whether this is a
viable option.

Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
16 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
Lead committee:
Finance and Performance
Committee
Risk added to register:
1.3.18
patients resulting in delays for patients in
services that are higher cost
Lack of reviews of CHC patients resulting in patients
who are not eligible remaining on CHC
Discharges from forensic units results in increased demand
Haringey Council also ensuring that
reviews are up to date and that clients
are given CHC eligibility where appropriate.
Effects
Continued increase
in CHC budget costs.
Lack of opportunities to invest in
developing improved pathways that will
result in reduced costs in the longer
term.
Group, and the Finance and Performance
Partnership Board.
Action owner:
Temmy Fasegha, - Vulnerable Adults
Commissioning Manager
Implementation date:
To be confirmed.
3. Review of budget
structure to bring mental health and learning
disabilities budgets under the responsibility of lead
commissioners to improve strategic
pathway development.
Action owners:
Shelley Shenker -
Assistant Director, Mental Health
Commissioning/ Temmy Fasegha, -
Vulnerable Adults Commissioning Manager
Implementation date:
To be confirmed.
4. Recruitment of 5 WTE clinical reviewers to clear
the backlog of 300 reviews.
3. Initial review meeting to
take place on 6.3.18, as part of a wider review of
the recovery plan.
4. Proposal to be
considered by Finance and Performance Committee
on 25.4.18.
Haringey CCG Risk Register HARINGEY CCG STRATEGIC OBJECTIVES:
1) To commission high quality, valued and responsive services, w orking in partnership w ith the public to make the best use of available resources; 2) To promote w ellbeing, reduce health inequalities and improve health outcomes for local people; 3) To improve the health and quality of life for people by commissioning integrated health and social care delivered closer to home.
17 1.3.18
Risk Ref:
SO(s) Risk Description Risk Owner
Lead Committee
Cause and Effects Why could this risk occur
and what could be the effects if the risk
materialised?
Inherent Risk
Score (Without
Controls)
Existing Mitigation / Controls
How are we managing this risk? What are the Key Controls in place
to prevent this risk from occurring?
Assurance / Evidence
Who / Where can we gain evidence that these
controls are working effectively?
(All assurances are positive unless stated
otherwise).
Residual Risk
Score (Current)
Planned Actions: Is the action a Gap in
Control (C) or a Gap in Assurance (A)
Progress on Action At what stage are we at
with the current action?
Action owner:
Temmy Fasegha, - Vulnerable Adults
Commissioning Manager
Implementation date:
April 2018.
5. Development of
commissioning plans to ensure the delivery of
interventions that are early as possible,
maximise independence and reduce delays in moving on to the next
appropriate provision.
Action owners:
Shelley Shenker - Assistant Director,
Mental Health Commissioning
Implementation date:
June 2018.
Top Related