






Languages
Pages
Legal


Safety and risk management in hospitalsMichel Dückers, PhD
Marjan Faber, PhD
Juliëtte Cruijsberg, MSc
Richard Grol, PhD
Lisette Schoonhoven, PhD
Michel Wensing, PhD
IQ Scientific Institute for Quality of Healthcare,Radboud University Nijmegen Medical Centre
December 2009


Acknowledgements
This study was produced as part of the Quest for Quality and Improved Performance (QQUIP), an initiative of the Health Foundation. Thanks are due to anonymous reviewers.
QQUIP and the Quality Enhancing Interventions project
QQUIP (Quest for Quality and Improved Performance) is a five-year research initiative of the Health Foundation. QQUIP provides independent reports on a wide range of data about the quality of healthcare in the UK. It draws on the international evidence base to produce information on where healthcare resources are currently being spent, whether they provide value for money and how interventions in the UK and around the world have been used to improve healthcare quality.
The Quality Enhancing Interventions component of the QQUIP initiative provides a series of structured evidence-based reviews of the effectiveness of a wide range of interventions designed to improve the quality of healthcare. The six main categories of Quality Enhancing Interventions for which evidence will be reviewed are shown below.
For more information visit www.health.org.uk/qquip

Published by:
The Health Foundation90 Long AcreLondon WC2E 9RATelephone: 020 7257 8000Facsimile: 020 7257 8001
www.health.org.uk
Registered charity number 286967Registered company number 1714937
First published December 2009
ISBN 978-1-906461-13-3
Copyright The Health Foundation
All rights reserved, including the right of reproduction in whole or in part in any form.
Every effort has been made to obtain permission from copyright holders to reproduce material. The publishers would be pleased to rectify any errors or omissions brought to their attention.

Dückers et al
Safety and risk management in hospitals
i
Contents
Glossary of acronyms iii
Executive summary iv
1. Introduction 1Safety and risk management concepts and definitions 1A continuous process 2Safety and risk management in hospitals 5A new research contribution 5
2. Objectives and methods 6Objectives 6 Methods 6 Data sources and searches 6 Search strategy 6 Study selection and data extraction 7
3. Results 11About the studies found 11 Number of studies 11 Methodological quality 11 Research setting 11Detection 11 Incident reports 13 Analysis techniques 14Mitigating factors 16 Actions to reduce risk 16 Reducing the number and severity of medication errors 16 Reducing the number and severity of fall incidents 18 Reducing diagnostic errors 19 Reducing the number and severity of adverse events and risks 19 Other safety or risk effects 20
4. Discussion 21 Main findings 21 Detection 21 Actions to reduce risk 21 Resilience 22Limitations 22
Contents

Dückers et al
Safety and risk management in hospitals
ii
Future research 23 Effectiveness detection 23 Continuous safety and risk management and resilience 23 Combined safety and risk management and implementation science 24 Expanding and improving safety and risk management research 24
References 25
Appendix A: Example of a search strategy and results 30
Appendix B: EPOC methodological filter 31
Appendix C: Study topics and interventions per SRM activity, sorted by design 32
Appendix D: Quality of study design 34
Appendix E: Included studies, sorted by alphabetical order 36
Contents

Dückers et al
Safety and risk management in hospitals
iii
Glossary of acronyms
ADE – adverse drug event
AE – adverse event
AIMS – Australian Incident Monitoring System
ARIMA – autoregressive integrated moving average
CBA – controlled before-after study
CI – criticality indices
CIT – critical incident technique
CPOE – computerised physician order entry
CWS – comparison with standards
EPOC – Effective Practice and Organisation of Care Group
FMEA – failure mode and effect analysis
MeSH – Medical Subject Heading
ICPS – International Classification for Patient Safety
IOM – Institute of Medicine
ITS – interrupted time series study
IV – intravenous
NICU – neonatal intensive care unit
OACM – organisational accident causation model
PDA – personal digital assistant
QEI – Quality Enhancing Interventions
QQUIP – Quest for Quality and Improved Performance
RCA – root cause analysis
RCT – randomised controlled trial
SEA – significant event auditing
SRM – safety and risk management
UBA – uncontrolled before-after study
WHO – World Health Organization
Glossary of acronyms

Dückers et al
Safety and risk management in hospitals Executive summary
iv
Executive summary
IntroductionPatient safety has become a matter of interest to healthcare professionals, governments and researchers worldwide. During the last decade, many studies have been conducted to assess the prevalence, severity and causes of a large variety of different types of adverse events in hospitals, as well as the effectiveness of various approaches to enhance safety.
ObjectivesThe objectives of this systematic review were:
1. to synthesise the evidence on the effectiveness of detection, mitigation and actions to reduce risks in hospitals; and
2. to identify and describe the components of interventions that are responsible for effectiveness.
MethodsThirteen literature databases were examined in May and June 2008 following a predefined search strategy. We included studies of sufficient methodological quality if these dealt with the effects of safety and risk management (SRM) in a hospital setting. At least two reviewers assessed the title and abstracts of unique studies. Two reviewers, working independently, studied the retrieved full-text articles and extracted information on their methods and results.
ResultsThirty-eight studies were included in the final review:
• three systematic reviews
• six randomised controlled trials (RCTs)
• four controlled before-after studies (CBAs)
• nine interrupted time series studies (ITSs)
• sixteen uncontrolled before-after studies (UBAs).
The types of interventions and outcomes were classified into three categories (two studies fitted in more than one category):
1. detection (nine studies)
2. mitigating factors (no studies)
3. actions to reduce risks (thirty-one studies).

Dückers et al
Safety and risk management in hospitalsExecutive summary
v
Detection
Studies could be divided into two categories: incident reports and analysis techniques.
Incident reports
All studies showed positive effects on the quality and/or quantity of reports. Specific findings were:
• The total error rate was higher in studies using voluntary reporting than in a study using mandatory reporting.
• Voluntary incident reporting may be associated with under-reporting in specific professions and in specific types of incidents.
• Nurses reported considerably more often than doctors.
• Incidents involving medication are reported most frequently.
• Feedback to the reporter is seen as an important way of encouraging staff to continue reporting incidents.
• Multi-institutional reporting, where information is gathered about adverse events in different hospitals and analysed centrally, identified rare but important problems.
• Paper-based reporting sometimes helps to increase reporting rates rather than a web-based tool.
Analysis techniques
Many publications were found relating to analysis techniques in industry and healthcare, although these did not focus on effects or effectiveness. Only two evaluations were identified; both showed positive results. However, systematic evidence on the effectiveness of safety analysis remains limited.
Mitigating factors
Mitigating factors are actions or circumstances that prevent or moderate the progression of an incident towards harming a patient. We did not identify any studies that fitted in this category.
Actions to reduce risks
The majority of the studies we examined dealt with this topic.
Actions taken to reduce risk concentrate on preventing the reoccurrence of the same or similar safety incidents, and on improving system resilience. The main patient outcome categories were:
• medication errors (for example, computerised physician order entry [CPOE]; pharmacist participation in rounds; education tools; clinical decision support systems; bar coding; organisation-wide safety programmes; smart-pump technology – an infusion system that checks that medication programming is within pre-established institutional limits before infusion can begin; structured order sheets – a standardised order sheet containing a number of pre-structured information categories; the Breakthrough Series, which uses a collaborative approach to enhance learning and reduce medication errors; failure mode and effect analysis [FMEA]
• fall incidents (for example, multi-component falls prevention programmes; flooring types; types of physiotherapy)

Dückers et al
Safety and risk management in hospitals Executive summary
• diagnostic errors (for example, computerised decision support and web-based reminder systems)
• adverse events and risks (for example, reporting systems; computerised clinical information systems; retrospective medical-record screening and review; or a combination of interventions, including multidisciplinary rounds led by doctors, and culture interventions)
• simulated survival (for example, human simulation training).
ConclusionResearch evidence for safety interventions in hospitals has remained limited. Published studies predominantly report on positive effects; however, the methodological quality of the studies is generally weak. The diversity of the collected material made it problematic to combine studies quantitatively. SRM interventions applied in a hospital setting are multifaceted and therefore it was difficult to disentangle the effects from the context in which they were implemented. This makes it challenging to formulate recommendations for future implementation to professionals and policy-makers. There is therefore a pressing need for high-quality evaluations of the effectiveness – and cost-effectiveness – of SRM interventions.
vi

Dückers et al
Safety and risk management in hospitals
1
1. Introduction
1. Introduction
This study is part of the Health Foundation’s QQUIP (Quest for Quality and Improved Performance) research initiative. One of the three main focuses of QQUIP is the Quality Enhancing Interventions (QEI) programme, which includes a series of structured, evidence-based reviews of the effectiveness of a wide range of interventions designed to improve the quality of healthcare. The programme aims to answer the question: ‘What works to improve quality and performance?’ There are six categories in the QEI programme, and this study falls within the category of ‘organisational interventions’ and focuses on safety and risk management (SRM).
Patient safety has increasingly become a matter of interest to governments, health professionals and scholars internationally. Over the last decade a great deal of research has been conducted to assess the prevalence, severity and causes of many different types of adverse events, as well as the effectiveness of efforts and approaches to enhance safety, and reduce risks and adverse events. SRM interventions relate to a wide variety of organisational aspects linked to safety and risks, ranging from co-ordination, resource allocation and standardisation in healthcare organisations, to issues of human resource management, communication, information technology, and inter-institutional improvement initiatives.
Safety and risk management concepts and definitionsThe MeSH is the US National Library of Medicine’s controlled vocabulary thesaurus. It consists of sets of terms that name descriptors in a hierarchical structure. This allows users to search at various levels of specificity. The Medical Subject Heading (MeSH) of ‘safety management’ was introduced in 1994. It encompasses:
the development of systems to prevent accidents, injuries, and other adverse occurrences in an institutional setting. The concept includes prevention or reduction in adverse events or incidents involving employees, patients, or facilities. Examples include plans to reduce injuries from falls or plans for fire safety to promote a safe institutional environment.
(MeSH 2009)
Safety management belongs to the MeSH tree of ‘risk management’, a heading that was introduced in 1990. Risk management involves:
the process of minimizing risk to an organization by developing systems to identify and analyze potential hazards to prevent accidents, injuries, and other adverse occurrences, and by attempting to handle events and incidents which do occur in such a manner that their effect and cost are minimized. Effective risk management has its greatest benefits in application to insurance in order to avert or minimize financial liability.
(MeSH 2009)
The World Health Organization (WHO) Conceptual Framework for the International Classification for Patient Safety (ICPS) offers a definition of SRM, restricted to a healthcare setting:
activities or measures taken by an individual or a health care organization to prevent, remedy or mitigate the occurrence or reoccurrence of a real or potential (patient) safety event.
(WHO, World Alliance for Patient Safety 2009)

Dückers et al
Safety and risk management in hospitals
2
1. Introduction
The ICPS aims to define, harmonise and group a standardised set of patient safety concepts – with agreed definitions, and labelled with preferred terms – into an internationally acceptable classification in a way that is conducive to learning and to improving patient safety over time and across borders (Sherman et al 2009).
A widely accepted definition of ‘patient safety’ comes from the Institute of Medicine (IOM). In To err is human patient safety is described ‘as the freedom from accidental injury due to medical care or from medical error’ (IOM 2000). The ICPS provides another definition:
the reduction of risk of unnecessary harm associated with healthcare to an acceptable minimum. An acceptable minimum refers to the collective notions of given current knowledge, resources available and the context in which care was delivered weighed against the risk of non-treatment or other treatment.
(WHO, World Alliance for Patient Safety 2009)
None of the definitions presented so far conflict with each other. They all refer to intentional actions, activities and measures: part of an organisational improvement or learning process in a healthcare setting. Other relevant phrases relating to patient safety are ‘medical error’, ‘near miss’ and ‘adverse event’. Again a leading definition comes from the ICPS:
An error is a failure to carry out a planned action as intended or application of an incorrect plan. Errors may manifest by doing the wrong thing (commission) or by failing to do the right thing (omission), at either the planning or execution phase.
(WHO, World Alliance for Patient Safety 2009)
Fallowfield and Fleissig (2004) suggest that medical errors should be distinguished from negligence or malpractice, insofar as the first is accidental while the second two are deliberate violations of a rule or standard of behaviour. Furthermore, medical errors do not lead to observable injury to the patient in all cases. The situations that did not cause harm to patients, but could have done, are described as ‘near miss’ (Wilson et al 1996). The term ‘adverse event’ is used for incidents in which the person receiving healthcare was harmed (Leape et al 1993). In their study, Leape et al identified a range of factors that contribute to adverse patient events, categorising them as diagnostic, treatment, preventive and other.
A continuous process In its simplest form, SRM in healthcare can be conceptualised as a continuous process in which healthcare providers respond to safety incidents, medical errors and expected risks. A logical starting point for an attempt to collect and synthesise the evidence on effective SRM interventions is to make an inventory of key concepts. An understanding of the patient safety literature, however, has been compromised by the inconsistent use of language (Runciman et al 2009). Similar patient safety concepts use different terms (for example ‘near miss’, ‘close call’), and identical terms are used to embrace several concepts (for example ‘medical error’ for errors, violations and system failures – see also Runciman et al 2006; Elder, Pallerla and Regan 2006. To meet the need for clarification and standardisation, the WHO’s World Alliance for Patient Safety has undertaken a project to develop an ICPS.
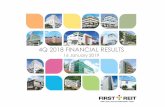
The current conceptual framework for the ICPS consists of three categories that are linked in several ways semantically (see Box 1). Two of the categories relate to the ‘clinically meaningful’ categorisation of an incident (based on incident types and patient outcomes) and ‘descriptive information’ about the context of the incident, including patient characteristics, incident characteristics, contributing factors/hazards and organisational outcomes. The third category, ‘proactive and reactive system resilience’, affects the activities and measures relating to SRM, and is the focus of this study. Within the ICPS, a distinction is made between detection, mitigating factors, ameliorating actions and actions taken to reduce risk (see Figure 1).

