






Languages
Pages
Legal


Frances Angelique A. Tequillo, MDCebu Doctors’ University
Staphylococci& Micrococci
Monday, June 27, 2011

The Staphylococci: An Overview
gram-positive spherical cells
arranged in grape-like irregular clusters
grow readily on many types of media
active metabolically
ferment carbohydrates
produce pigments from white to deep yellow
Monday, June 27, 2011

members of the normal flora of the skin & mucous membranes
may cause suppuration, abscess formation, and fatal septicemia
pathogenic types often hemolyze blood, coagulate plasma, & produce extracellular enzymes and toxins
rapidly develop resistance to antimicrobials
35 species
3 most important (clinically):
1.Staphylococcus aureus2.Staphylococcus epidermidis3.Staphylococcus saprophyticus
Monday, June 27, 2011

1. Coagulase positive Staphylococci
• S. aureus
2.Coagulase negative Staphylococci
• S. epidermidis
• S. saprophyticus
Grouping for Clinical Purposes
Monday, June 27, 2011
Staphylococcus aureus
major human pathogen
habitat: part of normal flora in humans and animals
usual site: skin, nasopharynx & perineum
can enter underlying tissue when there is a breach in mucosal barriers
forms characteristic abscesses
Monday, June 27, 2011

Diseases caused by S. aureus
due to direct effect of organism
local lesions of skin
deep abscesses
systemic infections
osteomyelitis, septic arthritis, infective endocarditis
toxin-mediated
food poisoning
toxic shock syndrome
scalded skin syndrome
Monday, June 27, 2011

Staphylococcus epidermidis
skin commensal
has predilection for plastic material
associated with infections of IV lines, prothetic heart valves, AV shunts
causes urinary tract infection in catheterized patients
Monday, June 27, 2011

Staphylococcus saprophyticus
skin commensal
important cause of urinary tract infection in sexually active young women
usually sensitive to a wide range of antibiotics
Monday, June 27, 2011

& IdentificationMorphology
Monday, June 27, 2011
Typical Organisms
spherical cells
about 1 um in diameter
arranged in irregular clusters
young cocci stain strongly Gm+
on aging, many cells become Gm-
nonmotile, non-sporeforming
Monday, June 27, 2011

