






Languages
Pages
Legal


I-MELT, 11-13 December 2017
1
ScaffoldingClinicalReasoningandDecisionMaking:ClinicalHandover
KatiePiper1
1NursingandMidwifery,MonashUniversity
Correspondingauthoremailaddress:[email protected]
ApeerreviewedshortpaperforapresentationattheInternationalconferenceonModelsofEngaged
LearningandTeaching(I-MELT)inAdelaide,11-13December2017.Availablefromwww.imelt.edu.au
Abstract
Clinicalhandoverisadangeroustimeforpatients.Poorcommunicationduringhandoveriswidelythoughtto
contributetopoorerpatientoutcomes.InAustralia,toolssuchasISBARhavebeenintroducedinanattempt
toprovideasharedframeworkandconsistenthandoverformat.DespitetheintroductionofISBAR,errorsare
still a prevalent issue. This paper introduces a potential solution. The Research Skills Development (RSD)
frameworkwasusedasatoolforfinalyearnursingstudentstoapplyclinicaljudgementandcriticalthinking
during handover. Identifying handover as an active process will stimulate the provision of rationales for
patientmanagement,andearlierrecognitionofclinicaldeterioration.
Background
Clinical handover presents a high risk for patient safety, with potentially life-threatening consequences
(Mannix, Parry&Roderick, 2017).Handover is definedas the transferofprofessional accountability and
responsibility of care (Australian Commission onQuality and Safety inHealthcare [ACSQHC] 2010). Poor
communication during this transaction can result in adverse events, including ineffective or wrong
treatments(Mannixetal.,2017)andprolongedhospitaladmission(Spooner,Chaboyer,Corley,Hammond,
&Fraser,2013).Thescaleofthisproblemislarge,withmillionsofhandoverepisodesoccurringannuallyin
the Australian healthcare system (ACSQHC, 2011). In Australia, ISBAR (Identify, Situation, Background,
Assessment andRecommendation) is a tool used to facilitate the safe transfer of patient information in
handover.ISBARassistswithorganisingthetransferofpatientinformationintoalogicalformattoreduce
theomissionofimportantinformationandtofacilitateconsistencyintheprocess.

I-MELT, 11-13 December 2017
2
Handovershouldnotbelimitedtothetransmissionofinformation;itisanopportunitytodevelopashared
understandingofpatients(Rixon,Braaf,Williams,Liew&Manias,2017).Thebenefitsofnursesquestioning
duringhandoverincludethedetectionofincorrectassessmentsandactions(Rayoetal,2014).Researchby
Drach-Zahavy (2015) suggests active participation in handover is associated with a reduction in errors.
Additionally,providingrationalesforclinicaldecisionshasbeenfoundtoimproveclinicalreasoning,enabling
thereceivingnursetoanticipateandplancare(Bakon,Wirihana,Christensen,Craft,2017).
Thereisaneedtodeveloplearningopportunitiesforstudentnursestodeveloptheirskillsinbothgivingand
receivinghandover.Handoverismorethanapassivetransaction;itprovidesaspaceforlearning,questioning
andutilisingclinicalreasoningskillstomakejudgementsaboutpatients.Studentsneedtomovebeyondusing
ISBARforthepassiverelayandone-waytransmissionofpatientinformation.Inadditiontoimplicationsfor
patientsafety,theundergraduatenursingcurriculumisembeddedinWorkIntegratedLearning(WIL).Strong
industry partnerships are critical for the implementation of the curriculum. Learning opportunities are
neededforstudentstoapplyworkskillsintheclassroom,toimprovetheemployabilityofgraduates.
Clinicalreasoningisanessentialcomponentofhealthcarepractice.Innursing,itistheprocessofmaking
professionaljudgementsanditisdependentonthedevelopmentofcriticalthinking(Banning,2008).Nurses
withinadequateclinicalreasoningskillsoftenfailtodetectpatientdeterioration(Levett-Jonesetal,2010)
andevidencesuggeststhatgraduatenursesmaylacktheclinicalreasoningskillstoprovidesafepatientcare
(Hunter&Arthur,2016).Inconsiderationofthesefactors,learningopportunitiesareneededtostimulate
studentstoapplycriticalthinkingduringthehandoverprocesssothatclinicalreasoningcanbedeveloped.
APotentialSolution
TheResearchSkillsDevelopment(RSD)framework(Willison,2017)wasusedintutorialsasaconceptualtool
forfinalyearstudentnursestodevelop,articulateandapplytheprocessesofcriticalthinkingandclinical
reasoning.Studentswereinitiallyprovidedwithastimulusposedasaclinicalproblemwhich,whendiscussed
intutorials,wasusedtounpackthefacetsoftheRSDframework,andforgethelinktoclinicalreasoning.
Students then received a video handover of a patient, designed to simulate the clinical environment.
Students applied theRSD framework to the informationobtained in thehandover. This process assisted
studentstocriticallyreflect,clearlyarticulaterisksandconcerns,andorganisetheinformationtheyreceived.
This made the clinical reasoning process more explicit, developing students’ conscious awareness and
confidence when analysing information. Students then had the opportunity to apply this learning in
simulatedscenariosduringtheirclinicalskillslaboratoryworkshops.