Dückers et al
Safety and risk management in hospitals
3
1. Introduction
Box 1: Ten classes within the conceptual framework for the ICPS
Clinically meaningful incident categorization• Incident type is a descriptive term for a category made up of incidents of a common nature
grouped because of shared, agreed features, such as ‘clinical process/procedure’, ‘resources/organizational management’ or ‘medication/IV fluid’ incident.
• Patient outcome is the impact upon a patient, which is wholly or partially attributable to an incident. Patient outcomes can be classified according to type of harm, degree of harm and any social and/or economic impact.
Descriptive information providing context for the incident• Patient characteristics categorize patient demographics, the original reason for seeking care and
the primary diagnosis.
• Incident characteristics classify the information about the circumstances surrounding the incident, such as where and when in the patient’s journey through the healthcare system the incident occurred, who was involved and who reported it.
• Contributing factors/hazards are the circumstances, actions or influences which are thought to have played a part in the origin or development of an incident or to increase the risk of an incident. Examples are human factors such as behaviour, performance or communication; system factors, such as work environment and external factors beyond the control of the organization, such as the natural environment or legislative policy. More than one contributing factor and/or hazard is typically involved in a single patient safety incident.
• Organizational outcomes refer to the impact upon an organization which is wholly or partially attributable to an incident such as an increased use of resources to care for the patient, media attention or legal ramifications.
System resilience (proactive and reactive risk management)The concept of ‘resilience’ in the context of the ICPS is defined as the degree to which a system continuously prevents, detects, mitigates or ameliorates hazards or incidents so that an organization can ‘bounce back’ to its original ability to provide core functions.
• Actions taken to reduce risk concentrate on steps taken to prevent the reoccurrence of the same or similar patient safety incident and on improving system resilience. Actions taken to reduce risk are those actions taken to reduce, manage or control any future harm, or probability of harm, associated with an incident. These actions may be directed toward the patient (provision of adequate care, decision support), toward staff (training, availability of policies/protocols), toward the organization (improved leadership/guidance, proactive risk assessment), and toward therapeutic agents and equipment (regular audits, forcing functions). Detection, mitigating factors and ameliorating actions both influence and inform the actions taken to reduce risk.
• Detection is defined as an action or circumstance that results in the discovery of an incident. For example, an incident could be detected by a change in the patient’s status, or via a monitor, alarm, audit, review or risk assessment. Detection mechanisms may be built into the system as official barriers or informally developed.
• Mitigating factors are actions or circumstances that prevent or moderate the progression of an incident toward harming the patient. Mitigating factors are designed to minimize the harm to the patient after the error has occurred and triggered damage control mechanisms.
• If the incident does result in harm, ameliorating actions can be introduced. Ameliorating actions are those actions taken or circumstances altered to make better or to compensate any harm after an incident. Ameliorating actions apply to the patient (clinical management of an injury, apologizing) and to the organization (staff debriefing, culture change and claims management).
Source: Sherman H, Castro G, Fletcher M et al (2009). ‘Towards an International Classification for Patient Safety: the conceptual framework’. International Journal for Quality in Health Care, vol 21, pp 4–7, by permission of Oxford University Press

Dückers et al
Safety and risk management in hospitals
4
1. Introduction
actio
ns ta
ken
to re
duce
ris
k
detection
actions taken to reduce risk
mitigating factors
ameliorating actions
contributing factors/hazards
organisational outcomes
influences informs
influences informs
influences informs
patient characteristics incident characteristicsincident
type
informs informs
patient outcome
influences informs
System resillience (proactive and reactive risk management)
Descriptive information
Clinically meaningful recognisable categories for incident identification
Figure 1: Conceptual framework for the ICPS
Source: Sherman H, Castro G, Fletcher M et al (2009). ‘Towards an International Classification for Patient Safety: the conceptual framework’. International Journal for Quality in Health Care, vol 21, p 4, by permission of Oxford University Press

Dückers et al
Safety and risk management in hospitals
5
1. Introduction
Safety and risk management in hospitals
This review focuses on SRM in hospitals. Most research on the effectiveness of SRM strategies has been carried out in hospital settings, with little in primary and community settings or in people’s homes (Øvretveit 2008). In terms of risk, hospitals are a relatively hazardous working environment for both patients and staff. Hospital staff must continuously deal with adverse events and numerous potential risks relating to surgery, anaesthetics and patient transfers: for example, wound infections, medication errors, wrong-site surgery. The relatively high risk of unsafe situations makes the hospital sector an important setting for an assessment of various approaches to SRM.
A new research contribution There is a substantial body of research in the area of patient safety. It is an ongoing challenge to keep track of the growing literature base and to categorise study findings and their implications in an orderly way. In their systematic review, Hoff et al (2004) examined the relationship between system features and safety outcomes. They considered the evidence available on associations between organisational dynamics, medical errors and patient safety. Their contribution involved an exploration of the relevance of, among others, culture, organisational structure, teams, feedback, opinion leaders, board leadership, educational programmes and information technology. Only a small number of studies confirmed a relationship between system components and errors or safety. This is an important finding. A possible explanation might be that the distance between system features and medical errors and safety events as investigated by Hoff et al (2004) is too large. A complementary perspective is that the field of organisational dynamics covers important conditions but that the association between conditions and safety outcomes depends on the successful implementation of specific SRM interventions. In other words, interventions – and not the organisational features – are linked more directly to patient safety. The effectiveness of such interventions, implemented within hospital organisations, is the main focus of our systematic review.
Given the gradual progress that is being made in the development of an international taxonomy and conceptual framework (see Figure 1), we apply our review on the effectiveness of SRM interventions from a system resilience perspective. The concept of resilience as defined by the ICPS is ‘the degree to which a system continuously prevents, detects, mitigates or ameliorates hazards or incidents’ so that an organisation can ‘bounce back’ to its original ability to provide core functions (Sherman et al 2009). Resilience is, in that sense, closely linked to actions to reduce risk. We underline the notion that, together, detection and mitigation can impede the progression of an incident from reaching and/or harming a patient. However, we refrain from placing undue emphasis on the effectiveness of ameliorating actions (that is, responses to harm), unless a direct influence is assessed of reactive ‘damage control’ actions on the dependent variable. Variables may include the number and severity of medical errors, adverse events, events reported, or hazards/root causes identified.

Dückers et al
Safety and risk management in hospitals
6
2. Objectives and methods
2. Objectives and methods
ObjectivesThe objectives of this study were to synthesise the evidence on the effectiveness of detection, mitigation and actions to reduce risks in hospitals, and to identify and describe the components of interventions that are responsible for effectiveness.
MethodsData sources and searches
A search for all relevant articles published before May 2008 was conducted in May and June 2008 of the following databases:
• PubMed
• PsycINFO
• Embase
• Cochrane Database of Systematic Reviews
• Database of Abstracts of Reviews of Effects (DARE)
• Cochrane Central Register of Controlled Trials
• Health Technology Assessment (HTA)
• NHS Economic Evaluation Database (NHS EED)
• Cumulative Index to Nursing and Allied Health Literature (CINAHL)
• King’s Fund
• World Health Organization Library and Information System (WHOLIS)
• CSA Sociological Abstracts
• Web of Science.
Search strategy
When searching for SRM literature, it became apparent at an early stage that we would need to apply additional limits, rather than just combining SRM with hospital terms as sector restrictors. Hospitals – together with risk and safety management (both as text words and MeSH headings) – resulted in almost 16,000 hits in PubMed, even when we applied a design filter from the Cochrane Effective Practice and Organisation of Care Group (EPOC). We therefore added a number of patient safety-related phrases to the search strategy. The final search strategy was based on SRM in relation to medical errors, adverse events, incidents and near misses, restricted to the hospital sector (see Box 2). An example of a search strategy from one database can be found in Appendix A.

Dückers et al
Safety and risk management in hospitals
7
2. Objectives and methods
Box 2: Search strategy
Search term
#1 ‘risk management’ (all fields, if possible MeSH)
#2 ‘safety management’ (all fields, if possible MeSH)
#3 2 OR 3
#4 ‘medical error(s)’ (all fields, if possible MeSH)
#5 ‘incident(s)’ (all fields)
#6 ‘adverse event(s)’ (all fields)
#7 ‘near miss(es)’
#8 4 OR 5 OR 6 OR 7
#9 ‘hospital(s)’ (all fields, if possible MeSH)
#10 3 AND 8 AND 9
#11 EPOC methodological filter
#12 10 AND 11
Study selection and data extraction
Types of studies
To determine which studies to include, we used a general hierarchy of evidence classification (from higher to lower validity):
• systematic reviews of reviews
• systematic reviews of studies
• individual randomised controlled trials
• quasi-experimental studies (for example, experimental studies without randomisation)
• controlled observational studies (for example, cohort or case-control studies)
• observational studies without a control group (for example, interrupted time series studies, uncontrolled before-after studies or case series).
Based on an exploration of available experimental studies, we considered all systematic reviews, randomised controlled trials (RCTs), controlled before-after studies (CBAs), interrupted time series studies (ITSs) and uncontrolled before-after studies (UBAs) as candidates for inclusion. To ensure that primarily studies with the preferred design were included in the study, we used a methodological filter (see Appendix B). We excluded studies that were not published in English, case studies or studies that did not include comparisons with a control group or pre-intervention episodes.

Dückers et al
Safety and risk management in hospitals
8
2. Objectives and methods
Types of interventions and setting
The review focused on three types of organisational interventions:
1. Detection: an action or circumstance that results in the discovery of an incident.
2. Mitigating factor: an action or circumstance that prevents or moderates the progression of an incident towards harming a patient.
3. Actions to reduce risks: actions taken to reduce, manage or control any future harm, or probability of harm, associated with an incident.
Types of outcome measures
SRM can influence different sorts of outcomes and this review focused on two types: the effects on safety and risk, and the effects on incident reporting and tracking. In the first case, outcomes were associated with changes in the safety and risk situation, so an SRM intervention was considered effective if it led to specific outcomes, such as the reduction in the number of (possible) incidents, errors, near misses and adverse events. In the second case, since an effective SRM cannot take place without adequate detection, it is likely that effective detection techniques will result in an increased quality or quantity of reported incidents (see Box 3).
Box 3: Types of outcome measures
Effects Examples
Effects on safety and risks Reducing the frequency or severity of:
• fall incidents
• wound infections
• misuse
• medication errors
Effects on incident reporting and tracking • Frequency
• Categories and severity/seriousness
• Willingness to report
• Differences between groups of practitioners (eg nursing staff or doctors)
Study selection procedure
Two reviewers, working independently, screened the papers found based on title and abstract, or, if necessary, the complete text. A third reviewer was consulted in those cases in which discrepancies were found.
We excluded studies from our review if they did not report any actual changes in the safety and risk situation, or any effect on monitored or reported incidents and risks. We also excluded studies if the intervention was not clearly defined.

