







Languages
Pages
Legal


Greg Atkinson and Alan M Batterham
Health And Social Care Institute
Teesside [email protected]
SIZE MATTERS:HOW A STATISTICIAN CAN HELP
ENDOTHELIAL FUNCTION RESEARCH

• Brachial FMD% is NOT “closely related” to coronary vasodilation, especially in CHD patients (r = 0.26) – Besides correlation is not the same as individual prediction error
which is what matters in the clinic• Brachial FMD% is NOT deemed suitable for assessing CHD risk in
asymptomatic people– (by the AHA - even without considering the issues raised here)
• FMD% does NOT indicate “function” per se– Baseline artery size is easier to measure so relative importance of
size and “function” must be untangled• Many claims about magnitude of changes/differences in FMD% ARE
biased without allometric adjustment– Bias is usually that the differences/changes are larger than reality
• Other errors include shear rate normalisation and repeatability claims
This presentation is about statistics. But statistics are part of scientific inference, so mistakes are being made

Endothelialdysfunction
Endothelial dysfunction – a precursor to atherosclerosis?

BASELINEFMD
The flow-mediated dilation (FMD) protocol - all about physiology
Dpeak
Dbase
Thanks to Helen Jones for these photos

The resulting measurements

The final step: Calculation of the FMD% index (all about statistics)
FMD% = (Dpeak-Dbase) x 100 Dbase
= 5.0 – 4.0 x 100
4.0
= 25%
Where “D” is diameter of artery
FMD
FMD
FMD 4 mm

The final step: Calculation of the FMD% index (all about statistics)
FMD% = (Dpeak-Dbase) x 100 Dbase
= 7.5 – 6.0 x 100
6.0
= 25%
Where “D” is diameter of artery
FMD
FMD
FMD 6 mmChange MUST be proportional to Dbase for FMD% to work, but is this true? We’ll check
later

Publications on FMD% far outstrip its use in the clinic or public health for risk appraisal, i.e. it’s “impact” in
UK REF terms
Source: Scopus
Celermajer et al. Lancet 1992

2013 - Atkinson, G., Batterham, A.M., Thijssen, D.H.J., Green, D.J. A new approach to improve the specificity of flow-mediated dilation for indicating endothelial function in cardiovascular research. Journal of Hypertension, 31: 287-291. Cited 67 times.
2013 - Atkinson, G., Batterham, A.M. Allometric scaling of diameter change in the original flow-mediated dilation protocol. Atherosclerosis, 226: 425-427. Cited 52 times.
2011 - Thijssen, D.H.J., Black, M.A., Pyke, K.E., Padilla, J., Atkinson, G., Harris, R.A., Parker, B., Widlansky, M.E., Tschakovsky, M.E., Green, D.J. Assessment of flow-mediated dilation in humans: A methodological and physiological guideline. American Journal of Physiology - Heart and Circulatory Physiology, 300: H2-H12. Cited >400 times.
But it’s great if you want citations

FMD% seems prognostic for future CHD in some studies (returned to later)
Yeboah et al. Circulation 2007;115:2390
FMD%<Median
But on the balance of evidence, the AHA do not recommend FMD% for risk appraisal in asymptomatic people (even without the extra issues raised here). So minimal impact potential in UK REF terms. Key statistic AUC which is rarely reported.

Percentage flow-mediated dilation
Time to translate the evidence into clinical
practice? No – Time to scrutinise the evidence. No point
just having a research tool if the research has no
impact

