





Languages
Pages
Legal


Sinclair & Green (2005) BMJ
I used to just get stressed out and think ‘”right hit the bottle”. I’d hit the bottle, get all depressed, at first I’d feel more relaxed…..then I’d end up like a volcano. I’d explode and either go and hit out at somebody or hit back on myself because I can’t cope with this and that’s when I’d hit myself hard’

Imperial College London: Mike Crawford, Emese Csipke
CNWL NHS Foundation Trust: Adrian Brown, Steve Reid
Imperial College Healthcare Trust: Julian Redhead, Robin Touquet
SHARPAn exploratory randomised trial of
brief intervention for alcohol misuse following deliberate self harm

Alcohol and completed suicide Alcoholism is one of the best predictors of suicide
following DSH (Beck 1989)
Suicide rate in those who misuse alcohol is 8 times that of general population (Foster et al. 1997)
Strong population level associations between alcohol consumption and suicide rates (Wasserman 2001)
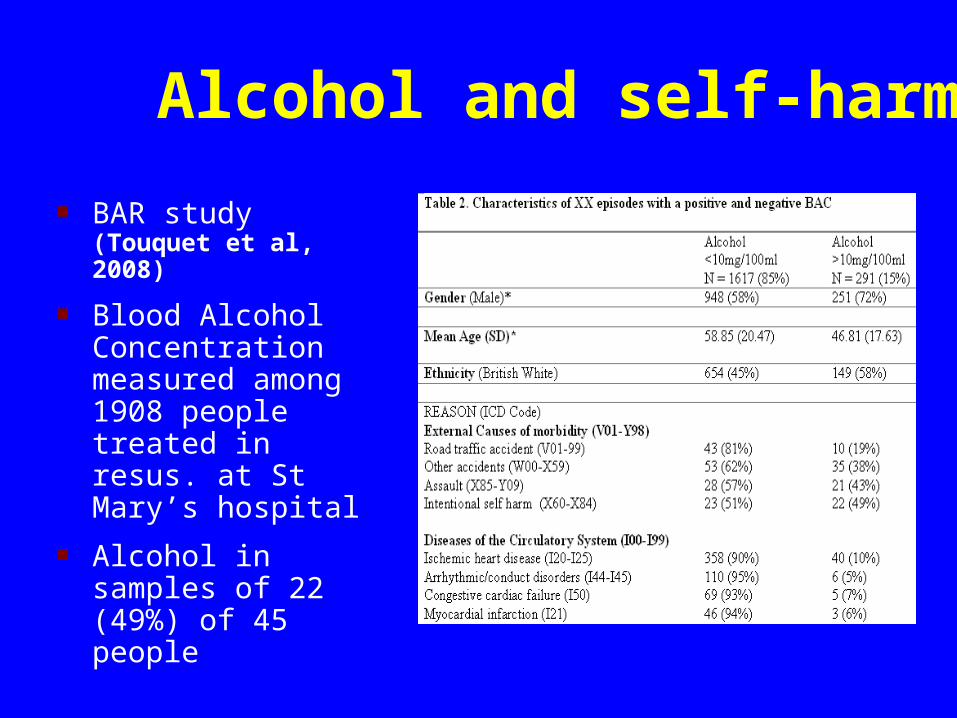
Alcohol and self-harm
BAR study (Touquet et al, 2008)
Blood Alcohol Concentration measured among 1908 people treated in resus. at St Mary’s hospital
Alcohol in samples of 22 (49%) of 45 people

Alcohol and self-harm
BAR study (Touquet et al, 2008)
Blood Alcohol Concentration measured among 1908 people treated in resus. at St Mary’s hospital
Alcohol in samples of 22 (49%) of 45 people

SBI and behavioural change Research conducted across a wide range of contexts
has demonstrated that SBI leads to medium term reductions in alcohol consumption (Moyer et al. 2001; Kaner et al. 2007)
This outcome may not be valued by clinicians REDUCE project: Decrease in 7 units of alcohol per
drinking session AND reattendance at Emergency Departments (Crawford et al 2004)
Evidence from clinical trials and systematic reviews has shown that SBI leads to reductions in accidents and injuries of between 30 and 70% (Gentilello et al. 1999, Dinh-Zarr et al. 2004)

SHARP Self Harm Alcohol Reduction Programme Does brief intervention for alcohol misuse among people
who present to emergency medical services following deliberate self harm reduce the likelihood of repetition?
To compare levels of reattendance to ED following self harm over six months among those who receive a self help leaflet with those who receive a leaflet plus an appointment for brief intervention from an Alcohol Nurse Specialist.
Feasibility – recruitment rate and explore effect size

Study sample ED at St Mary’s Paddington Inclusion criteria: Misusing
alcohol according to Paddington Alcohol Test (PAT)
Aged over 18
Address in greater London
Able to provide verbal consent to follow up (language and level of consciousness)
Excluding: those already in contact with alcohol services, those who make a specific request to do so

Paddington alcohol test

Study methods Pre-prepared sealed opaque envelopes containing either:
Experimental treatment (ET) - A card with details of appointment with Alcohol Nurse Specialist (ANS) together with a leaflet with information on drinking and healthControl treatment (CT) - A blank piece of card and a leaflet
Baseline demographic and PAT details. Follow-up at 3 and 6 months
Primary: reattendance at ED with DSH from records Secondary: episodes of DSH. Alcohol consumption using AUDIT. General mental health – using the 12-item GHQ. Satisfaction with care CSQ-3Covariate: extent of personality disturbance using SAP-AS (Moran et al, 2003)

Intervention• Referral for brief advice‘We believe that you are drinking alcohol at a level which may be harmful for your health, and would like to offer you an appointment with our Alcohol Nurse Specialist’
• ‘FRAMES’ approach and referral e.g. alcohol counselling, detoxification services etc.