Dückers et al
Safety and risk management in hospitals
9
2. Objectives and methods
Data extraction
One reviewer carried out the data extraction of full-text studies, and a second reviewer checked this using a pre-structured extraction form. The content of each paper included was summarised in descriptive texts. In the case of systematic reviews (of reviews), the topic, setting, search period, data sources, number of included studies, main outcomes (see Box 3) and conclusions were described. For non-review papers, the study setting and the nature of the intervention were described. For all included papers, an indication of the strength of the study was reported, based on the extent to which EPOC criteria for reviews, RCTs, CBAs and ITSs were met (as defined by The Cochrane Collaboration). The methodological quality of the reviews was determined by the quality of the studies they included, as well as the extent to which a systematic approach was followed. Criteria taken into account were:
• at least two authors scored eligibility
• authors used inclusion and exclusion criteria
• designs were judged using predefined criteria (EPOC, Jahad, etc)
• at least two authors scored findings
• authors used data extraction forms.
RCTs were assessed using seven criteria:
1. protection against selection bias
2. protection against contamination (for example, randomising organisations/professionals rather than individual patients)
3. protection against exclusion bias
4. follow-up of patients or episodes of care
5. comparability of baseline measurements
6. protection against detection bias (blinded assessment of primary outcomes)
7. reliability of primary outcome measures.
CBAs were judged using seven criteria:
1. protection against contamination
2. protection against exclusion bias
3. follow-up of patients or episodes of care
4. comparability of baseline measurements
5. protection against detection bias
6. characteristics for studies using second site as control
7. reliability of primary outcome measures.
The methodological quality of ITSs were determined using eight criteria:
1. intervention was independent of other changes
2. data analysed appropriately (autoregressive integrated moving average [ARIMA] or time series regression)
3. reason given for number of points pre and post intervention
4. shape of intervention effect was specified

Dückers et al
Safety and risk management in hospitals
10
2. Objectives and methods
5. intervention unlikely to affect data collection
6. protection against detection bias
7. completeness of data set
8. reliability of outcome measures.
UBAs were rated on one criteria only: the reliability of the primary outcome measure.
The summarising labelling of the methodological quality was based on two rules:
• Rule 1: if zero to two of the criteria were not fulfilled, for example, rated as ‘not done’ or ‘unclear’, in the case of an RCT, CBA or ITS, the study was considered strong. Studies were classed as moderate when three to maximally half of the criteria were not fulfilled. With weak studies, more than half of the criteria were not fulfilled.
• Rule 2: extra weight was given to fundamental characteristics of different studies, as critical aspects of the methodological quality had to be guaranteed. Strong RCTs and CBAs were rated as moderate if the comparability of control groups was not fulfilled. UBAs were rated as weak if the criterion on the reliability of the primary outcome measure was not fulfilled.
Synthesis of data
Our discussion of the evidence on SRM interventions has been organised into the activities described in the ICPS conceptual framework. We have described relevant characteristics for each activity, such as the study objectives and design, the nature of the intervention and the effects reported. Detailed information, for example, about the country, research setting and the statistical tests applied, can be found in Appendix E.

Dückers et al
Safety and risk management in hospitals
11
3. Results
3. Results
About the studies foundNumber of studies
Initially, we retrieved 3,772 references to studies from the various literature databases. Applying an EPOC design filter, in preparation for the first screening round, helped to reduce this to 1,872 studies. PubMed provided approximately 65 per cent of the studies. After checking the total number of studies for duplicates, we examined the abstracts of 1,645 unique studies using inclusion criteria (see Figure 2).
Two reviewers subsequently assessed 146 full-text articles and included 38 studies (see Appendix C for further details):
• three systematic reviews
• six randomised controlled trials (RCTs)
• four controlled before-after studies (CBAs)
• nine interrupted time series studies (ITSs)
• sixteen uncontrolled before-after studies (UBAs).
Methodological quality
We considered the design of four studies to be strong (Berner et al 2006; Paoletti et al 2007; Schneider et al 2006; Walsh et al 2008) and the design of seven studies to be moderate (Kozer et al 2005; Leape et al 1999; Lehmann et al 2007; Schwendimann et al 2006; Simon et al 2005; Snijders et al 2007; Voeffray et al 2006). The methodological quality of the remaining 27 studies was weak. (See Appendix D for further details.) Major limitations of these weak studies were the absence of studies with strong designs, and unclear descriptions of review procedures. In the case of RCTs, CBAs and ITSs, there was often uncertainty about the extent to which a perceived change was independent of other changes. The authors of most RCTs and CBAs could not guarantee the absence of contamination of interventions (that is, the possibility that the intervention reached the comparison group). ITSs were rarely examined with appropriate statistical techniques. The reliability of the outcome measure of many UBAs is unclear. In general, interventions were multifaceted or otherwise poorly specified.
Research setting
More than half of the material relates to studies in the USA. The other studies described interventions implemented in the UK, Australia, Canada, Hong Kong, the Netherlands and Switzerland. A limited number of studies made no distinction in the specialty or the types of patients treated. Other studies focused on: acute care, medical wards, ambulatory care, general internal medicine, paediatrics, cardiology, surgery, geriatrics, intensive care, and chemotherapy.
DetectionNine studies were identified on detection approaches. Studies could be divided into two categories: incident reports and analysis techniques. Two systematic reviews focused on incident reporting systems and their characteristics in relation to the size of effects (Simon et al 2005; Snijders et al 2007). Four empirical studies also described the effects of reporting systems, mainly voluntary or non-punitive

Dückers et al
Safety and risk management in hospitals
12
3. Results
Figure 2: Changes in the number of studies included during the review process
Total number of studies found (unfiltered) 3,772
PubMed 2,694PsycINFO 32Embase 285Cochrane Database of Systematic Reviews 13Database of Abstracts of Reviews of Effects 3Cochrane Central Register of Controlled Trials 11Health Technology Assessment database 4NHS Economic Evaluation Database 3CINAHL 557King’s Fund database 70WHOLIS 1CSA Sociological Abstracts 5Web of Science 94
Total number of studies found (filtered) 1,872
PubMed 1,197PsycINFO 19Embase 129Cochrane Database of Systematic Reviews 13Database of Abstracts of Reviews of Effects 3Cochrane Central Register of Controlled Trials 11Health Technology Assessment database 4NHS Economic Evaluation Database 3CINAHL 368King’s Fund database 70WHOLIS 1CSA Sociological Abstracts 5Web of Science 49
Unique studies: 1,645
Included after abstract scan: 146
Included for data extraction: 38
Extracted after EPOC filter: 1,900
Duplicates: 227
Excluded after abstract scan: 1,537
Excluded after full-text review: 108

Dückers et al
Safety and risk management in hospitals
13
3. Results
systems (Harris et al 2007; Lehmann et al 2007; Plews-Ogan et al 2004; Stump 2000). The other studies addressed an intervention package (Evans et al 2007), the Breakthrough Series, which uses a collaborative learning approach (Silver and Antonow 2000), and a multidisciplinary team addressing medication-related patient safety (Sim and Joyner 2002).
Incident reports
Effectiveness of reporting systems
The methodological quality of the studies in this category was moderate or weak. All of the studies reported positive effects on the quality or quantity of reported medical errors and incidents. One of the reviews (Simon et al 2005) assessed the effectiveness of hospital incident reporting systems in improving hospital and clinic performance in terms of patient safety, clinical outcomes, costs and operations. The authors included 11 studies published between 1994 and 2004: four with control conditions and seven uncontrolled evaluations. The main findings were that incident reporting and chart-review detection were less reliable than direct observation. The conclusion of the second review (Snijders et al 2007) was similar. Here the scope was narrowed to characteristics of incident reporting systems in neonatal intensive care units (NICU) in relation to type, aetiology, outcome and preventability of incidents. The search period was restricted to January 1980 and January 2006 and resulted in the inclusion of uncontrolled studies: eight prospective and two retrospective. Medication incidents were most frequently reported. Available data in the NICU showed that the total error rate was much higher in studies using voluntary reporting than in a study using mandatory reporting. Multi-institutional reporting, where information is gathered about adverse events in different hospitals and analysed centrally, identified rare but important errors. A substantial number of incidents were potentially harmful.
Various studies showed that the number of reports can be increased significantly by different approaches. Harris et al (2007) presented an increase of reporting incidence in their study of patient-safety event reporting in three intensive care units (medical, surgical and cardiothoracic). The introduction of a new, voluntary, card-based event reporting system was compared to existing online tools. In both systems, nurses submitted the majority of the reports (nurses 67.1 per cent; doctors 23.1 per cent; other reporters 9.5 per cent). However, with the paper-based system, the greatest increase in reporting related to doctors.
In a study by Lehmann et al (2007) the significant increase in the number of reports per month (from 19 to 102), and a change in the type of errors, was attributed to a revised medication event reporting policy that was implemented throughout the hospital in 2005. This policy was preceded by strategy sessions with the senior management about non-punitive reporting in the autumn of 1999 and small-scale implementation in October 2000.
Plews-Ogan et al (2004) described a substantial increase in the reporting of adverse events and near misses after the implementation of clinician-based near miss/adverse event voluntary reporting, coupled with systems analysis and redesign as a model for continuous quality improvement. The study took place in the ambulatory setting.
In a study by Stump (2000) the number of reported events increased considerably within one year after the medication error reporting process was redesigned in one hospital. The new process differed from the old one in the following ways:
• It was non-punitive.
• The central pharmacy department received a report within 48 hours rather than two to three months.
• A unified database was used instead of a fragmented process.

Dückers et al
Safety and risk management in hospitals
14
3. Results
• Near misses could be captured in every stage of the medication-use process and not only during the dispensing process.
• Structured check-box reports were used instead of handwritten free text.
• Staff at department level were involved in reviewing the data.
Effects of interventions other than reporting systems
Evans et al (2007) described a significant improvement in reporting in inpatient areas and in emergency departments after an intervention package was implemented. This included:
• a questionnaire and focus group to identify barriers for reporting
• a manual to improve knowledge
• education sessions
• the redesign of reporting processes to address concerns
• a one-page report form replacing the existing three-page form
• the introduction of a free-call telephone service
• the mailing of four feedback newsletters
• presentations being given at meetings.
Silver and Antonow (2000) reported how a Breakthrough Series model was applied to reduce the number of medication errors reported. Teams consisting of staff from quality improvement, pharmacy and medical departments attended seminars and acquired knowledge to enhance error reporting. Sim and Joyner (2002) linked an increase in reporting of medication variances to the introduction of a multidisciplinary team, formed to address medication-related patient safety initiatives. The team was set up in a community hospital that had a wide variety of acute care, critical care, emergency care and surgical and diagnostic services.
In summary, all studies, regardless of the quality of their design and the different interventions, described attempts to enhance incident and risk reporting. Nevertheless, incident reporting and chart review were found to be less reliable, complete and precise than observation. Nurses reported more often than doctors. There are also indications that the number of incidents reported was lower with mandatory rather than voluntary reporting.
Analysis techniques
Extensive literature is available on different analysis techniques. Woloshynowych et al (2005), for example, wrote an extensive and detailed publication on the nature and characteristics of different methods in industry and healthcare such as the Australian Incident Monitoring System (AIMS), the critical incident technique (CIT), comparison with standards (CWS), failure mode and effect analysis (FMEA), the organisational accident causation model (OACM), root cause analysis (RCA) and significant event auditing (SEA).
The study identified the following positive aspects of these methods:
• They contribute to priority setting.
• They emphasise the system and not the individual.
• They localise weak spots and risks.

Dückers et al
Safety and risk management in hospitals
15
3. Results
Negative elements included the following:
• They can be time consuming or complex.
• Their outcomes depend on the level of available expertise.
• A comprehensive answer is not always guaranteed.
Although relevant, the above study and other studies addressing reactive (for example, critical incident technique) or proactive (for example, FMEA) analysis techniques could not be included in this review as they do not focus on effects or effectiveness.
Two examples of studies that address the results of FMEA show that it enables changes to be monitored. Bonnabry et al (2005) conducted an FMEA to compare risks associated with the old and new process, to quantify the improved safety of the new process, and to identify the major residual risks in paediatric parental nutrition. A multidisciplinary team carried out the FMEA by following a series of process steps:
1. prescription
2. transmission to pharmacy
3. pharmaceutical validation
4. label production
5. compounding
6. quality control.
Several changes were implemented:
• new prescription software
• direct recording on a server
• automatic printing of the labels
• the creation of a file used to pilot an automatic compounder.
In the new process, the sum of the criticality indices (CI) of all 18 identified failure modes was reduced by 59 per cent compared with the old process. In the new process, the CIs of the different failure modes were reduced by a mean factor of seven.
Robinson et al (2006) also used FMEA to identify the elements of risk in chemotherapy, with the aim of implementing appropriate improvement strategies. The results of the analysis helped them to implement strategies in three processes: prescribing, dispensing and administration. The study concluded that it was feasible to improve potential error rates for prescribing, dispensing and administration. Actual effects were addressed in a later section of the study.
The main conclusion to be drawn in relation to different analysis methods and techniques is that, despite an abundance of descriptive material, information on their reliability and accuracy is limited. We did not find any studies comparing the effectiveness of analysis techniques.