r2 = 62%
Celermajer et al. Lancet 1992; 340: 1111–1115.
Dbase-dependencyA problem
right from the start
“For arteries of diameter less than 6.0 mm, flow-mediated dilation is about 10% in control subjects; however for arteries of more than 6.0mmin diameter, flow-mediated dilation is small even in healthy subjects. . . .our method is best applied to the study of smaller arteries in adults (such as the brachial or internal carotid) and larger arteries in children”
(Celermajer et al.,1992)
Some convoluted solutions to the Dbase problem
“Reporting absolute change in diameter will minimize this [the Dbase-dependency] problem … percent change might be the easiest method to use if baseline diameter remains stable over time. However, the best policy may be to measure and report baseline diameter, absolute change and percent change in diameter.”
(Correttti et al., 2002)
“Objective comparison of %FMD is only possible between patients with the same brachial artery size.”
(Milia-Stelic et al., 2007)
“Shear rate normalisation is essential for examining endothelial-dependent flow-mediated dilation between groups differing in baseline arteries”.
(Pyke et al., 2004)
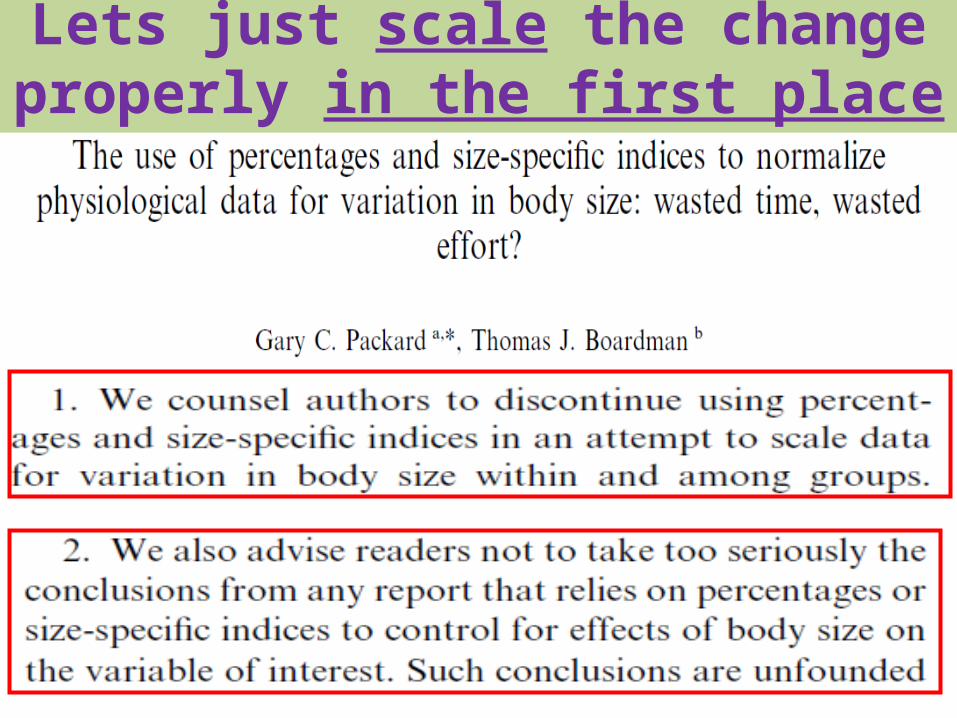
Lets just scale the change properly in the first place

15
Many allometric relationships have been established between body size and organ weight as well as body
size and physiological process
Allometry – the study of size and its consequences

The allometric relationship between Dbase and Dpeak?
FMD% = (Dpeak-Dbase) x 100 Dbase
= Dpeak
Dbase
= Dpeak . Dbase-1
Where “D” is diameter of artery
FMD
FMD
FMD
AllometricExponent