grow readily on most media
under aerobic or microaerophilic conditions
grow most rapidly at 37C
form pigment best at room temperature (20-25C)
form round, smooth, raised, & glistening colonies on solid media
Culture
Monday, June 27, 2011
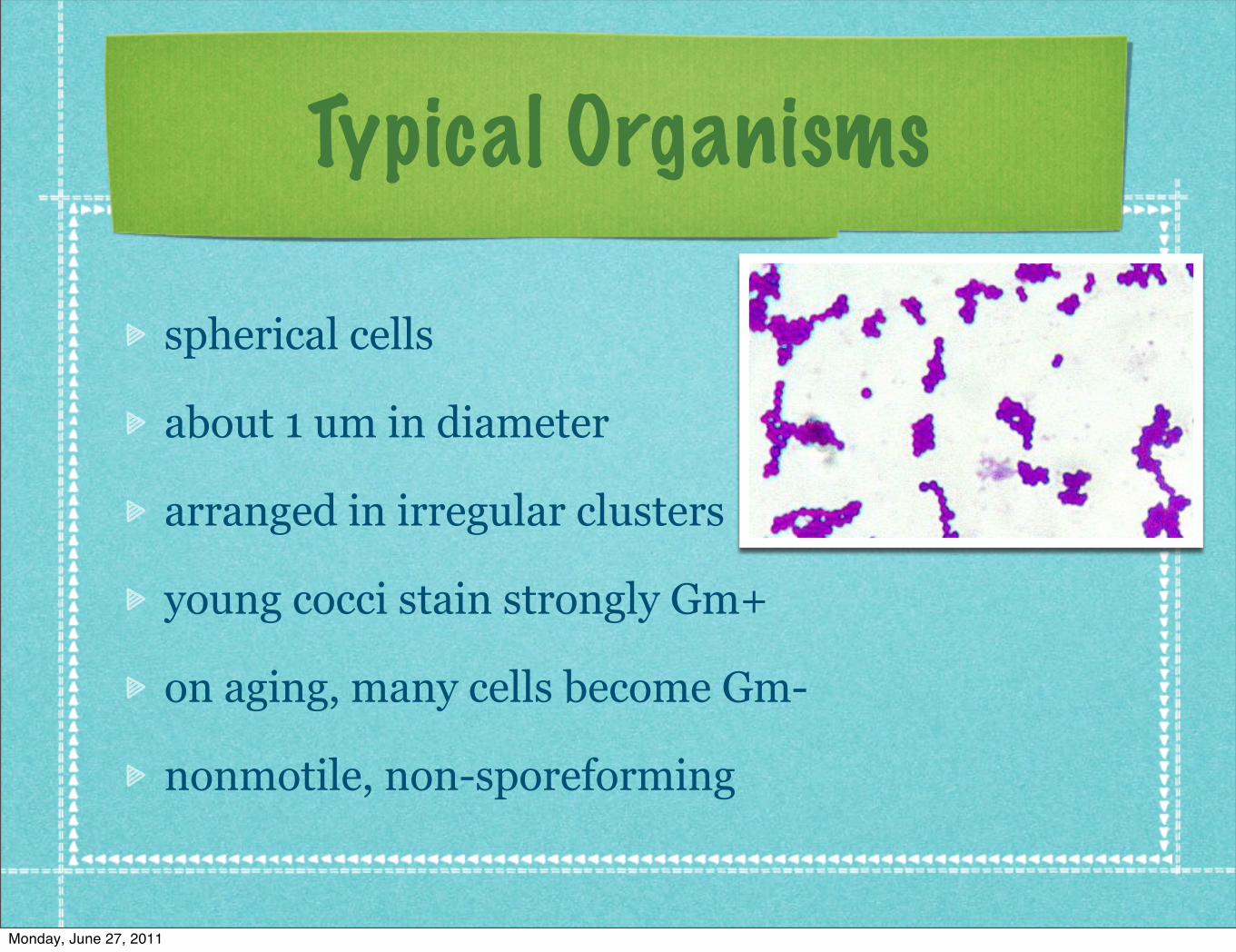
S. aureus form gray to deep golden yellow colonies
S. epidermidis form gray to white colonies
many colonies develop pigment only upon prolonged incubation
Peptostreptococcus sp. resemble staphylococci morphologically
S. aureus
S. epidermidis
Monday, June 27, 2011
produce catalase (unlike streptococci)
slowly ferment carbohydrates
producing lactic acid
resistant to drying, heat, and 9% NaCl
readily inhibited by some chemicals (3% hexachlorophene)
variably sensitive to many antimicrobials
Growth Characteristics
Monday, June 27, 2011

Resistance:
1. penicillins
2.nafcillin, methicillin, & oxacillin
3.vancomycin
4.tetracyclines, erythromycins, & aminoglycosides
Resistance
Monday, June 27, 2011

Variation
colony size, pigment, & hemolysis
enzyme elaboration
drug resistance
pathogenicity
Monday, June 27, 2011

Antigenic Structures
Monday, June 27, 2011

polysaccharide polymer w/c provides the rigid exoskeleton of the cell wall
destroyed by strong acid or exposure to lysozyme
elicits interleukin-1 production to cause fever and opsonic antibodies by monocytes
serves as chemoattractant for PMN leukocytes
have endotoxin-like activity
activates complement
Peptidoglycan
Monday, June 27, 2011

Teichoic acid
polymers of glycerol or ribitol phosphate
linked to the peptidoglycan layer
can be antigenic
antiteichoic acid antibodies detected in patients with active endocarditis (S. aureus)
Monday, June 27, 2011

Protein A
cell wall component of many S. aureus strains
binds to the Fc portion of IgG molecules, except IgG3
important reagent in immunology and diagnostic laboratory technology
protein A with attached IgG directed against a specific bacterial antigen will agglutinate bacteria that have that antigen (“coagglutination”)
Monday, June 27, 2011

other antigenic structures
capsules - inhibit phagocytosis by PMN leukocytes unless specific antibodies are present
coagulase (clumping factor) - binds nonezymatically to fibrinogen, leading to aggregation of bacteria
Monday, June 27, 2011

Enzymes & Toxins
Monday, June 27, 2011

Catalase
converts H2O2 into H2O and O2
catalase test differentiates staphylococci (+) from streptococci (-)
Monday, June 27, 2011