Dückers et al
Safety and risk management in hospitals
16
3. Results
Mitigating factorsMitigating factors are designed to minimise the harm to a patient after an error has occurred and has triggered damage-control mechanisms (see Box 1 on page 3). We did not identify any studies that fitted in this category.
Actions to reduce riskThe remaining studies included in this review address interventions aimed at reducing risks. Actions taken to reduce risk concentrate on preventing the reoccurrence of the same or similar safety incidents and on improving system resilience (see Box 1). The main patient outcome categories were medication errors, fall incidents, diagnostic errors, human simulation training, adverse events, and safety risks.
Reducing the number and severity of medication errors
Medication was by far the largest category of safety improvement and risk-reduction interventions. We identified ten different types of interventions:
• computerised physician order entry (CPOE)
• pharmacist participation in doctors’/post-admission rounds
• education tools
• a clinical decision support system on a personal digital assistant (PDA)
• bar-code technology
• an organisation-wide safety programme
• smart-pump technology
• structured order sheets
• the Breakthrough Series
• failure mode and effect analysis (FMEA).
Computerised physician order entry
Four studies evaluated the effectiveness of CPOE implementation. One of them was a systematic review conducted by Shamliyan et al (2008). The hypothesis was tested that medication errors and adverse clinical events decrease with CPOE compared with handwritten orders by doctors in paediatric and adult patients, independent of patient and provider characteristics. The search period ranged from 1995 to 2004, and 12 studies were included: one RCT, nine UBAs and two studies with an unclear design. The main conclusion was that CPOE implementation was associated with a significant reduction in medication errors in adult and paediatric populations. However, results should be interpreted with caution. Effects may have been overestimated due to the use of non-randomised uncontrolled interventions. Implementation of CPOE was not associated with a substantial improvement in patient safety, and the studies did not allow broad generalisability. Two other studies also reported positive effects of CPOE (King et al 2003; Voeffray et al 2006). The authors of a fourth study – about CPOE in paediatric inpatient care – did not consider it as effective in reducing medication errors as it is in adult inpatient care (Walsh et al 2008).

Dückers et al
Safety and risk management in hospitals
17
3. Results
Pharmacist participation in doctors’/post-admission rounds
Two studies described how pharmacist participation in doctors’/post-admission rounds led to lower rates of preventable adverse drug events (Leape et al 1999) and enhanced accuracy of medication history (Fertleman et al 2005).
Education tools
Three studies examined the effectiveness of education tools. Simpson et al (2004) concluded that the impact of a combined risk-management/clinical pharmacist-led education programme on medication errors in an NICU was significantly positive. The results were similar to an assessment by Schneider et al (2006) of the influence of an interactive CD-ROM programme on the rate of medication administration errors made by nurses. However, this second approach did not contribute to a significantly reduced administration error rate. A study by Manning et al (2007) highlighted that a new web-based educational tool was not accompanied by a reduction in self-reported error rate either.
Clinical decision support system
Berner et al (2006) evaluated the effectiveness of a clinical decision support system on a PDA. The intervention group with the PDA decision support tool revealed a significantly lower mean proportion of cases per doctor with unsafe prescriptions for the intervention group than the control group, after adjustment for baseline rates.
Bar-code technology
Two studies dealt with the effectiveness of bar-code technology. Paoletti et al (2007) described the implementation of a multidisciplinary approach to systematically decrease medication errors by using observation methodology, electronic medication-administration records and bar-coded medication administration. The medication error rate decreased significantly in one of the two intervention groups and remained unchanged in the other. In the second study (Poon et al 2006) the implementation of bar-code technology resulted in a considerable reduction in dispensing errors and potential adverse drug events (ADEs).
Organisation-wide safety programme
Cohen et al (2005) focused on a possible reduction in adverse drug events as a result of an organisation-wide safety programme. The positive results – a significant reduction in ADE rate and the proportion of patients with ADEs – were attributed to a programme that included:
• the formation of a patient safety council
• assigning a full-time safety specialist
• the implementation of an event reporting system
• the introduction of drug protocols
• weekly medication-profile audits
• order standardisation.
Smart-pump technology
Smart-pump technology is an infusion system that checks that medication programming is within pre-established institutional limits before infusion can begin. Larsen et al (2005) conducted a study to determine whether combining standard drug concentrations with smart-pump technology reduced reported medication-infusion errors. They found that the significant reduction in the number of reported errors was associated with continuous medication infusions.

Dückers et al
Safety and risk management in hospitals
18
3. Results
Structured order sheet
Kozer et al (2005) concluded that a structured order sheet (a standardised order sheet containing a number of pre-structured information categories) is effective in reducing the incidence of medication errors in paediatric emergency departments. The intervention group used a new structured order sheet instead of the regular blank order sheets, which resulted in a statistically significant reduction.
The Breakthrough Series
Silver and Antonow (2000) conducted an evaluation of the Breakthrough Series (described on page 14). Analysis of this model, which used a collaborative approach to increase knowledge among teams of staff, demonstrated a significant decrease in overall error frequency and a significant increase in error detection and prevention.
Failure mode and effect analysis
The FMEA conducted by Robinson et al (2006) has also been described earlier (see page 15). After the implementation of improvement strategies, which resulted from the analysis, improvements were achieved in the potential prescribing error rate, actual dispensing errors and actual administration errors. The use of pre-printed standard order sets increased.
Reducing the number and severity of fall incidents
Multi-component falls prevention programmes
Five of the seven studies addressing interventions to reduce the number and/or severity of fall incidents are multi-component falls prevention programmes. Dempsey (2004) and Donoghue et al (2005) both reported positive results. Dempsey tested a falls prevention programme in an acute medical area, which was re-evaluated five years later to determine if the effects had been sustained. The conclusion was that the number of falls reduced by 55 per cent between 1995 and 1996. In 2001, the rate of patient falls had exceeded pre-research levels. Donoghue et al carried out research to find out whether a companion observer programme helped to prevent high-risk inpatients on an acute aged care ward from falling. Patients at high risk were accompanied in a room staffed by volunteer companion observers. The 128 observers worked in two-hour shifts, on weekdays from 8.00am to 8.00pm. Their primary objective was to keep patients company and to notice if they became increasingly agitated or showed risky behaviour. If this was the case, then they gently reassured the patient and, if necessary, contacted a nurse. The fall rate decreased by 44 per cent.
Another programme proved partly effective. Williams et al (2007) evaluated a systematic, co-ordinated approach to limit the severity and minimise the number of falls in an acute care hospital. Patients were classified according to three levels of risk: low, medium and high. Appropriate interventions (environment, mobility, elimination) were developed for each risk level on a fall care plan for each patient. Analysis showed a significant reduction in the number of falls (9.5 per 1,000 occupied bed days before and 8.0 per 1,000 occupied bed days after), although not in the severity of falls.
In the remaining studies, the intended decrease was not detected. Schwendimann et al (2006) examined an interdisciplinary falls prevention programme based on:
1. screening of all patients at admission for risk of falls
2. examination of patients considered at risk of falling
3. interventions for all patients to provide safety in the hospital
4. interventions for patients considered at risk of falling
5. reassessment of those patients who fell.

Dückers et al
Safety and risk management in hospitals
19
3. Results
After the implementation, a decrease in falls was observed, but this was not significant. There were no considerable differences over time in individual departments, and the annual proportion of minor and major injuries did not decrease. Lane (1999) evaluated the effectiveness of a falls prevention programme in reducing the patient fall rate. The programme also identified patients at risk of falling and established guidelines for interventions promoting patient safety. However, the study reported an insignificant change in patient fall rate per 1,000 patients days and an insignificant decrease in injuries.
Other interventions
In a falls prevention interventions review, Gillespie et al (2003) extracted two other studies, which did not deal with a falls prevention programme, but with different interventions. Donald et al (2000) compared two flooring types – carpet and vinyl – in hospital bed areas, and two types of physiotherapy – conventional therapy and additional leg strengthening exercises – in avoiding falls. No significant effect was found for either intervention. Tideiksaar et al (1993) examined the clinical efficacy of a bed alarm system in reducing falls from bed on a geriatric evaluation and treatment unit. The system functioned effectively, activating an alarm in all cases when patients were transferring from their bed and, with the exception of one case, nurses could respond quickly to help patients and prevent bed falls. Although there was a clinical trend towards reduced falls in the experimental group, this was not significant enough to make a statistical difference in bed falls between the experimental group with the bed alarm system and the four control groups.
Reducing diagnostic errors
A third category of outcomes was the reduction in diagnostic errors. Two studies about reminder systems were included, with both reporting significant improvements. Ramnarayan et al (2006a) examined the impact of a web-based diagnostic reminder system on clinicians’ decisions in an acute paediatric setting during assessments that were characterised by diagnostic uncertainty. After the introduction of the diagnostic computerised decision support system, the percentage of unsafe diagnostic workups decreased significantly from 45.2 per cent to 32.7 per cent. Ramnarayan et al (2006b) assessed the impact of a diagnostic reminder system on the quality of clinical decisions made by various grades of clinicians during acute assessment. The mean count of diagnostic errors of omission decreased significantly, and the mean diagnostic quality score increased. The number of irrelevant diagnoses increased from 0.7 to 1.4, but did not result in a corresponding increase in the number of irrelevant or deleterious tests and treatments.
Reducing the number and severity of adverse events and risks
Four studies fit within this category. The review of institutional reporting systems by Simon et al (2005) has been discussed on page 13. In this review the authors also assessed the effectiveness of reporting systems as an SRM intervention to improve safety and reduce risks. The majority (7 out of 11) of the included studies reported no reduction in medical errors and adverse events after implementing incident reporting systems.
The three other studies mainly reported positive results. A wide variety of approaches has been studied in attempts to reduce the number and severity of adverse events and risks, using information and communication technology (ICT) programmes, FMEA or multi-component intervention packages.
Fraenkel et al (2003) described the effects of a computerised clinical information system, implemented in an intensive care unit. Significant reductions occurred in the following incidents: medication, intravenous, ventilation and other incidents.

Dückers et al
Safety and risk management in hospitals
20
3. Results
Jain et al (2006) reported a variety of positive results. They evaluated a combination of different interventions that were implemented individually over a 12-month period, including:
• multidisciplinary rounds led by doctors
• daily bed-flow meetings to access bed availability
• evidence-based practices relating to three quality initiatives
• culture change, with a forum on team decision-making.
In a third study, the number of patient attendances associated with an adverse event decreased significantly between the first and last quarter of the study year (Wolff and Bourke 2002). Retrospective screening of patient files took place in two phases. After three months, several interventions were implemented:
• a variety of actions aimed at preventing events from recurring (changes in hospital policies, focused auditing, discussion with staff, implementation of guidelines)
• weekly adverse event reports/quarterly reports
• encouragement of staff to report clinical incidents.
In the light of the findings of the studies in this category, it is important to emphasise that the number of adverse events is generally an unreliable patient safety measure as the risk of under-reporting is substantial.
Other safety or risk effects
While most of the studies could be organised into the following categories: adverse events in general, medication errors, fall incidents, and diagnostic errors, one study could not be categorised in this way. DeVita et al (2005) found that simulated survival rates improved significantly after human simulation training in an educational environment to develop multidisciplinary team skills. The course components were:
• a web-based presentation and pre-test before the course
• a brief reinforcing training session on the day of the course
• three out of five different simulated scenarios, each followed by debriefing and analysis with the team.

Dückers et al
Safety and risk management in hospitals
21
4. Discussion
4. Discussion
The primary study objectives of this review were:
1. to synthesise the evidence on the effectiveness of detection, mitigation and actions to reduce risks in hospitals; and
2. to identify and describe the components of interventions that are responsible for effectiveness.
The study covered a wide variety of conditions and interventions related to safety and risks. We categorised the collected studies within different safety and risk management (SRM) interventions, as part of the International Classification for Patient Safety (ICPS) framework (see Box 1and page 3 and Figure 1 on page 4).
Main findingsDetection
The first type of intervention is detection. All the studies we included that deal with incident reporting (incident reporting systems, intervention packages, the Breakthrough Series, and efforts by a multidisciplinary team) indicate a positive effect of the interventions on the quality and/or quantity of reports. Most of the research on detection addresses reporting systems. When identifying the effective components of these systems, one finding is that voluntary incident reporting may lead to under-reporting (Plews-Ogan et al 2004). The total error rate was higher in studies using voluntary reporting than in a study using mandatory reporting (Snijders et al 2007). In practice, nurses report considerably more events than do doctors (Simon et al 2005; Harris et al 2007). Feedback to the reporter is seen as an important factor in safeguarding the willingness of staff to continue to report incidents and near misses (Simon et al 2005). In the case of neonatology, Snijders et al (2007) found that multi-institutional reporting identified uncommon but relevant errors. Moreover, Harris et al (2007) concluded that paper-based reporting sometimes works better than a web-based tool. The effective components of the other interventions to advance reporting are part of a larger intervention package, which therefore makes it impossible to disentangle the effective components from the whole programme.
A second detection activity concerns analysis methods. Despite a large number of papers devoted to this subject, research addressing the effectiveness and efficiency of safety analysis is scarce (see also Vincent 2004). There are indications that analysis techniques are effective in identifying potential risks or root causes, and in monitoring changes. One study by Robinson et al (2006), which had a weak design, shows that applying an FMEA has positive results, although information about which method works best in which circumstances – in terms of effectiveness, efficiency, accuracy and reliability – was not provided.
Actions to reduce risk
No studies on mitigating factors were identified. The majority of the studies, which were also those with the strongest study designs, dealt with actions to reduce risk. The collected evidence contributes to the knowledge about what works in general in reducing the number and severity of medication errors, fall incidents, diagnostic errors and adverse events. Unfortunately, however, it often remains unclear what the effective component was and why it worked. This is because SRM interventions are embedded in the structure and process of healthcare organisations. Furthermore, the diversity of the collected material, combined with the limited evidence for each topic, makes it difficult to draw generic conclusions or to conduct a quantitative meta analysis.