I-MELT, 11-13 December 2017
3
Evaluation
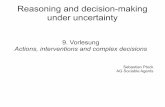
ThiswasatrialusingtheRSDframeworktostimulatecriticalthinkingandtheapplicationofclinicalreasoning
tothehandoverprocess.UndergraduatestudentnursesarrangedtheRSDfacetssothattheywereapplicable
andmeaningfulforthispurpose(seefigure1).SomefacetsoftheRSDframeworkwereveryclearlyapplied
tosupportclinical reasoningduringhandover,particularly ‘EmbarkandClarify’.Someaspectsof theRSD
frameworkcutacrossmanyaspectsoftheclinicalreasoningprocess,resultinginconfusion.However,this
wasconsolidatedthroughoutthesemesterastheapplicationoftheRSDfacetsbecamemorefamiliarand
studentswereabletoadaptthem.
Thecurriculumneedstobedevelopedtoscaffoldthisteachingandlearningactivity.Prior learningabout
clinicalhandoverisrequired.ThisneedstoreachbeyondusingISBARasatoolforthepassivetransmission
ofinformation;studentsneedtobeawareoftherisksassociatedwithclinicalhandoverandtheimportance
ofaskingcriticalquestions.Duringthistrial,thefocuswaspredominantlyonreceivingclinicalhandover.This
activityneedstobedevelopedfurthertoincorporategivingclinicalhandover.Clearerlinksalsoneedtobe
madetoclinicalskillslaboratorypracticeandtheRSDfacetsandpentagonneedtobeavailabletostudents
duringtheseworkshops.
Toeffectively evaluate this teachingand learningactivity, itwill be important todrawon students’ own
experience of giving and receiving handover prior to commencing this work. Further evaluation will be
requiredaftertheimplementationofthisactivityandafterthestudent’sclinicalpracticumtoascertainthe
translationoflearningtoclinicalpractice.
Conclusion
Thisteachingand learningactivitywasdevelopedforstudentnursestoapplycritical thinkingandclinical
reasoningskillstoclinicalhandover.AftertriallingtheapplicationoftheRSDframeworkforthispurpose,this
activitywillbedevelopedtoenableformalevaluationoftranslationtoclinicalpractice.Thecurriculumoverall
needstoincorporateteachingandlearningactivitiesinrelationtogivingandreceivinghandover,whereasit
iscurrentlyaskillthatistakenforgranted.Furtherresearchisneededtoinvestigatethelinksbetweenclinical
handoverandpatientsafety.