Coagulase & Clumping Factor
enzyme-like protein that clots oxalated or citrated plasma
binds to thrombin to initiate fibrin polymerization
deposits fibrin on the surface of bacteria and alters their ingestion by phagocytes
essential in invasive pathogenic potential
clumping factor: responsible for adherence of organisms to fibrinogen & fibrin
S. aureus tends to form clumps when mixed with plasma
Monday, June 27, 2011
Other Enzymes
hyaluronidase (spreading factor)
staphylokinase
proteinases
lipases
β-lactamase
Monday, June 27, 2011
Exotoxins
α-toxin: potent hemolysin
β-toxin: degrades sphingomyelin; toxic to many cells, including erythrocytes
δ-toxin: disrupts biologic membranes; plays a role in S. aureus diarrheal disease
γ-toxin: lyses white blood cells by causing pore formation in the cellular membranes that increase cation permeability
Monday, June 27, 2011

Leukocidin
S. aureus
has 2 components
act synergistically on the white blood cell membrane
important virulence factor in community associated methicillin resistant S. aureus infections
Monday, June 27, 2011

Exfoliative Toxins
epidermolytic toxins of S. aureus (superantigens)
toxin A: heat-stable (resists boiling for 20 mins)
toxin B: heat-labile
yield the generalized desquamation of the staphylococcal scalded skin syndrome by dissolving the mucopolysaccharide matrix of the epidermis
Monday, June 27, 2011

Toxic Shock Syndrome Toxin
TSST-1: produced by most strains of S. aureus isolated from patients with toxic shock syndrome; prototypical superantigen
binds to MHC class II molecules, stimulates T cells, leading to symptoms of TSS
fever, shock, multisystem involvement; desquamative rash
enterotoxin F
Monday, June 27, 2011

Enterotoxin
(A-E, G-I, K-M); superantigens
heat-stable and resistant to the action of gut enzymes
important cause of food poisoning
produced when S. aureus grows in carbohydrate and protein foods
ingestion of 25 μg of enterotoxin B leads to vomiting and diarrhea
emetic effect is due to CNS stimulation (vomiting center) after the toxin acts on neural receptors in the gut
Monday, June 27, 2011

Pathogenesis
Monday, June 27, 2011

members of the normal flora of human skin and respiratory & GI tracts
also found in clothing, bed linens & other fomites in human environments
pathogenicity is due to combined effect of extracellular factors and toxins together with the invasive properties of the strain
S. aureus (pathogenic, invasive) produce coagulase and forms a yellow pigment;hemolytic
S. epidermidis (nonpathogenic, non-invasive) are coagulase negative & non-hemolytic.
Monday, June 27, 2011

Pathology
Monday, June 27, 2011

prototype lesion: furuncle
S. aureus in hair follicles cause tissue necrosis
coagulase coagulates fibrin around the lesion & within the lymphatics
formation of a wall that limits the process, plus presence of inflammatory cells & fibrous tissue
liquefaction of necrotic tissue occurs at the center of the lesion
organisms may spread via lymphatics & bloodstream
Monday, June 27, 2011

Monday, June 27, 2011

Monday, June 27, 2011

Clinical Findings
Monday, June 27, 2011

localized infection appears as a “pimple”, hair follicle infection, or abscess
intense, localized, painful inflammatory reaction that undergoes central suppuration & heals quickly when the pus is drained
wall of fibrin & inflammatory cells around the core limits the spread of organisms
should not be broken down by manipulation or trauma
Monday, June 27, 2011

infection can result from direct contamination of a wound (e.g.) postoperative infections
secondary localization within or organ or system is accompanied by signs & symptoms of organ dysfunction and intense focal suppuration
food poisoning - violent nausea, vomiting & diarrhea; rapid convalescence; (-) fever
Monday, June 27, 2011

TSS - abrupt onset of high fever, vomiting, diarrhea, myalgia, scarlatiniform rash (erythematous skin rash which desquamates); hypotension with cardiac & renal failure (severe); can recur
seen in women who use tampons (5 days ff onset of menses)
also in men & children with staphylococcal wound infections
Monday, June 27, 2011

Monday, June 27, 2011

Staphylococcal Scalded Skin Syndrome
disease of young children
mediated through minor staphylococcal infection by “epidermolytic toxin”-producing strains
mild erythema and blistering of skin followed by shedding of sheets of epidermis
children are relatively healthy and most eventually recover
Monday, June 27, 2011