Sample size and data analysis A sample of over 1,400 participants would be
required to have 80% power to detect a 30% reduction in the repetition of self harm using a 5% level of statistical significance.
Aimed to recruit at least 100 (over a two year period)
ANALYSIS:
Primary analysis conducted using an intention to treat principle. Differences in our primary outcome measure compared using chi-squared tests. Logistic regression analysis was then used to take account of any differences in potential confounding factors.

ResultsRecruitment:27 month period -November 2005 to January 2008.
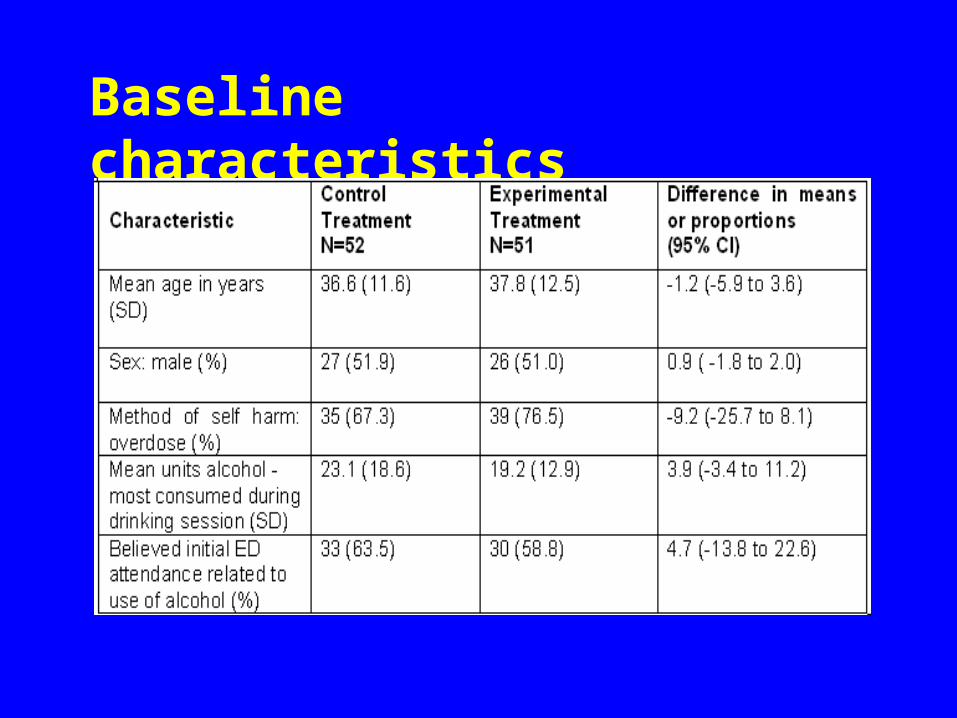
Baseline characteristics

Outcome data

Baseline alcohol consumption
Odds ratio for each unit increase in number of units drunk at baseline= 1.03 (95% CI = 1.00 to 1.06)

Adjusted Odds Ratios
Offer of brief intervention, adjusted for baseline alcohol consumption 1.00 (95% CI = 0.32 to 3.15)
Offer of brief intervention, adjusted all baseline variables 1.15 (95% CI = 0.34 to 3.97)
Twenty-four (47.1%) of the 51 randomised to experimental treatment received it. Odds of repetition of DSH among those attending an appointment 0.93 (95% CI = 0.27 to 3.14)
Trend towards reduced alcohol consumption among those referred for brief intervention persisted (B = -0.24, p = 0.06)
Discussion High level of alcohol misuse (56%)
Intervention acceptable: 47% attended appointment
Intervention probably associated with decreased alcohol use (7 units per drinking session)
BUT no difference in repetition of DSH or likelihood that alcohol was used in an episode of self harm (wide confidence limits)

Strengths and limitations Randomised Masked assessment of outcomes Feasible intervention
BUT Small size and low power Little baseline data Short follow-up period

Alcohol misuse and PD Data on SAP-AS from 75 (73%). 67 (89%) had
‘probable PD’. Concurrent alcohol misuse an indicator of PD among
people who self harm (45% Haw et al 2001 75% of those with comorbid alcohol misuse)
Lower levels of attendance at appointment with ANS
NICE guidelines (2009): brief interventions for people with borderline PD are not recommended
Complex interventions such as DBT associated with reduced levels of use of alcohol (Linehan et al. 1999)

Leadership
Teachable moment: when a link between alcohol consumption and health can be clearly seen
Timing: after dealing with the patient’s agenda.
Achieving behavioural change

Leadership
Teachable moment: when a link between alcohol consumption and health can be clearly seen
Timing: after dealing with the patient’s agenda.
When the relationship between alcohol use and health consequence is ‘accidental’ rather than ‘instrumental’
Achieving behavioural change
Leadership
Teachable moment: when a link between alcohol consumption and health can be clearly seen
Timing: after dealing with the patient’s agenda.
When the relationship between alcohol use and health consequence is ‘accidental’ rather than ‘instrumental’
‘when I feel I need to harm myself the first thing I do is pick up a drink’
Achieving behavioural change
Top Related