I-MELT, 11-13 December 2017
4
Communicate&Apply
Figure1
‘Whenindoubt,returntothecentre’
Analyse& Synthesise
Embark&Clarify
Organise&Manage
Evaluate&Reflect
Find& Generate
What is my role in the handover process?
What is my level of accountability and responsibility to this patient?
Is there anything affecting my ability to give/receive handover?
How can I organise information during handover?
Do I understand the information I have about this patient?
What does this information mean?
What conclusions can I draw about the safety of the patient?
What questions to I need to ask about this patient?
How can I elicit the information I need effectively?
Is anything impacting on my ability to communicate?
Where can I find additional information?
What resources do I have and are they reliable?
How did the handover impact the safety of my patient / my shift?
What did I do well?
What do I need to do next time?
How can I continue to develop my skills and confidence?

I-MELT, 11-13 December 2017
5
References
AustralianCommissiononSafetyandQuality inHealthCare(2010).TheOSSIEGuidetoClinicalHandover
Improvement.Sydney,ACSQHC.Retrievedfrom:
https://www.safetyandquality.gov.au/wp-content/uploads/2012/01/ossie.pdf
Australian Commission on Quality and Safety in Healthcare (2011). Implementation toolkit for clinical
handover improvement.Retrieved from:https://www.safetyandquality.gov.au/our-work/clinical-
communications/clinical-handover/implementation-toolkit-for-clinical-handover-improvement-
and-resource-portal/
Bakon,S.,Wirihana,L.,Christensen,M.,&Craft,J.(2017).Nursinghandovers:anintegrativereviewofthe
differentmodelsandprocessesavailable.InternationalJournalofNursingPractice,23,e125,5-8.
Banning,M.(2008).Clinicalreasoninganditsapplicationtonursing:conceptsandresearchstudies.Nurse
EducationinPractice,8,177-183.
Drach-Zahavy,A.,&Hadid,N.(2015)Nursinghandoversasresilientpointsofcare:linkinghandoverstrategies
totreatmenterrorsinthepatientcareinthefollowingshift.JournalofAdvancedNursing,71(5),
1135–1145.
Hunter,S.,&Arthur,C.(2016).Clinicalreasoningofnursingstudentsonclinicalplacement:clinical
educators’perceptions.NurseEducationinPractice,18,73-79.
Levett-Jones,T.,Hoffman,K.,Dempsey,J.,Yeun-SimJeong,Noble,D,Norton,C,A.,Roche,J&Hickey,N.
(2010).The‘fiverights’ofclinicalreasoning:aneducationalmodeltoenhancenursingstudents’
abilitytoidentifyandmanageclinically‘atrisk’patients.Nurseeducationtoday,30,515-520.
Mannix,T.,Parry,Y&Roderick,A.(2017).Improvingclinicalhandoverinapaediatricward:implicationsfor
nursingmanagement.JournalofNursingManagement,25,215-222.
Spooner,A,J.,Chaboyer,W.,Corley,A.,Hammond,N&Fraser,J,F.(2013).Understandingcurrent
intensivecareunitnursinghandoverpractices.InternationalJournalofNursingPractice,19,214-
220.
Rixon,S.,Braaf,S.,Williams,A.,Liew,D&Manias,E.(2017).Thefunctionsandrolesofquestioningduring
nursinghandoversinspecialtysettings:anethnographicstudy.ContemporaryNurse,53,(2),182-
195.
Rayo,M.F.,Mount-Campbell,A.F.,O’Brien,J.M.,White,S.E.,Butz,A.,Evans,K.,&Patterson,E.S.(2014).
Interactivequestioningincriticalcareduringhandovers:atranscriptanalysisofcommunication
behavioursofphysicians,nursesandnursepractitioners.BMJQualityandSafety,23,483-489.
Willison,J.(2017).ModelsofEngagedLearningandTeaching.Retrievedon20/2/17from:
http://www.adelaide.edu.au/rsd/i-melt
Top Related