Diagnostic Laboratory Tests
Monday, June 27, 2011

Specimens
surface swab pus
blood
tracheal aspirate
spinal fluid for culture
depends on localization of the process
Monday, June 27, 2011

Smears
gram positive cocci in clusters in Gram-stained smears
(pus or sputum)
impossible to distinguish saprophytic from pathogenic staphylococci on smears
Monday, June 27, 2011

Smears
gram positive cocci in clusters in Gram-stained smears
(pus or sputum)
impossible to distinguish saprophytic from pathogenic staphylococci on smears
Monday, June 27, 2011
Culture
specimen placed on blood agar plates give rise to colonies in 18 hours at 37C
hemolysis & pigment color takes days (RT)
S. aureus ferments mannitol
Monday, June 27, 2011

Culture
specimen placed on blood agar plates give rise to colonies in 18 hours at 37C
hemolysis & pigment color takes days (RT)
S. aureus ferments mannitol
Monday, June 27, 2011

Catalase Test
used to detect presence of cytochrome oxidase enzymes
a drop of 3% H2O2 is placed on a slide + small amount of bacteria
presence of bubbles (release of O2) indicates a (+) test
Monday, June 27, 2011

Catalase Test
used to detect presence of cytochrome oxidase enzymes
a drop of 3% H2O2 is placed on a slide + small amount of bacteria
presence of bubbles (release of O2) indicates a (+) test
Monday, June 27, 2011

Coagulase Test
Citrated rabbit (or human) plasma diluted 1:5 is mixed with broth culture / growth
incubated at 37C
clot formation in 1-4 hours is (+)
indicates pathogenicity in humans
Monday, June 27, 2011

Coagulase Test
Citrated rabbit (or human) plasma diluted 1:5 is mixed with broth culture / growth
incubated at 37C
clot formation in 1-4 hours is (+)
indicates pathogenicity in humans
Monday, June 27, 2011

Susceptibility Testing
broth microdilution or disk diffusion
should be done routinely for isolates of clinically significant lesions
resistance to penicillin G can be predicted by a (+) test for β-lactamase (produced by 90%)
resistance to nafcillin (& oxacillin & methicillin) occurs in 35% of S. aureus & 75% of S. epidermidis isolates
Monday, June 27, 2011

Monday, June 27, 2011

Monday, June 27, 2011

Serologic & Typing Tests
little practical value
molecular typing techniques used to document spread of epidemic disease-producing clones of S. aureus
pulsed-field gel electrophoresis & multilocus sequence typing are highly discriminatory
Monday, June 27, 2011
Clues
in all pus-forming lesions
Gram stain and culture of pus
in all systemic infections
blood culture
in infections of other tissues
culture of relevant tissue or exudate
Monday, June 27, 2011

Treatment
Monday, June 27, 2011

tetracyclines - used for long term treatment of multiple skin infections (acne, furunculosis)
drainage - for abscess & other closed suppurating lesions; + antimicrobial therapy
Penicillin G - drug of choice for non-β-lactamase producing S. aureus
Vancomycin - for nafcillin-resistant staphylococci (eg S. epidermidis infection in patients with prosthetic devices)
Monday, June 27, 2011

