






Languages
Pages
Legal


DATA LINKAGEIntroduction to Design and Planning
Longitudinal Studies
Andrew P Costa, PhDAssociate Professor | Schlegel Chair in Clinical Epidemiology & Aging | https://hei.mcmaster.ca/ Research Director | St. Joseph’s Healthcare Centre for Integrated CareResearch Director | Michael G. DeGroote School of Medicine, Waterloo Regional CampusAssociate Scientific Director | CLSA https://www.clsa-elcv.ca/ Adjuct Scientist | IC/ES McMaster https://www.ices.on.ca@Andrew_P_Costa
CIHR SPA 20211

Participants aged 45 to 85
at baseline (51,338)
Active follow-up every 3 years
CLSA Research Platform
20152010 - 2015
TIME
20 Years
2018
Baseline FU-1 FU-2 FU-3 FU-4 FU-5 FU-6
50,000 women and men aged 45 - 85 at baseline
Target: 20,000Actual: 21,241
Randomly selected withinprovinces
Target: 30,000 Actual: 30,097
Randomly selected within 25-50 km of 11 sites
Questionnaire• By telephone (CATI)
Questionnaire• In person, in home (CAPI)
Clinical/physical testsBlood, urine
• @ Data Collection Site
2033
Participant Recruitment
VancouverVictoriaSurrey Calgary Winnipeg
Hamilton
Ottawa
MontrealSherbrooke
Halifax
St. John’s
Comprehensiven=30,000
Trackingn=20,000