Dückers et al
Safety and risk management in hospitals
22
4. Discussion
Resilience
Resilience is the degree to which a system continuously prevents, detects, mitigates or ameliorates hazards or incidents so that an organisation can ‘bounce back’ to its original ability to provide core functions (see Box 1 on page 3). Within the context of ‘resilience’, SRM is linked to implementation science and concepts such as continuous quality improvement, cyclical quality management systems, and organisational learning. Improving safety and risk reduction, based on collected information about incidents and risks, or analysis results, requires some sort of learning or feedback mechanism. The study by Robinson et al (2006) provides a case in which analysis results were used as input for improvement. However, Simon et al (2005) concluded that many of the studies in their review on institutional reporting systems suffered from a flaw: that they are based on the assumption that incident data will automatically improve safety performance by directing system or institutional interventions, and by affecting health provider knowledge and skills via feedback.
In many of the studies included in our review, the relationship between detection, mitigation and risk reduction actions could not be verified. A general conclusion is that the initiation of reporting systems is likely to contribute to an increase in the number of reports. The real challenge, however, relates not to the quantity or quality of reports but to the degree to which professionals or organisations use the collected information to generate improvement. Feedback is considered a conditio sine qua non for learning and, thus, for continuous SRM. Still, the practical feasibility of feedback must be considered with some reservations. There is limited evidence about effective forms of safety feedback within healthcare (Benn et al 2009), and a Cochrane review of audit and feedback, which included more than 100 trials, showed a very modest improvement in professional performance overall (Jamtvedt et al 2006).
LimitationsThere are several reasons to view the findings of the studies we reviewed with caution and to question their usefulness in initiatives that translate them to new settings. These reasons are set out below:
• It seems highly probable that the published research on SRM has a substantial publication bias. Almost 90 per cent of the studies included in our review reported positive results.
• More than two-thirds of the included studies were of a low methodological quality. The available research is mainly comprised of uncontrolled observational evaluations. In many of the studies, the sample size was relatively small, and details were described poorly. This therefore limited the ability of the researchers to determine whether patients with particular characteristics – for example, age or morbidity – were more or less likely to respond to, for example, fall incident or medication safety interventions. In particular, the effects reported in the UBAs should be interpreted with caution.
• Interventions were often embedded in multifaceted intervention packages or programmes. In these cases, it was not possible to isolate the impact of specific components from other activities and conditions. This is not necessarily problematic, but it does make it challenging to determine what exactly caused an effect, or lack of effect.
• Most studies provided limited information on the costs relating to the intervention. Without this information, policy-makers, programme designers, managers and/or professionals cannot make informed decisions about the costs and benefits of improvement schemes.
• By taking ‘safety and risk management’ as a starting point, this review identified research linked to this term in the literature. Such an open approach allowed us to obtain a general sense of reference and guidance, instead of directly focusing on specific applications. This is an explorative approach, in which the term itself defines the scope. However, as a result, not all of the safety research performed in the context of quality improvement has been included.

Dückers et al
Safety and risk management in hospitals
23
4. Discussion
We therefore recommend extending the search strategy of future literature studies by using key phrases from the evolving ICPS framework. Our decision to select studies with strong research designs follows from the study objectives, but this means that relevant information from studies not meeting this threshold was excluded. As a result, only a selection of safety items were presented in this review, while highly relevant items such as infection control were omitted.
Future researchEffectiveness detection
By linking our review to the ICPS framework, we have the opportunity to locate gaps in the international literature on SRM. Most of the evidence discussed in this review affects detection and risk reduction measures. Researchers need to feel encouraged to proceed with the evaluation of the effectiveness of these and other detection interventions. In particular, we recommend the further assessment and comparison of analysis techniques (and their role as a window on the system – see, for example, Vincent 2004). It is important to learn more about their effectiveness, efficiency and accuracy. One way of exploring this area tentatively is for experts with practical experience of particular analysis methods to analyse the same incident (in the case of causes) or process (in the case of failure modes) and study whether their findings are similar. If they are, research could identify whether differences found can be attributed to the method or way the analysis was conducted. In this way, it may be possible to decide whether the result of an applied risk analysis method depends on the type of analysis or on the presence of specific conditions during the implementation. Likewise, the impact of analysis techniques may be best studied in combination with safety improvement interventions.
Continuous safety and risk management and resilience
Although the poor availability of material on mitigation is interesting, it is in the area of continuous SRM and resilience where we perceive the greatest need for original and system-oriented evaluations of effectiveness. How do SRM interventions contribute to continuous learning? Testable hypotheses can be formulated in relation to positive influences of various SRM approaches and conditions within hospitals, such as:
• the application of integrated safety frameworks
• organisational culture
• safety culture
• leadership styles
• guidelines
• performance management
• continuous quality improvement techniques
• multidisciplinary teams joining a quality improvement collaborative.
Although high expectations are often raised, in the current review no evidence on these topics was found in relation to SRM outcomes. This finding reflects that of other studies: for example, the research evidence concerning collaboratives (Schouten et al 2008), as well as the low number of studies identified by Hoff et al (2004) that verify the relationship between organisational features and patient safety. Compared with the review by Hoff et al, which focused on conditions, our emphasis on interventions resulted in a relatively large number of studies describing positive effects on safety and risk outcomes. Nevertheless, the possibilities for future research are enormous.

Dückers et al
Safety and risk management in hospitals
24
4. Discussion
Combined safety and risk management and implementation science
There is currently a substantial body of research on organisational changes in healthcare settings, but quality and safety systems have seldom been studied in rigorous evaluations, so their effectiveness remains unproven (Wensing et al 2006). Authors of studies identified in this review have highlighted the importance of follow-up measurements and the issue of sustainability (Dempsey 2004; Kozer et al 2005), and sustainability of implementation outcomes and changed practices is a highly relevant research area (Greenhalgh et al 2005; Grol et al 2007). We strongly recommend that research on the improvement of patient safety links to, and builds on, the extensive and rich world of quality improvement research and implementation science (Grol et al 2008). For example, it is not clear whether and how knowledge about the success and failure of the implementation of SRM interventions is used in dissemination decisions locally, nationally or internationally (in the case of effect studies published in international journals). Dissemination without a good understanding of the idiosyncrasies of a particular innovation may be a waste of time or may even be counterproductive.
Expanding and improving safety and risk management research
A conclusion that can be drawn from this review is that it is surprising – given the international attention focusing on patient safety – that the evidence base for SRM in a hospital setting is so limited. SRM needs to be approached like any intervention in healthcare in that it should prove its effectiveness – and cost effectiveness – before wide implementation is promoted. At this point, the number and quality of published studies on SRM interventions is too small to support conclusions about effectiveness in a systems perspective. Therefore, considerable expansion and improvement in research on SRM is much needed and would be of great value.

Dückers et al
Safety and risk management in hospitals
25
References
References
Benn J, Koutanji M, Wallace L et al (2009). ‘Feedback from incident reporting: Information and action to improve patient safety’ Quality and Safety in Healthcare, vol 18, pp 11–21.
Berner ES, Houston TK, Ray MN et al (2006). ‘Improving ambulatory prescribing safety with a handheld decision support system: a randomized controlled trial’. Journal of the American Medical Informatics Association (JAMIA), vol 13, pp 171–179.
Bonnabry P, Cingria L, Sadeghipour F et al (2005). ‘Use of a systematic risk analysis method to improve safety in the production of paediatric parenteral nutrition solutions’. Quality and Safety in Health Care, vol 14, pp 93–98.
Cohen MM, Kimmel NL, Benage MK et al (2005). ‘Medication safety program reduces adverse drug events in a community hospital’. Quality and Safety in Health Care, vol 14, pp 169–174.
Dempsey J (2004). ‘Falls prevention revisited: a call for a new approach’. Journal of Clinical Nursing, vol 13, pp 479–485.
DeVita MA, Schaefer J, Lutz J et al (2005). ‘Improving medical emergency team (MET) performance using a novel curriculum and a computerized human patient simulator’. Quality and Safety in Health Care, vol 14, pp 326–331.
Donald IP, Pitt K, Armstrong E et al (2000). ‘Preventing falls on an elderly care rehabilitation ward’. Clinical Rehabilitation, vol 14, pp 178–185.
Donoghue J, Graham J, Mitten-Lewis S et al (2005). ‘A volunteer companion-observer intervention reduces falls on an acute aged care ward’. International Journal of Health Care Quality Assurance Incorporating Leadership in Health Services, vol 18, pp 24–31.
Elder NC, Pallerla H and Regan S (2006). ‘What do family physicians consider an error? A comparison of definitions and physician perception’. BMC Family Practice, vol 7, p 73.
Evans SM, Smith BJ, Esterman A et al (2007). ‘Evaluation of an intervention aimed at improving voluntary incident reporting in hospitals’. Quality and Safety in Health Care, vol 16, pp 169–175.
Fallowfield LJ and Fleissig A (2004). ‘Communication with patients in the context of medical error’. Health Care Risk Special Report, vol 10, pp 12–14.
Fertleman M, Barnett N and Patel T (2005). ‘Improving medication management for patients: the effect of a pharmacist on post-admission ward rounds’. Quality and Safety in Health Care, vol 14, pp 207–211.
Fraenkel DJ, Cowie M and Daley P (2003). ‘Quality benefits of an intensive care clinical information system’. Critical Care Medicine, vol 31, pp 120–125.
Gillespie LD, Gillespie WJ, Robertson MC et al (2003). ‘Interventions for preventing falls in elderly people. Cochrane Database of Systematic Reviews, Issue 4, Art no. CD000340.

Dückers et al
Safety and risk management in hospitals
26
References
Greenhalgh T, Robert G, Bate P et al (2005). Diffusion of innovations in Health Service Organisations: a systematic literature review. London: Blackwell Publishing.
Grol R, Berwick DM and Wensing M (2008). ‘On the trail of quality and safety in health care’. British Medical Journal, vol 336, pp 74–76.
Grol R, Bosch MC, Hulscher MEJL et al (2007). ‘Planning and studying improvement in patient care: the use of theoretical perspectives’. Milbank Quarterly, vol 85, pp 93–138.
Harris CB, Krauss MJ, Coopersmith CM et al (2007). ‘Patient safety event reporting in critical care: a study of three intensive care units’. Critical Care Medicine, vol 35, pp 1,068–1,076.
Hoff T, Jameson L, Hannan E et al (2004). ‘A review of the literature examining linkages between organizational factors, medical errors, and patient safety’. Medical Care Research and Review, vol 61, pp 3–37.
Institute of Medicine (2000). To err is human: building a safer health system. Washington DC: National Academy Press.
Jain M, Miller L, Belt D et al (2006). ‘Decline in ICU adverse events, nosocomial infections and cost through a quality improvement initiative focusing on teamwork and culture change’. Quality and Safety in Health Care, vol 15, pp 235–239.
Jamtvedt G, Young JM, Kristoffersen DT et al (2006). ‘Audit and feedback: effects on professional practice and health care outcomes’. Cochrane Database of Systematic Review, Issue 2, Art no. CD000259.
King WJ, Paice N, Rangrej J et al (2003). ‘The effect of computerized physician order entry on medication errors and adverse drug events in pediatric inpatients’. Pediatrics, vol 112, pp 506–509.
Kozer E, Scolnik D, MacPherson A et al (2005). ‘Using a preprinted order sheet to reduce prescription errors in a pediatric emergency department: a randomized, controlled trial’. Pediatrics, vol 116, pp 1,299–1,302.
Lane AJ (1999). ‘Evaluation of the fall prevention program in an acute care setting’. Orthopaedic Nursing, vol 18, pp 37–43.
Larsen GY, Parker HB, Cash J et al (2005). ‘Standard drug concentrations and smart-pump technology reduce continuous-medication-infusion errors in pediatric patients’. Pediatrics, vol 116, e21–e25.
Leape LL, Cullen DJ, Clapp MD et al (1999). ‘Pharmacist participation on physician rounds and adverse drug events in the intensive care unit’. Journal of the American Medical Association, vol 282, pp 267–270.
Leape LL, Lawthers AG, Brennan TA et al (1993). ‘Preventing medical injury’. Quality Review Bulletin, vol 19, pp 144–149.