One way to derive the allometric exponent (log – log model)Ln
(Pea
k D
iam
eter
)
Ln (Baseline Diameter)
Atkinson and Batterham, Atherosclerosis 2013; 226:425-427
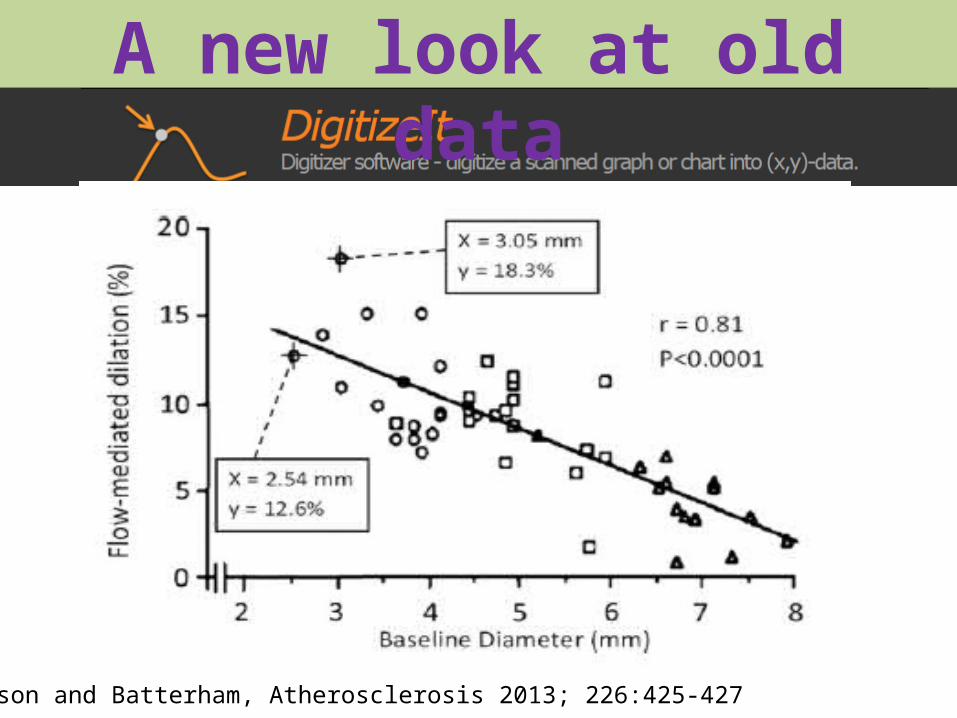
A new look at old data

Extracted data using DigitizeIt

Absolute flow-mediated response is actually inversely proportional to Dbase!
Atkinson and Batterham, Atherosclerosis 2013; 226:425-427

Flow-mediated response is inversely proportional to Dbase
Data re-analysed from Pyke et al. J Appl Physiol 2004; 97: 499-508.
This is the same data that wasused to conclude shear rate
normalisation is necessary. When scaled properly, the Dbase
problem goes away anyway.

Study name Population Artery Sample size Statistics for each study Point estimate and 95% CI
Point Lower Upper estimate limit limit
Atkinson et al., 2013 Young adults and children Brachial 64.000 0.890 0.845 0.935
Atkinson and Batterham 2013a Yound adults Femoral 14.000 0.860 0.765 0.955
Atkinson and Batterham 2013b Children Femoral 16.000 0.930 0.845 1.015
Atkinson and Batterham 2014 Adults (>45 years) Brachial 3499.000 0.940 0.935 0.945
Atkinson, In Press Adults Brachial 44.000 0.820 0.780 0.860
0.937 0.932 0.942
-1.00 -0.50 0.00 0.50 1.00
Favours A Favours B
Meta Analysis
Allometric exponents for various FMD datasets

Comparison of models for Celermajer et al. 1992
FMD% vs Allometry
Reanalysed data from Celermajer et al., 1992Atkinson and Batterham, Atherosclerosis 2013; 226:425-427
FMD% is leading us down false
trails