Depth and Breadth of CLSAPHYSICAL & COGNITIVE MEASUREMENTS§ Height & weight § Waist and hip measurements§ Blood Pressure, Pulse Rate§ Grip strength, timed up-and-go, chair raise, 4-m walk
Standing balance, ADL/IADL, Functional measures§ Vision (retinal imaging, Tonometer & visual acuity)§ Hearing (audiometer)§ Spirometry§ Body composition (DEXA) & Bone density (DEXA)§ Aortic calcification (DEXA)§ ECG, Carotid Plaque sweep (ultrasound), Carotid intima-media thickness (ultrasound)§ Cognitive assessment (30 min battery
HEALTH INFORMATION§ Chronic disease symptoms (18 disease algorithm)§ Medication and supplements intake § Women’s health§ Self-reported health service use § Oral health§ Preventative health§End of Life Questionnaire
PSYCHOSOCIAL§ Social participation§ Social networks and support§ Caregiving and care receiving§ Mood, psychological distress, §PTSD§ Coping, adaptation§ Injuries and consumer products§ Work-to-retirement transitions§ Retirement planning§ Social inequalities§ Mobility-lifespace, Transportation§ Air Pollution & Built environments §Income, Wealth and Assets
LIFESTYLE & SOCIODEMOGRAPHIC§ Smoking§ Alcohol consumption§ Physical activity (PASE)§ Nutrition (nutritional risk and food frequency)§ Birth location§ Ethnicity/race/gender§ Marital status§ Education§Age, Sex, Gender Identity, housing
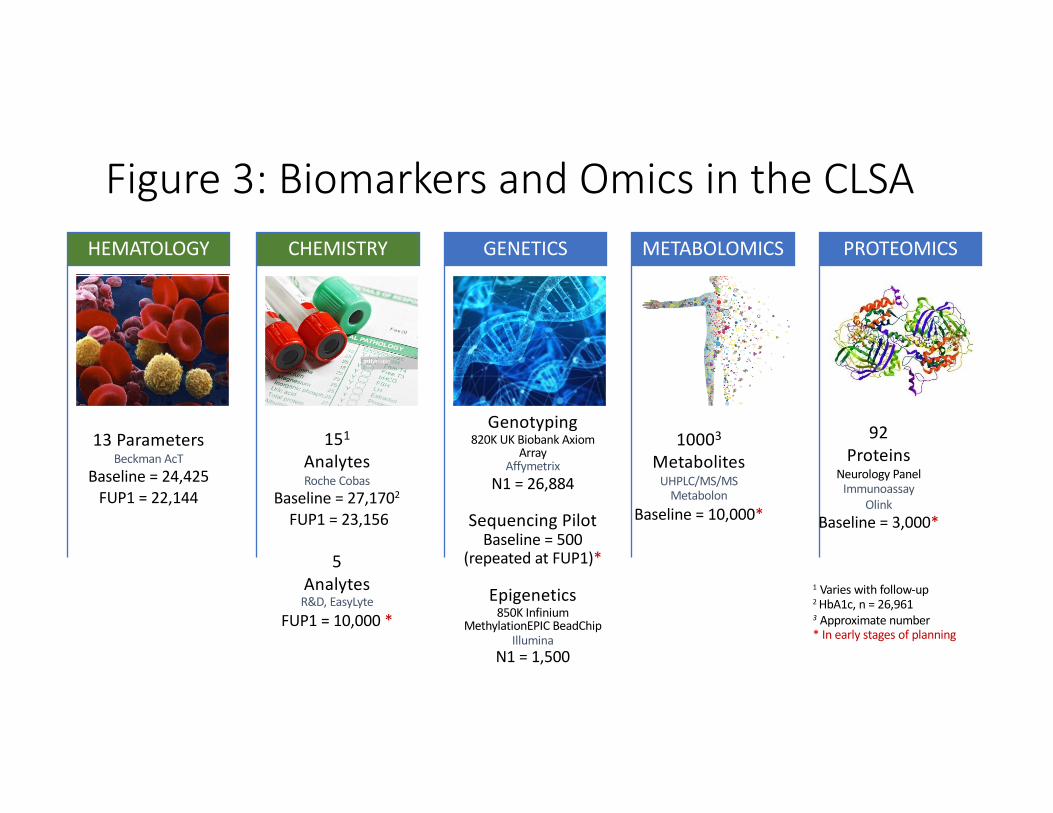
HEMATOLOGY CHEMISTRY
Genotyping
820K UK Biobank Axiom
Array
Affymetrix
N1 = 26,884
Sequencing Pilot
Baseline = 500
(repeated at FUP1)*
Epigenetics
850K Infinium
MethylationEPIC BeadChip
Illumina
N1 = 1,500
GENETICS METABOLOMICS PROTEOMICS
Figure 3: Biomarkers and Omics in the CLSA
151
Analytes
Roche Cobas
Baseline = 27,1702
FUP1 = 23,156
5
Analytes
R&D, EasyLyte
FUP1 = 10,000 *
13 Parameters
Beckman AcT
Baseline = 24,425
FUP1 = 22,144
92
Proteins
Neurology Panel
Immunoassay
Olink
Baseline = 3,000*
10003
Metabolites
UHPLC/MS/MS
Metabolon
Baseline = 10,000*
1Varies with follow-up
2 HbA1c, n = 26,961
3Approximate number
* In early stages of planning
5
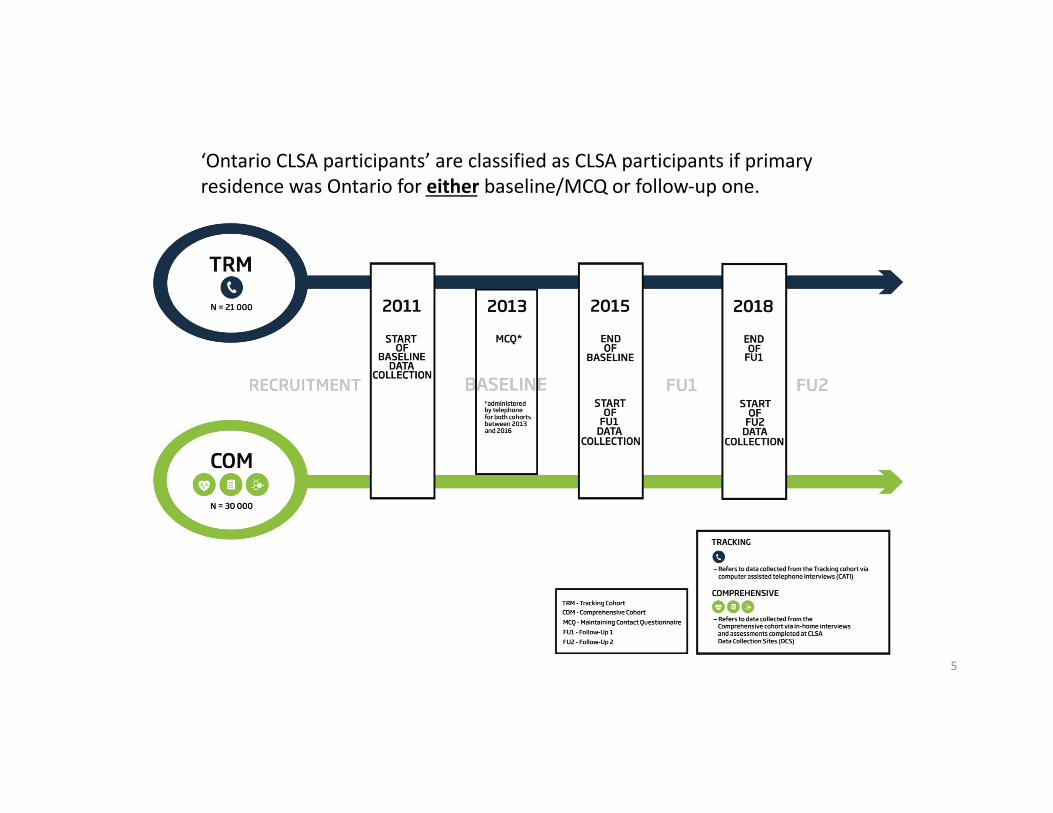
‘Ontario CLSA participants’ are classified as CLSA participants if primary residence was Ontario for either baseline/MCQ or follow-up one.
What is the future of data linkage in longitudinal cohorts?
• Linking CLSA data with other secondary data sources:
• “Simple” – environmental data (e.g., CANUE)
• “Trickier” – provincial health service and clinical data (e.g, IC/ES, Pop. Data B.C.”)
• “Complicated” – wearable technologies, geospatial data, consumer and social e
• Combined data may give new insights
6