Monday, June 27, 2011

Monday, June 27, 2011

Monday, June 27, 2011

Monday, June 27, 2011

Epidemiology & Control
Monday, June 27, 2011

chief sources of infection: shedding human lesionsfomites contaminated from shed lesionsrespiratory tractskin
cleanliness, hygiene & aseptic management can control spread of lesionsin hospitals: NICU, ICU, OR, and cancer chemotherapy units are at highest risk for severe staphylococcal infectionsrecent development: dissemination of CA-MRSA
Monday, June 27, 2011
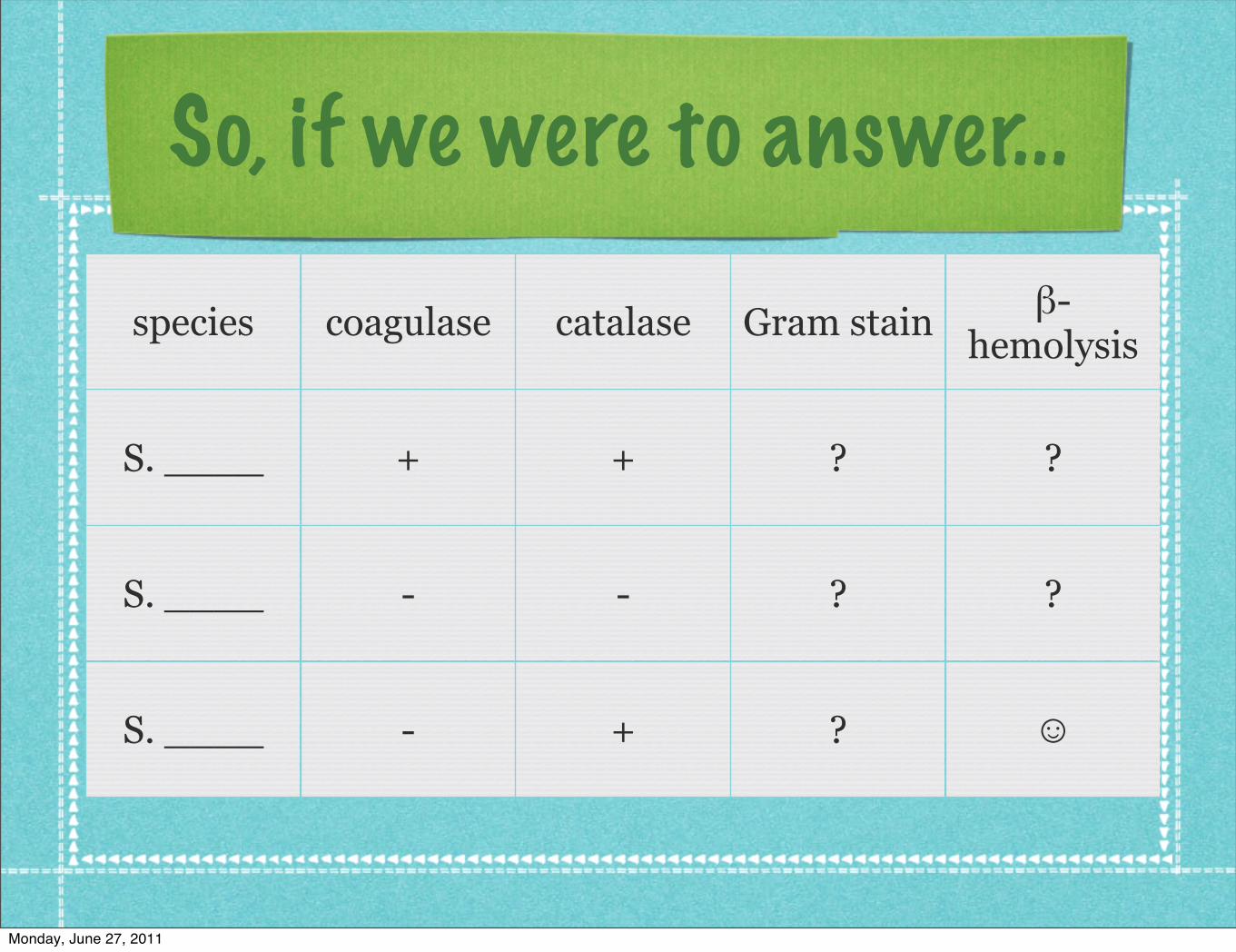
So, if we were to answer...
species coagulase catalase Gram stain β-hemolysis
S. ____ + + ? ?
S. ____ - - ? ?
S. ____ - + ? ☺
Monday, June 27, 2011

The Micrococci
Monday, June 27, 2011

comprise the normal flora of the upper layers of the epidermis & hair follicles (w/ S. epidermidis)
Gram+ spherical cells that appear in tetrads
cell wall comprises ~50% of cell mass
rich in guanine & cytosine (GC)
M. luteus, M. roseus
produce yellow & pink colonies when grown on mannitol salt agar
Monday, June 27, 2011

thought to be saprophytic or commensal organisms
may be opportunistic pathogens, esp. in immunocompromised hosts
pulmonary infections (in immunocompromised), recurrent bacteremia, septic shock, septic arthritis, endocarditis, meningitis
difficult to identify as cause of infection
part of normal skin flora
not usually identified with disease
Monday, June 27, 2011

M. lutea
Monday, June 27, 2011
Monday, June 27, 2011

“Blessed is the man who, having nothing to say,abstains from giving us wordy evidence of the fact.”
GEORGE ELIOT, Impressions of Theophrastus Such
Monday, June 27, 2011
Top Related