Some more examples

Children vs Adults (again)
Atkinson et al. J Hypertens 2013;31:287-291.
So FMD% is NOT better in children, so is it really an early
indicator of atherosclerosis? Yet another paradox?
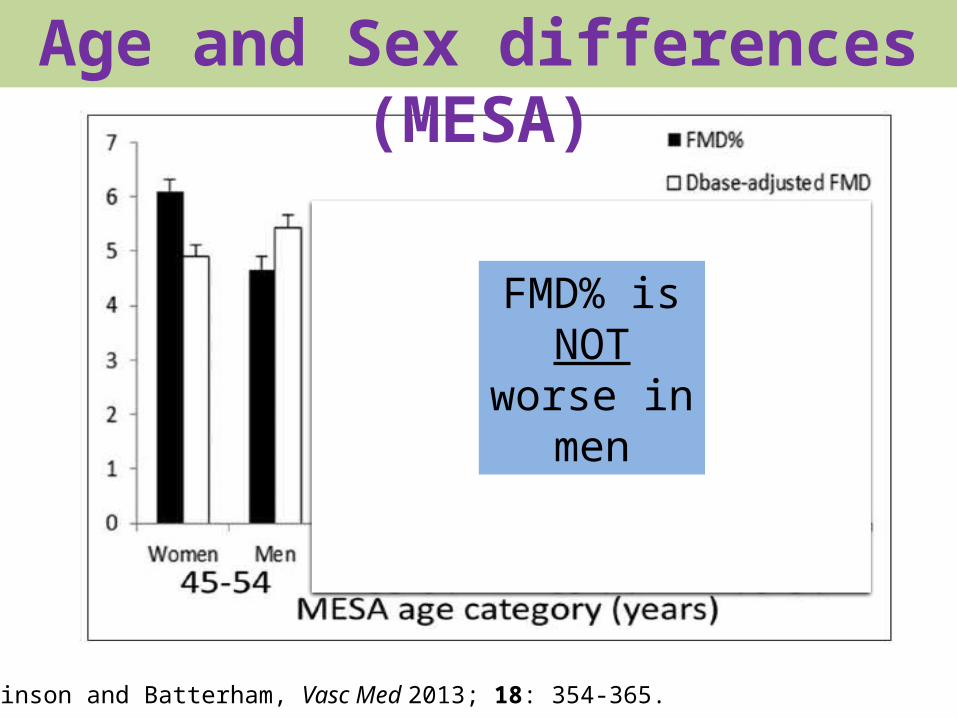
Age and Sex differences (MESA)
Atkinson and Batterham, Vasc Med 2013; 18: 354-365.
FMD% is NOT
worse in men
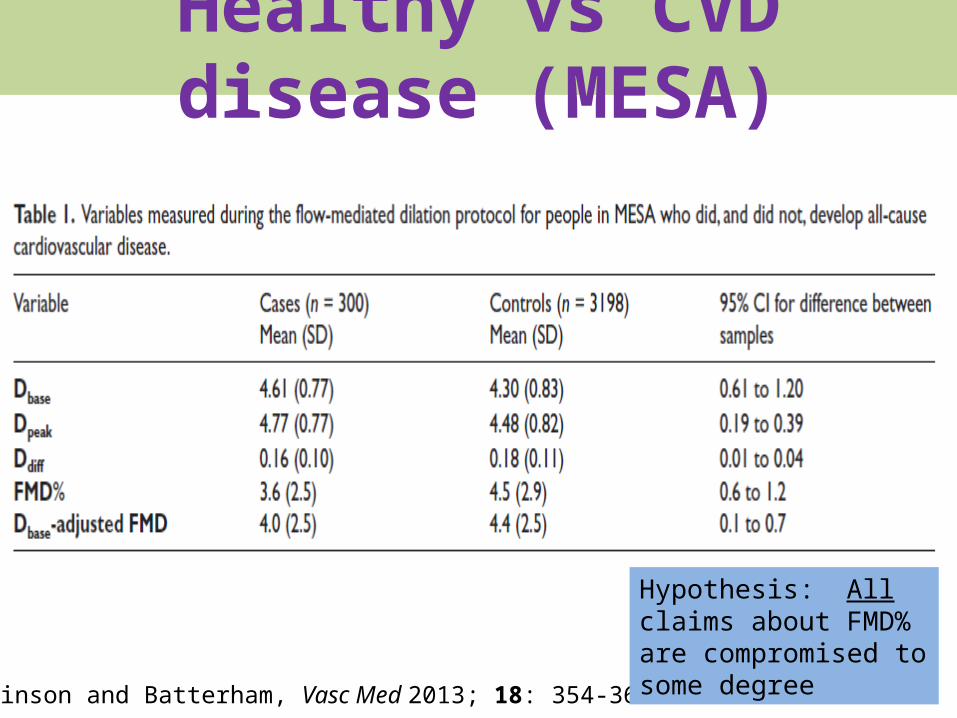
Healthy vs CVD disease (MESA)
Atkinson and Batterham, Vasc Med 2013; 18: 354-365.
Hypothesis: All claims about FMD% are compromised to some degree