Dückers et al
Safety and risk management in hospitals
27
References
Lehmann DF, Page N, Kirschman K et al (2007). ‘Every error a treasure: improving medication use with a nonpunitive reporting system’. Joint Commission Journal on Quality and Patient Safety, vol 33, pp 401–407.
Manning DM, O’Meara JG, Williams AR et al (2007). ‘3D: a tool for medication discharge education’. Quality and Safety in Health Care, vol 16, pp 71–76.
MeSH (2009). Available at www.nlm.nih.gov/mesh/MBrowser.html. Accessed 29 August 2009.
Øvretveit J (2008). Which interventions are effective for improving patient safety? A synthesis of research and policy issues. Copenhagen/Stockholm: WHO HEN/MMC Karolinska.
Paoletti RD, Suess TM, Lesko MG et al (2007). ‘Using bar-code technology and medication observation methodology for safer medication administration’. American Journal of Health-System Pharmacy, vol 64, pp 536–543.
Plews-Ogan ML, Nadkarni MM, Forren S et al (2004). ‘Patient safety in the ambulatory setting. A clinician-based approach’. Journal of General Internal Medicine, vol 19, pp 719–725.
Poon EG, Cina JL, Churchill W et al (2006). ‘Medication dispensing errors and potential adverse drug events before and after implementing bar code technology in the pharmacy’. Annals of Internal Medicine, vol 145, pp 426–434.
Ramnarayan P, Roberts GC, Coren M et al (2006a). ‘Assessment of the potential impact of a reminder system on the reduction of diagnostic errors: a quasi-experimental study’. BMC Medical Informatics and Decision Making, vol 6, p 22.
Ramnarayan P, Winrow A, Coren M et al (2006b). ‘Diagnostic omission errors in acute paediatric practice: impact of a reminder system on decision-making’. BMC Medical Informatics and Decision Making, vol 6, p 37.
Robinson DL, Heigham M and Clark J (2006). ‘Using Failure Mode and Effects Analysis for safe administration of chemotherapy to hospitalized children with cancer’. Joint Commission Journal on Quality and Patient Safety, vol 32, pp 161–166.
Runciman WB, Williamson JAH, Deakin A et al (2006). ‘An integrated framework for safety, quality and risk management: an information and incident management system based on a universal patient safety classification’. Quality and Safety in Health Care, vol 15, i82–i90.
Runciman W, Hibbert P, Thomson R et al (2009). ‘Towards an International Classification for Patient Safety: key concepts and terms’. International Journal for Quality in Health Care, vol 21, pp 18–26.
Schneider PJ, Pedersen CA, Montanya KR et al (2006). ‘Improving the safety of medication administration using an interactive CD-ROM program’. American Journal of Health-System Pharmacy, vol 63, pp 59–64.
Schouten LMT, Hulscher MEJL, Van Everdingen JJE et al (2008). ‘Evidence for the impact of quality improvement collaboratives: systematic review’. British Medical Journal, vol 336, pp 1,491–1,494.

Dückers et al
Safety and risk management in hospitals
28
References
Schwendimann R, Buhler H, De Geest S et al (2006). ‘Falls and consequent injuries in hospitalized patients: effects of an interdisciplinary falls prevention program’. BMC Health Services Research, vol 6, p 69.
Shamliyan TA, Duval S, Du J et al (2008). ‘Just what the doctor ordered. Review of the evidence of the impact of computerized physician order entry system on medication errors’. Health Services Research, vol 43, pp 32–53.
Sherman H, Castro G, Fletcher M et al (2009). ‘Towards an International Classification for Patient Safety: the conceptual framework’. International Journal for Quality in Health Care, vol 21, pp 2–8.
Silver MP and Antonow JA (2000). ‘Reducing medication errors in hospitals: a peer review organization collaboration’. Joint Commission Journal on Quality and Patient Safety, vol 26, pp 332–340.
Sim TA and Joyner J (2002). ‘A multidisciplinary team approach to reducing medication variance’. Joint Commission Journal on Quality and Patient Safety, vol 28, pp 403–409.
Simon A, Lee RC, Cooke DL et al (2005). Institutional medical incident reporting systems: a review. Alberta: AHFMR, Health Technology Assessment Unit.
Simpson JH, Lynch R, Grant J et al (2004). ‘Reducing medication errors in the neonatal intensive care unit’. Archives of Disease in Childhood: Fetal and Neonatal Edition, vol 89, F480–F482.
Snijders C, van Lingen RA, Molendijk A et al (2007). ‘Incidents and errors in neonatal intensive care: a review of the literature’. Archives of Disease in Childhood: Fetal and Neonatal Edition, vol 92, F391–F398.
Stump LS (2000). ‘Re-engineering the medication error-reporting process: removing the blame and improving the system’. American Journal of Health-System Pharmacy, vol 57, Suppl 4, S10–S17.
Thomson R, Lewalle P, Sherman H et al (2009). ‘Towards an International Classification for Patient Safety: a Delphi survey’. International Journal for Quality in Health Care, vol 21, pp 9–17.
Tideiksaar R, Feiner CF and Maby J (1993). ‘Falls prevention – the efficacy of a bed alarm system in an acute-care setting’. Mount Sinai Journal of Medicine, vol 60, pp 522–527.
Voeffray M, Pannatier A, Stupp R et al (2006). ‘Effect of computerisation on the quality and safety of chemotherapy prescription’. Quality and Safety in Health Care, vol 15, pp 418–421.
Vincent C (2004). ‘Analysis of clinical incidents: a window on the system not a search for root causes’. Quality and Safety in Health Care, vol 13, pp 242–243.
Walsh KE, Landrigan CP, Adams WG et al (2008). ‘Effect of computer order entry on prevention of serious medication errors in hospitalized children’. Pediatrics, vol 121, e421–e427.
Wensing M, Wollersheim H and Grol R (2006). ‘Organisational interventions to implement improvements in patient care: a structured review of reviews’. BMC Implementation Science, vol 1, p 2.

Dückers et al
Safety and risk management in hospitals
29
References
Williams TA, King G, Hill AM et al (2007). ‘Evaluation of a falls prevention programme in an acute tertiary care hospital’. Journal of Clinical Nursing, vol 16, pp 316–324.
Wilson RM, Runciman WB, Gibberd RW et al (1996). ‘Quality in Australian health care study’. Medical Journal of Australia, vol 164, p 754.
Wolff AM and Bourke J (2002). ‘Detecting and reducing adverse events in an Australian rural base hospital emergency department using medical record screening and review’. Emergency Medical Journal, vol 19, pp 35–40.
Woloshynowych M, Rogers S, Taylor-Adams S et al (2005). ‘The investigation and analysis of critical incidents and adverse events in healthcare’. Health Technology Assessment, vol 9, pp 1–143.
World Health Organization, World Alliance for Patient Safety (2009). The conceptual framework for the International Classification for Patient Safety. Geneva: World Health Organization.

Dückers et al
Safety and risk management in hospitals
30
Appendix A: Example of a search strategy and results
Appendix A: Example of a search strategy and results
Search results: PubMed, 29 May 2008
Search term No. of hits
#1 ‘medical error’ [text word] 517
#2 ‘medical errors’ [text word] 7,480
#3 ‘medical errors’ [MeSH] 57,441
#4 1 OR 2 OR 3 57,871
#5 ‘incident’ [text word] 22,827
#6 ‘incidents’ [text word] 7,670
#7 5 OR 6 29,138
#8 ‘adverse event’ [text word] 6,182
#9 ‘adverse events’ [text word] 31,743
#10 8 OR 9 35,427
#11 ‘near miss’ [text word] 468
#12 ‘near misses’ [text word] 237
#13 11 OR 12 653
#14 4 OR 7 OR 10 OR 13 121,257
#15 ‘risk management’ [text word] 12,602
#16 ‘risk management’ [MeSH] 107,835
#17 15 OR 16 109,272
#18 ‘safety management’ [text word] 8,952
#19 ‘safety management’ [MeSH] 8,788
#20 18 OR 19 8,952
#21 17 OR 20 109,398
#22 ‘hospital’ [text word] 610,365
#23 ‘hospitals’ [text word] 224,372
#24 ‘hospitals’ [MeSH] 156,732
#25 22 OR 23 OR 24 714,103
#26 14 AND 21 AND 25 2,694
#27 EPOC filter (see Appendix B) 7,422,048
#28 26 AND 27 1,197

Dückers et al
Safety and risk management in hospitals
31
Appendix B: EPOC methodological filter
Appendix B: EPOC methodological filter
Randomized Controlled Trial [publication type] OR Controlled Clinical Trial [publication type] OR Comparative Study OR Evaluation Studies OR ‘comparative study’ OR ‘effects’ OR ‘effect’ OR ‘evaluations’ OR ‘evaluating’ OR ‘evaluation’ OR ‘evaluates’ OR ‘changing’ OR ‘changes’ OR ‘change’ OR ‘interventions’ OR ‘intervention’ OR ‘impact’ OR ‘random allocation’ OR ‘post test’ OR ‘posttest’ OR ‘pre test’ OR ‘pretest’ OR ‘time series’ OR ‘experimental’ OR ‘experiments’ OR ‘experiment’ OR ‘intervention studies’ OR ‘intervention study’ OR ‘controlled clinical trial’ OR ‘randomised controlled trial’ OR ‘randomized controlled trial’
Source: The Cochrane Effective Practice and Organisation of Care (EPOC) Group

Dückers et al
Safety and risk management in hospitals
32
Appendix C: Study topics and interventions per SRM activity
Dückers et al
Safety and risk management in hospitals
33
Appendix C: Study topics and interventions per SRM activity
Ap
pen
dix
C: S
tud
y to
pic
s an
d in
terv
enti
on
s p
er S
RM
act
ivit
y, s
ort
ed b
y d
esig
n
Act
ivit
yS
RM
top
icR
evie
wR
CT
CB
AIT
SU
BA
Inte
rven
tio
n
1D
etec
tio
n2
01
33
Qua
ntity
and
qua
lity
of
repo
rts
+-
--
-In
stitu
tiona
l med
ical
inci
dent
rep
ortin
g sy
stem
s (S
imon
et a
l 20
05)*
+-
--
-C
hara
cter
istic
s of
inci
dent
rep
ortin
g sy
stem
s (S
nijd
ers
et a
l 20
07)
Num
ber o
f rep
orts
--
+-
-In
terv
entio
n pa
ckag
e: e
duca
tion,
a r
ange
of r
epor
ting
optio
ns, e
nhan
ced
repo
rt m
anag
emen
t an
d fe
edba
ck (
Eva
ns e
t al 2
007
)
--
-+
-N
ew, v
olun
tary
, car
d-ba
sed
even
t rep
ortin
g sy
stem
(H
arris
et a
l 20
07)
--
-+
-R
evis
ed, n
on-p
uniti
ve m
edic
atio
n ev
ent r
epor
ting
polic
y (L
ehm
ann
et a
l 20
07)
--
-+
-C
hang
ing
the
trad
ition
al, m
ulti-
tiere
d in
cide
nt r
epor
ting
syst
em fo
r med
icat
ion
erro
rs to
a
stan
dard
ised
, non
-pun
itive
med
icat
ion-
use
varia
nce
proc
ess
(Stu
mp
200
0)
--
--
+V
olun
tary
nea
r mis
s/ad
vers
e ev
ent r
epor
ting,
com
bine
d w
ith s
yste
m a
naly
sis
and
rede
sign
(P
lew
s-O
gan
et a
l 20
04)
--
--
+B
reak
thro
ugh
Ser
ies
to r
educ
e m
edic
atio
n er
rors
(S
ilver
and
Ant
onow
20
00
)*
--
--
+M
ultid
isci
plin
ary
team
add
ress
ing
med
icat
ion-
rela
ted
patie
nt s
afet
y in
itiat
ives
: num
ber o
f va
rianc
e re
port
s (S
im a
nd J
oyne
r 20
02)
2M
itig
atin
g f
acto
rs0
00
00
3A
ctio
ns
to r
edu
ce r
isk
26
36
14
Adv
erse
eve
nts
(uns
peci
fied)
+-
--
-In
stitu
tiona
l med
ical
inci
dent
rep
ortin
g sy
stem
s (S
imon
et a
l 20
05)*
--
-+
-C
linic
al in
form
atio
n sy
stem
(F
raen
kel e
t al 2
003
)
--
--
+Te
amw
ork
and
cultu
re c
hang
e (J
ain
et a
l 20
06
)
--
--
+U
se o
f FM
EA
to id
entif
y ris
k, a
nd fo
r im
plem
entin
g st
rate
gies
(R
obin
son
et a
l 20
06
)
--
--
+R
etro
spec
tive
med
ical
-rec
ord
scre
enin
g an
d cl
inic
al r
evie
w fo
llow
ed b
y ap
prop
riate
qua
lity
impr
ovem
ent a
ctio
ns (
Wol
ff a
nd B
ourk
e 20
02)
Med
icat
ion
erro
rs/a
dver
se
drug
eve
nts
+-
--
Com
pute
risat
ion
of p
hysi
cian
ord
ers:
pre
scrip
tion
(Sha
mliy
an e
t al 2
008
)
-+
--
-D
ecis
ion
supp
ort t
ool o
n pe
rson
al d
igita
l ass
ista
nt (
Ber
ner e
t al 2
00
6)
-+
--
-S
truc
ture
d or
der s
heet
(K
ozer
et a
l 20
05)
-+
--
-N
ew w
eb-b
ased
edu
catio
n to
ol c
ompa
red
with
a s
tand
ard
educ
atio
n to
ol (
Man
ning
et a
l 20
07)