Linkage with Contextual and Environmental Data: Collaboration with The Canadian Urban Environment
Health Research Consortium (CANUE)
Air Quality Nighttime Light Greenness
Weather & ClimateCan-ALE DataSocial & Material Deprivation Indices
What is the future of data linkage in longitudinal cohorts?
• Linking CLSA data with other secondary data sources:
• “Simple” – environmental data (e.g., CANUE)
• “Trickier” – provincial health service and clinical data (e.g, IC/ES, Pop. Data B.C.”)
• “Complicated” – wearable technologies, geospatial data, consumer and social e
• Combined data may give new insights
8

‘Atypical’ / Emerging Sources
9
‘Big Data’An incredible amount of data is collected every day in our health system as really, a byproduct, of all of the activity that happens in health care
These data can be harnessed to help us understand needs and help us make decisions about their care.
We can use these huge sources of data to evaluate health in real-world settings.
Progress on BarriersCapture and storage
Cost, cost-effectiveness
Transfer/Sharing, Information privacyStandards, liability
Analysis, visualization, queryData >> information (artificial intelligence)

Administrative health records, clinical registries, vital statistics, ethno-cultural identifiers, social services, corrections, education, transport data, etc. – all linked at the level of the individual
Example: Data held by IC/ES (Ontario)• Registered Persons Database (RPDB)
• Hospital Discharge Abstract Database (DAD)
• National Ambulatory Care Reporting System (NACRS)
• Continuing Care Reporting System (CCRS)
• Home Care Reporting System (HCRS) + HCD
• National Rehabilitation Reporting System (NRS)
• Ontario Mental Health Reporting System (OMHRS)
• Ontario Health Insurance Plan Claims Database (OHIP)
• Ontario Drug Benefit Claims (ODB)
• Ontario Cancer Registry (OCR)
• Derived Diagnostic Cohorts (CHF, HIV, COPD, Dementia, etc.)
• Ontario Marginalization Index (ON-Marg)
13