Two fundamental and oft-cited claims
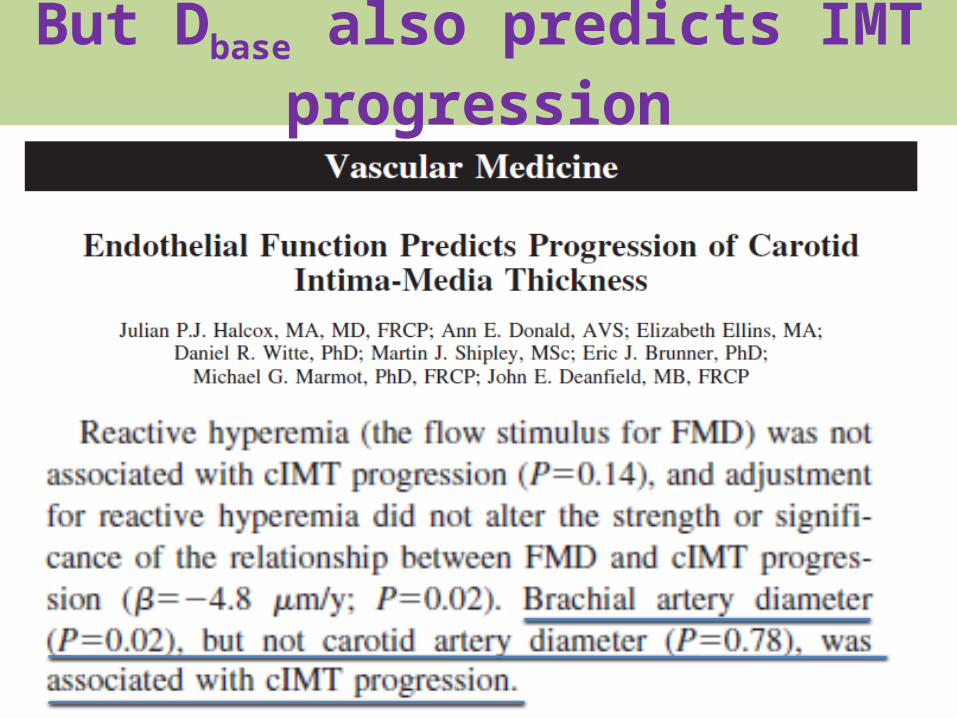
But Dbase also predicts IMT progression

Is the brachial-coronary vasodilation correlation really “close”? No – especially in the CHD patients that were
studied – time to stop regurgitating this in the literature?
r = 0.36

Dbase itself is also prognostic
Yeboah et al. Circulation 2007;115:2390
Low FMD%
FMD%<Median
High Dbase
Dbase>Median
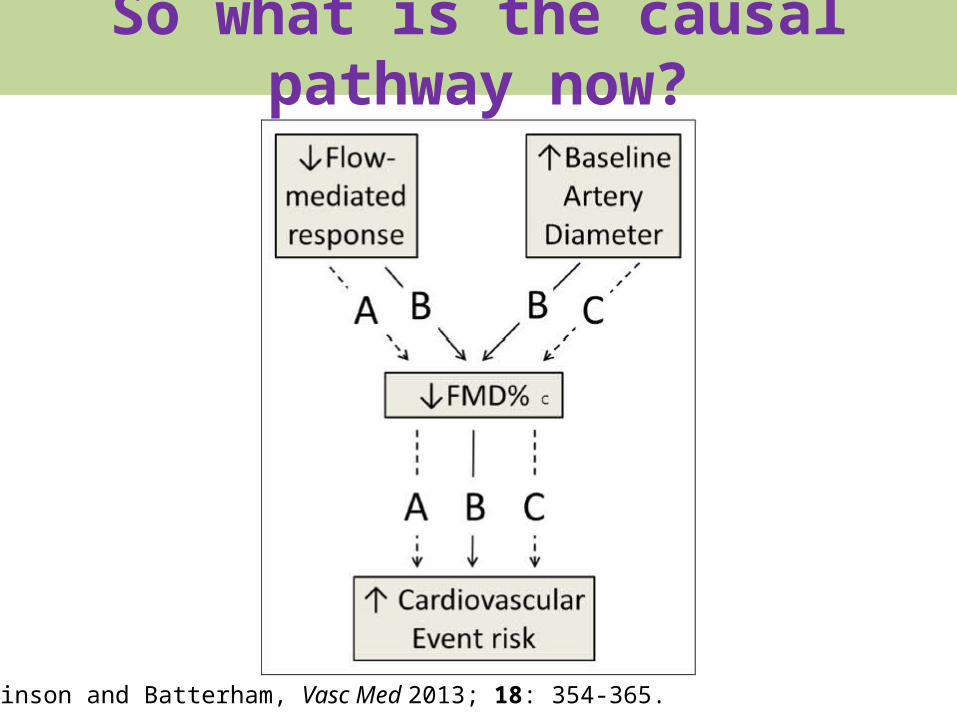
So what is the causal pathway now?
Atkinson and Batterham, Vasc Med 2013; 18: 354-365.