Dückers et al
Safety and risk management in hospitals
32
Appendix C: Study topics and interventions per SRM activity
Dückers et al
Safety and risk management in hospitals
33
Appendix C: Study topics and interventions per SRM activity
-+
--
-In
tera
ctiv
e C
D-R
OM
pro
gram
me
(Sch
neid
er e
t al 2
00
6)
--
+-
-C
ompu
teris
ed p
hysi
cian
ord
er e
ntry
sys
tem
with
out c
linic
al d
ecis
ion
supp
ort (
Kin
g et
al 2
003
)
--
+-
-P
harm
acis
t par
ticip
atio
n in
the
ICU
at t
he ti
me
of d
rug
pres
crib
ing
(Lea
pe e
t al 1
999
)
--
+-
-O
bser
vatio
n m
etho
dolo
gy a
nd e
lect
roni
c m
edic
atio
n re
cord
s: b
ar-c
ode
tech
nolo
gy
(Pao
lett
i et a
l 20
07)
--
-+
-O
rgan
isat
ion-
wid
e sa
fety
pro
gram
me
(Coh
en e
t al 2
005
)
--
-+
-C
ombi
ned
risk
man
agem
ent/
clin
ical
pha
rmac
ist-
led
educ
atio
n pr
ogra
mm
e
(Sim
pson
et a
l 20
04)
--
-+
-C
ompu
teris
ed p
hysi
cian
ord
er e
ntry
sys
tem
(V
oeff
ray
et a
l 20
06
)
--
-+
-C
ompu
teris
ed p
hysi
cian
ord
er e
ntry
sys
tem
, che
ck d
osag
e w
ith a
lert
func
tion
(W
alsh
et a
l 20
08)
--
--
+P
harm
acis
t par
ticip
atio
n on
pos
t-ad
mis
sion
war
d ro
unds
(F
ertle
man
et a
l 20
05)
--
--
+C
ombi
ning
sta
ndar
d dr
ug c
once
ntra
tions
with
sm
art-
pum
p te
chno
logy
: inf
usio
n
(Lar
sen
et a
l 20
05)
--
--
+B
ar-c
ode
tech
nolo
gy (
disp
ensi
ng e
rror
s an
d po
tent
ial A
DE
s (P
oon
et a
l 20
06
)
--
--
+B
reak
thro
ugh
Ser
ies
to r
educ
e m
edic
atio
n er
rors
(S
ilver
and
Ant
onow
20
00
)*
Sev
erity
and
/or n
umbe
r of
fall
inci
dent
s-
+-
--
Com
paris
on o
f car
pet a
nd v
inyl
floo
ring
type
s in
bed
are
as a
nd tw
o ty
pes
of p
hysi
othe
rapy
(D
onal
d et
al 2
00
0)
-+
--
-B
ed a
larm
sys
tem
(T
idei
ksaa
r et a
l 199
3)
--
-+
-In
terd
isci
plin
ary
falls
pre
vent
ion
prog
ram
me
(Sch
wen
dim
ann
et a
l 20
06
)
--
--
+C
ompa
nion
obs
erve
r pro
gram
me,
bas
ed o
n 12
8 vo
lunt
eer o
bser
vers
(D
onog
hue
et a
l 20
05)
--
--
+F
all r
isk
asse
ssm
ent a
nd p
reve
ntio
n pr
ogra
mm
e (D
emps
ey 2
004
)
--
--
+F
alls
pre
vent
ion
prog
ram
me
(Lan
e 19
99)
--
--
+S
yste
mat
ic, c
o-o
rdin
ated
app
roac
h (W
illia
ms
et a
l 20
07)
Dia
gnos
tic e
rror
s-
--
-+
Web
-bas
ed d
iagn
ostic
rem
inde
r sys
tem
on
clin
icia
ns’ d
ecis
ions
(R
amna
raya
n et
al 2
00
6a)
--
--
+C
ompu
teris
ed d
ecis
ion
supp
ort (
a di
agno
stic
rem
inde
r sys
tem
) ((R
amna
raya
n et
al 2
00
6b)
Sim
ulat
ed s
urvi
val r
ates
--
--
+H
uman
sim
ulat
ion
trai
ning
/edu
catio
nal e
nviro
nmen
t to
deve
lop
team
ski
lls (
DeV
ita e
t al 2
005
)
* In
clud
ed m
ore
than
onc
e in
this
tabl
e
AD
E =
adv
erse
dru
g ev
ent
FM
EA
= fa
ilure
mod
e an
d ef
fect
s an
alys
is
ICU
= in
tens
ive
care
uni
t.

Dückers et al
Safety and risk management in hospitals
34
Appendix D: Quality of study design
Dückers et al
Safety and risk management in hospitals
35
Appendix D: Quality of study design
Des
ign
Fir
st a
uth
or
A1
A2
A3
A4
A5
B1
B2
CD
1D
2E
FG
1G
2H
IJ
KL
MN
OP
QO
vera
ll q
ual
ity
Rev
iew
(3)
Sha
mliy
an 2
008
121
00
11?
-?
?+
Wea
k
Sim
on 2
005
110
40
7?
++
??
Mod
erat
e
Sni
jder
s 20
0710
??
??
++
-?
?M
oder
ate
RC
T (
6)B
erne
r 20
06+
-+
NA
++
?S
tron
g
Don
ald
2000
??
NA
++
??
Wea
k
Koz
er 2
005
++
NA
+-
+?
Mod
erat
e
Man
ning
200
7+
?N
A-
NA
+?
Wea
k
Sch
neid
er 2
006
++
+N
A+
+?
Str
ong
Tid
eiks
aar
1993
??
NA
++
??
Wea
k
CB
A (
4)E
vans
200
7+
??
+?
-?
Wea
k
Kin
g 20
03?
NA
NA
+?
--
Wea
k
Leap
e 19
99?
NA
NA
++
-+
Mod
erat
e
Pao
letti
200
7-
NA
NA
++
++
Str
ong
ITS
(9)
Coh
en 2
005
??
-?
+-
+?
Wea
k
Frae
nkel
200
3?
?-
--
??
?W
eak
Har
ris 2
007
??
--
-?
??
Wea
k
Lehm
ann
2007
+?
-+
+?
?+
Mod
erat
e
Sch
wen
dim
ann
2006
??
+-
++
++
Mod
erat
e
Sim
pson
200
4-
+-
--
--
?W
eak
Stu
mp
2000
-?
--
-+
??
Wea
k
Voe
ffray
200
6?
+-
++
+?
?M
oder
ate
Wal
sh 2
008
?+
++
++
+-
Str
ong
UB
A (
16)
Dem
psey
200
4?
Wea
k
DeV
ita 2
005
+W
eak
Don
oghu
e 20
05+
Wea
k
Fert
lem
an 2
005
?W
eak
Jain
200
6?
Wea
k
Lane
199
9+
Wea
k
Lars
en 2
005
?W
eak
Ple
ws-
Oga
n 20
04?
Wea
k
Poo
n 20
06+
Wea
k
Ram
nara
yan
2006
a?
Wea
k
Ram
nara
yan
2006
b+
Wea
k
Rob
inso
n 20
06?
Wea
k
Silv
er 2
000
?W
eak
Sim
200
2?
Wea
k
Will
iam
s 20
07+
Wea
k
Wol
ff 20
02?
Wea
k
Ap
pen
dix
D: Q
ual
ity
of s
tud
y d
esig
n

Dückers et al
Safety and risk management in hospitals
34
Appendix D: Quality of study design
Dückers et al
Safety and risk management in hospitals
35
Appendix D: Quality of study design
Des
ign
Fir
st a
uth
or
A1
A2
A3
A4
A5
B1
B2
CD
1D
2E
FG
1G
2H
IJ
KL
MN
OP
QO
vera
ll q
ual
ity
Rev
iew
(3)
Sha
mliy
an 2
008
121
00
11?
-?
?+
Wea
k
Sim
on 2
005
110
40
7?
++
??
Mod
erat
e
Sni
jder
s 20
0710
??
??
++
-?
?M
oder
ate
RC
T (
6)B
erne
r 20
06+
-+
NA
++
?S
tron
g
Don
ald
2000
??
NA
++
??
Wea
k
Koz
er 2
005
++
NA
+-
+?
Mod
erat
e
Man
ning
200
7+
?N
A-
NA
+?
Wea
k
Sch
neid
er 2
006
++
+N
A+
+?
Str
ong
Tid
eiks
aar
1993
??
NA
++
??
Wea
k
CB
A (
4)E
vans
200
7+
??
+?
-?
Wea
k
Kin
g 20
03?
NA
NA
+?
--
Wea
k
Leap
e 19
99?
NA
NA
++
-+
Mod
erat
e
Pao
letti
200
7-
NA
NA
++
++
Str
ong
ITS
(9)
Coh
en 2
005
??
-?
+-
+?
Wea
k
Frae
nkel
200
3?
?-
--
??
?W
eak
Har
ris 2
007
??
--
-?
??
Wea
k
Lehm
ann
2007
+?
-+
+?
?+
Mod
erat
e
Sch
wen
dim
ann
2006
??
+-
++
++
Mod
erat
e
Sim
pson
200
4-
+-
--
--
?W
eak
Stu
mp
2000
-?
--
-+
??
Wea
k
Voe
ffray
200
6?
+-
++
+?
?M
oder
ate
Wal
sh 2
008
?+
++
++
+-
Str
ong
UB
A (
16)
Dem
psey
200
4?
Wea
k
DeV
ita 2
005
+W
eak
Don
oghu
e 20
05+
Wea
k
Fert
lem
an 2
005
?W
eak
Jain
200
6?
Wea
k
Lane
199
9+
Wea
k
Lars
en 2
005
?W
eak
Ple
ws-
Oga
n 20
04?
Wea
k
Poo
n 20
06+
Wea
k
Ram
nara
yan
2006
a?
Wea
k
Ram
nara
yan
2006
b+
Wea
k
Rob
inso
n 20
06?
Wea
k
Silv
er 2
000
?W
eak
Sim
200
2?
Wea
k
Will
iam
s 20
07+
Wea
k
Wol
ff 20
02?
Wea
k
A1:
nu
mbe
r of s
tudi
es in
clud
ed. A
2: n
umbe
r of R
CTs
in
clud
ed. A
3: n
umbe
r of C
BA
s in
clud
ed.
A4:
num
ber o
f IT
Ss
incl
uded
. A5
: num
ber o
f UB
As
incl
uded
B1:
sc
orin
g of
elig
ibili
ty b
y at
leas
t tw
o au
thor
s.
B2
: aut
hors
use
d in
clus
ion
and
excl
usio
n cr
iteria
C:
desi
gns
wer
e ju
dged
usi
ng p
rede
fined
cri
teria
(E
PO
C,
Jaha
d, e
tc)
D1:
sco
ring
of fi
ndin
gs b
y at
leas
t tw
o au
thor
s. D
2: a
utho
rs
used
dat
a ex
trac
tion
form
s
E:
conc
ealm
ent o
f allo
catio
n (p
rote
ctio
n ag
ains
t sel
ectio
n bi
as)
F:
prot
ectio
n ag
ains
t con
tam
inat
ion
(eg
rand
omis
ing
orga
nisa
tion
/pro
fess
iona
ls r
athe
r tha
n in
divi
dual
pa
tient
s)
G1:
fol
low
-up
of p
rofe
ssio
nals
(pr
otec
tion
agai
nst e
xclu
sion
bi
as).
G2
: fol
low
-up
of p
atie
nts
or e
piso
des
of c
are
H:
base
line
mea
sure
men
t (no
diff
eren
ces)
I:
blin
ded
asse
ssm
ent o
f prim
ary
outc
ome
(s) (
prot
ectio
n ag
ains
t det
ectio
n bi
as)
J:
char
acte
rist
ics
for s
tudi
es u
sing
sec
ond
site
as
cont
rol
K:
the
inte
rven
tion
is in
depe
nden
t of o
ther
cha
nges
L:
data
wer
e an
alys
ed a
ppro
pria
tely
(A
RIM
A o
r tim
e se
ries
reg
ress
ion)
M:
reas
on fo
r the
num
ber o
f poi
nts
pre
and
post
in
terv
entio
n gi
ven
N:
shap
e of
the
inte
rven
tion
effe
ct w
as s
peci
fied
O:
inte
rven
tion
unlik
ely
to a
ffec
t dat
a co
llect
ion
P:
com
plet
enes
s of
dat
a se
t
Q:
relia
ble
prim
ary
outc
ome
mea
sure
(s)
+ =
done
- = n
ot d
one
? =
uncl
ear
NA
= n
ot a
vaila
ble