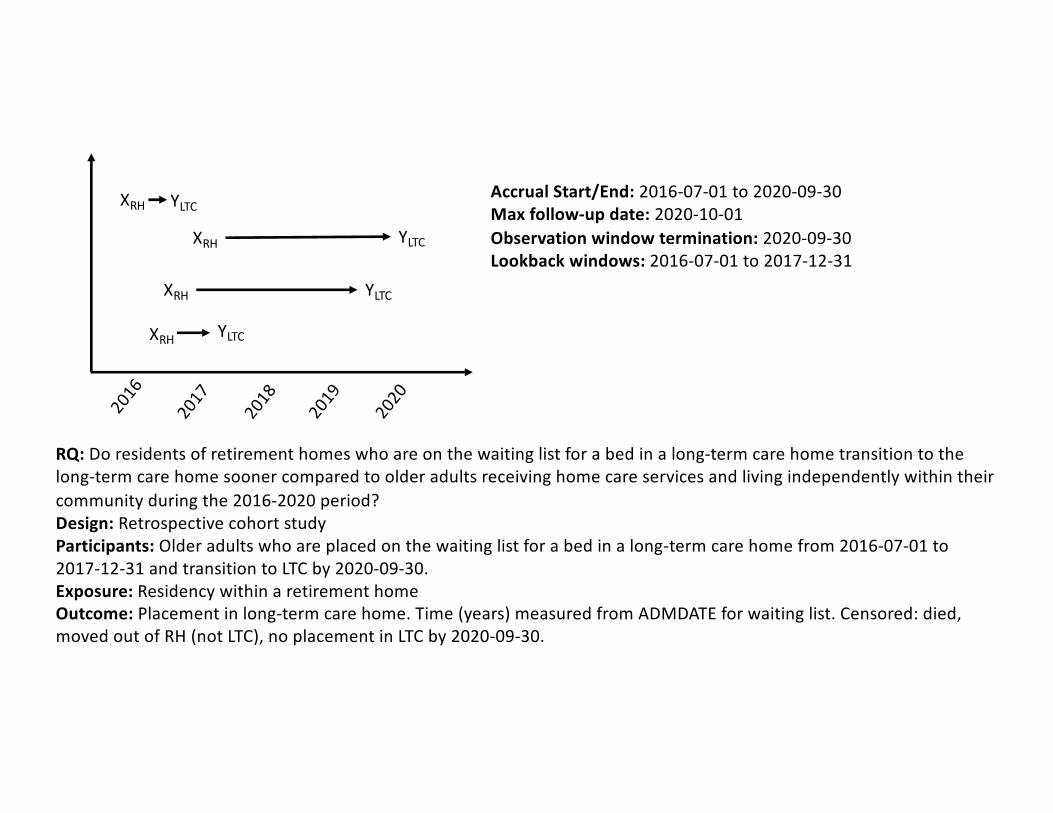
Sankey Diagram Illustrating Life Trajectories Among Residents of Retirement Homes, 2016 to 2019
2016
2017
2018
2019
2020
XRH
XRH
XRH
XRH
YLTC
YLTC
YLTC
YLTC
Accrual Start/End: 2016-07-01 to 2020-09-30Max follow-up date: 2020-10-01Observation window termination: 2020-09-30Lookback windows: 2016-07-01 to 2017-12-31
RQ: Do residents of retirement homes who are on the waiting list for a bed in a long-term care home transition to the long-term care home sooner compared to older adults receiving home care services and living independently within their community during the 2016-2020 period?Design: Retrospective cohort studyParticipants: Older adults who are placed on the waiting list for a bed in a long-term care home from 2016-07-01 to 2017-12-31 and transition to LTC by 2020-09-30. Exposure: Residency within a retirement homeOutcome: Placement in long-term care home. Time (years) measured from ADMDATE for waiting list. Censored: died, moved out of RH (not LTC), no placement in LTC by 2020-09-30.

Some secondary data can define phenotypes
16

The balance….
Longitudinal Cohorts
• Representative
• Comprehensive data
• Recall and drop out
• Standardized data
Derived Cohorts Data from Secondary Data• Census level
• Opportunistic data points
• Complete follow-up
• Often lack of meaningful standardization

No one organization has “all the data”
• Data environment is complex and complementary
• HDRN Canada is developing the Canada HDR Alliance to enable research access to data that accommodates this complexity
• The Canadian Longitudinal Study on Aging (CLSA) is a pilot member of the HDR Alliance
• Health Data Research Network Canada (HDRN Canada) has a mandate to expand
available data – with our member organizations holding foundational population-based
data
18
CLSA Data Linkage• The Canadian Longitudinal Study on Aging (CLSA)
recently joined the Alliance. CLSA is a large, national, longitudinal research study of adult development and aging.
• Collaborative activities with CLSA:• Facilitating the linkage between the CLSA data sets and
HDRN data centres, and streamlining requests to access linked data through DASH
• Co-developing data access and methodological resources that are consistent across provincial and territorial data centres
• Exploring a number of scientific opportunities to demonstrate impact of data linkage
19
The possibilities ..
• 94% of participant provided consent to linkage.
• This provided researchers with unique data not available in current provincial data platforms to do:• Cross-sectional linkage• Longitudinal health service cohort• Measure validation, include disease algorithms.
• The partnership expands the access and relevance of CLSA’s detailed longitudinal data to the Canadian researcher interested in health services and policy questions that will allow ‘cell to health system’ research across jurisdictions

Capacity Building Questions
• The saturation of the CLSA cohort in specific administrative data sets currently, and in the future.• The utility of various administrative data sets to define key health
service variables for the CLSA cohort.• The utility of CLSA cohort data to validate administrative data fields
and to act as a detailed base-cohort of older adults. • The utility of cross-walking CLSA data to administrative data sets that
can provide updated information between follow-ups or upon transition to institutional settings.
21

CLSA is funded by the Government of Canada through CIHR and CFI, and provincial governments and universities
Contact:Data inquiries: [email protected] inquiries: [email protected]
Top Related