Conclusions (1)FMD%:• Is a ratio (honestly – some referees argued not!)• Misrepresents the apparent inverse relationship
between flow-mediated response and artery size• Is dependent on Dbase for purely statistical reasons• Can be a biased index of the flow-mediated D change• Can cloud the causal pathway between flow-mediated
response per se and cardiovascular disease• Is not adequately repeatable (but Dbase is) and is not
recommended by AHA for appraising risk of CHD in asymptomatic people

Conclusions (2)Allometric scaling:• Removes the dependency on artery size in all datasets
if done properly• Isolates the flow-mediated response per se• Makes any other approaches to remove Dbase-
dependency redundant, including shear rate normalisation
• Quantifies differences in the flow-mediated response precisely
• Clarifies the causal pathway• Is bad news for some

ReferencesATKINSON, G. & BATTERHAM, A. M. 2013. Allometric scaling of diameter change in the original flow-mediated dilation protocol. Atherosclerosis, 226, 425-427.ATKINSON, G. & BATTERHAM, A. M. 2013. The percentage flow-mediated dilation index: A large-sample investigation of its appropriateness, potential for bias and causal nexus in vascular medicine. Vascular Medicine (United Kingdom), 18, 354-365.ATKINSON, G. 2013. The dependence of FMD% on baseline diameter: A problem solved by allometric scaling. Clinical Science, 125, 53-54.ATKINSON, G. 2013. Impaired endothelial function in obstructive sleep apnoea: Allometric scaling can help estimate the true difference in flow-mediated response. Heart, 99, 968-969.ATKINSON, G. 2014. The difference in the flow-mediated response between steroid users and non-users. European Journal of Preventive Cardiology, 21, 339.ATKINSON, G. 2014. Shear rate normalization is not essential for removing the dependency of flow-mediated dilation on baseline artery diameter: Past research revisited. Physiological Measurement, 35, 1825-1835.ATKINSON, G. & BATTERHAM, A. M. 2012. The use of ratios and percentage changes in sports medicine: Time for a rethink? International Journal of Sports Medicine, 33, 505-506.ATKINSON, G. & BATTERHAM, A. M. 2013. Response to "Adjusting for brachial artery diameter in the analysis of flow-mediated dilatation: Pitfalls of a landmark paper?". Atherosclerosis, 228, 282-283.ATKINSON, G. & BATTERHAM, A. M. 2014. Response to: 'Allometric scaling of endothelium-dependent vasodilation: Brachial artery flow-mediated dilation coming of age'. Vascular Medicine (United Kingdom), 19, 142-143.ATKINSON, G. & BATTERHAM, A. M. 2014. When will the most important confounder of percentage flow-mediated dilation be reported and adjusted for at the study level? International Journal of Cardiology, 172, 261-262.ATKINSON, G. & BATTERHAM, A. M. 2015. The Clinical Relevance of the Percentage Flow-Mediated Dilation Index. Current Hypertension Reports, 17.ATKINSON, G., BATTERHAM, A. M., THIJSSEN, D. H. & GREEN, D. J. 2013. Reply to Stoner et al. regarding 'A new approach to improve the specificity of flow-mediated dilation for indicating endothelial function in cardiovascular research'. Journal of Hypertension, 31, 1058.ATKINSON, G., BATTERHAM, A. M., THIJSSEN, D. H. J. & GREEN, D. J. 2013. A new approach to improve the specificity of flow-mediated dilation for indicating endothelial function in cardiovascular research. Journal of Hypertension, 31, 287-291.ATKINSON, G., THOMPSON, A. & BATTERHAM, A. M. 2014. Baseline artery diameter: The hidden confounder in research syntheses on human endothelial function? Heart Lung and Circulation, 23, 98-99.
Top Related