Dückers et al
Safety and risk management in hospitals
36
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
37
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Ber
ner,
200
6
US
A
RC
T
Am
bula
tory
/out
patie
nt c
are,
ge
nera
l int
erna
l med
icin
e
Inte
rven
tion
grou
p:
N =
34
(pre
-inte
rven
tion)
N =
31
(pos
t-in
terv
entio
n)C
ontr
ol g
roup
:N
= 3
4 (p
re-in
terv
entio
n)N
= 2
8 (p
ost-
inte
rven
tion)
Per
iod
= N
C (
8-m
onth
fo
llow
-up)
Aim
To e
valu
ate
the
effe
ctiv
enes
s of
a P
DA
-bas
ed C
DS
S o
n N
SA
ID p
resc
ribin
g sa
fety
by
inte
rnal
med
icin
e re
side
nts
in
the
outp
atie
nt s
ettin
g
Inte
rven
tio
nP
DA
with
CD
SS
Co
ntr
ol
PD
A w
ithou
t CD
SS
Pri
mar
y o
utc
om
eP
ropo
rtio
n of
cas
es
per d
octo
r with
uns
afe
NS
AID
pre
scrip
tions
AN
CO
VA
Sig
nific
ant r
educ
tion
(0.2
3 ve
rsus
0.
45 u
nsaf
e pr
escr
iptio
n ca
ses
per
doct
or [I
ver
sus
C],
F =
4.2
4, p
< 0
.05,
ef
fect
siz
e =
0.5
4)
Res
iden
ts p
rovi
ded
with
a
PD
A-b
ased
CD
SS
for N
SA
ID
pres
crib
ing
mad
e fe
wer
uns
afe
trea
tmen
t dec
isio
ns th
an
part
icip
ants
usi
ng a
PD
A w
ithou
t th
e C
DS
S
Coh
en, 2
005
US
A
ITS
Hos
pita
l car
e
N =
10
–20
char
t rev
iew
s of
dis
char
ged
patie
nts
per
mon
th
Per
iod
= 20
01–2
003
(6
mon
ths
base
line,
9 m
onth
s im
plem
enta
tion,
21-
mon
th
follo
w-u
p)
Aim
To a
sses
s th
e im
pact
of
a w
ide
rang
ing
safe
ty
prog
ram
me
on p
atie
nt h
arm
Inte
rven
tio
nC
ombi
ned
inte
rven
tion,
in
clud
ing
:•
form
atio
n of
a p
atie
nt
safe
ty c
ounc
il•
assi
gnin
g a
full-
time
safe
ty s
peci
alis
t•
impl
emen
tatio
n of
eve
nt
repo
rtin
g sy
stem
• in
trod
uctio
n of
dru
g pr
otoc
ols
• w
eekl
y m
edic
atio
n pr
ofile
au
dits
• or
der s
tand
ardi
satio
n
Co
ntr
ol
NA
1. A
DE
rat
e pe
r 1,0
00
dose
s de
liver
ed
2. A
DE
rat
e pe
r 1,0
00
patie
nt d
ays
3. P
ropo
rtio
n of
pa
tient
s w
ith a
n A
DE
4.
Num
ber o
f AD
Es
asso
ciat
ed w
ith
patie
nt h
arm
pe
r tot
al d
oses
de
liver
ed
5. C
ost s
avin
g
Chi
-squ
are
test
for t
rend
s
1. S
igni
fican
t red
uctio
n (m
edia
n =
2.04
[1.7
9–2
.70,
IQR
] in
base
line
vers
us 0
.65
[0.4
1–0.
87] p
ost-
inte
rven
tion,
p
= 0.
001
) 2.
Sig
nific
ant r
educ
tion
(med
ian
= 5.
07 [3
.79
–6.
02] i
n ba
selin
e ve
rsus
1.
30 [0
.87–
1.71
] pos
t-in
terv
entio
n,
p =
0.0
01)
3. S
igni
fican
t dec
line
(27%
at b
asel
ine
vers
us 9
% p
ost-
inte
rven
tion,
RR
=
0.33
, p <
0.0
01)
4. S
igni
fican
t red
uctio
n (R
R =
0.1
2 [0
.04
–0.
38, 9
5% C
I], p
< 0
.001
)5.
With
4,4
00
AD
Es
prev
ente
d ea
ch
year
, ann
ual c
ost s
avin
gs a
re
appr
oxim
atel
y $1
0,0
00,
00
0
Hig
hly
effe
ctiv
e, in
expe
nsiv
e pr
ogra
mm
e
Ap
pen
dix
E: I
ncl
ud
ed s
tud
ies,
so
rted
by
alp
hab
etic
al o
rder

Dückers et al
Safety and risk management in hospitals
36
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
37
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Dem
psey
, 20
04
Aus
tral
ia
UB
A
Acu
te m
edic
al a
rea
Per
iod
= Ja
nuar
y –
June
19
95 (
pre
-inte
rven
tion)
, Ja
nuar
y –
June
199
6 (p
ost-
inte
rven
tion)
, 20
01
(re
-eva
luat
ion
5 ye
ars
post
-in
terv
entio
n)
Aim
To te
st th
e ef
fect
iven
ess
of a
fa
lls p
reve
ntio
n pr
ogra
mm
e in
an
acu
te m
edic
al w
ard
Inte
rven
tio
nF
alls
pre
vent
ion
prog
ram
me,
co
nsis
ting
of a
n as
sess
men
t to
ol, a
n al
ert g
raph
ic, a
nd
educ
atio
n fo
r pat
ient
and
sta
ff
Co
ntr
ol
NA
Fal
l rat
e (p
er 1
,00
0 O
BD
) N
on-p
aire
d t-
test
Sig
nific
ant r
educ
tion
in fa
ll ra
te
(3.6
3 pr
e-in
terv
entio
n ve
rsus
2.2
9 po
st-in
terv
entio
n [p
= 0
.05
])
Fiv
e ye
ars
post
-inte
rven
tion,
fall
rate
ha
s do
uble
d (6
.8, s
igni
fican
ce n
ot
pres
ente
d)
Mar
gina
lly e
ffec
tive
falls
pr
even
tion
prog
ram
me,
but
re
sults
wer
e no
t sus
tain
able
af
ter 5
yea
rs
DeV
ita, 2
005
US
A
UB
A
Adv
ance
car
diac
life
su
ppor
t/m
edic
al e
mer
genc
y te
am
N =
10
cour
ses
and
138
indi
vidu
als
Per
iod
= M
arch
20
02 –
May
20
03
Aim
To d
evel
op m
ultid
isci
plin
ary
team
ski
lls a
nd im
prov
e M
ET
pe
rfor
man
ce
Inte
rven
tio
nH
uman
sim
ulat
ion
trai
ning
in
an e
duca
tiona
l env
ironm
ent t
o de
velo
p m
ultid
isci
plin
ary
team
sk
ills.
Cou
rse
com
pone
nts:
1. W
eb-b
ased
pre
sent
atio
n an
d pr
e-t
est b
efor
e th
e co
urse
2. B
rief r
einf
orci
ng tr
aini
ng
sess
ion
on th
e da
y of
the
cour
se3.
Thr
ee o
f fiv
e di
ffer
ent
sim
ulat
ed s
cena
rios
each
fo
llow
ed b
y4.
Deb
riefin
g an
d an
alys
is
with
the
team
Co
ntr
ol
NA
Pri
mar
y o
utc
om
e1.
Suc
cess
ful c
risis
m
anag
emen
t re
sulti
ng in
m
anne
quin
‘s
urvi
val’
Sec
on
dar
y o
utc
om
e2.
Com
plet
ion
of
orga
nisa
tiona
l and
pa
tient
car
e ta
sks
Non
-par
amet
ric te
sts:
Coc
hran
’s Q
an
d K
enda
ll’s
W
1. S
igni
fican
t im
prov
ed o
vera
ll si
mul
ator
‘sur
viva
l’ fr
om 0
% to
90
%
acro
ss th
e th
ree
sess
ions
in a
day
’s
cour
se (
Coc
hran
’s Q
= 1
2.6,
p
= 0.
002
). M
ost i
mpr
ovem
ent
betw
een
the
first
and
the
seco
nd
sess
ions
(p
= 0.
014)
rat
her t
han
betw
een
the
seco
nd a
nd th
ird
sess
ions
(p
= 0.
180
) (po
st-h
oc
anal
ysis
) 2.
Sig
nific
antly
impr
oved
ove
rall
task
co
mpl
etio
n ra
te fr
om 3
1% to
89
%,
and
each
sim
ulat
or r
ole
impr
oved
fr
om 1
0 to
45%
dur
ing
the
first
se
ssio
n to
80
to 9
5% d
urin
g th
e th
ird s
essi
on (
Ken
dall’
s W
= 0
.91,
p
< 0.
001
). Im
prov
emen
t firs
t and
se
cond
ses
sion
s (p
= 0
.002
) and
be
twee
n se
cond
and
third
(p
= 0
.011
) (po
st-h
oc a
naly
sis)
Trai
ning
mul
tidis
cipl
inar
y te
ams
usin
g si
mul
atio
n te
chno
logy
is
feas
ible
and
eff
ectiv
e in
im
prov
ing
team
per
form
ance
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
38
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
39
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Don
ald,
20
00
Uni
ted
Kin
gdom
RC
T
Eld
erly
car
e re
habi
litat
ion
war
d in
a c
omm
unity
ho
spita
l
N =
54
Per
iod
= F
ebru
ary
– S
epte
mbe
r 199
6 (9
mon
ths)
Aim
Com
paris
on o
f tw
o flo
orin
g ty
pes
– ca
rpet
and
vin
yl –
in
the
bed
area
s, a
nd tw
o ty
pes
of p
hysi
othe
rapy
–
conv
entio
nal t
hera
py a
nd
addi
tiona
l leg
str
engt
heni
ng
exer
cise
s –
in a
void
ing
falls
Inte
rven
tio
n 1
1a. A
ssig
ned
to w
ard
area
w
ith v
inyl
floo
r cov
erin
g an
d co
nven
tiona
l phy
siot
hera
py,
once
or t
wic
e da
ily1b
. As
1a p
lus
seat
ed le
g st
reng
then
ing
exer
cise
s (h
ip fl
exor
s an
d an
kle
dors
iflex
ors)
Inte
rven
tio
n 2
2a. A
ssig
ned
to w
ard
area
with
car
pet a
nd
conv
entio
nal p
hysi
othe
rapy
2b. A
s 2a
plu
s se
ated
leg
stre
ngth
enin
g ex
erci
ses
(hip
flex
ors
and
ankl
e do
rsifl
exor
s)
1. N
umbe
r of f
alle
rs
durin
g ad
mis
sion
2. N
umbe
r of f
ract
ure
falls
Man
n-W
hitn
ey U
-tes
t and
Chi
-squ
are
with
Fis
her’s
exa
ct te
st
1. N
o di
ffer
ence
in n
umbe
r of f
alle
rs:
• a
dditi
onal
exe
rcis
e gr
oup
vers
us
conv
entio
nal p
hysi
othe
rapy
= 4
fa
lls v
ersu
s 7
falls
, RR
= 0
.21,
95
% C
I = 0
.04
–1.2
(p
= 0.
12)
• c
arpe
t ver
sus
viny
l = 1
0 fa
lls
vers
us 1
fall,
RR
= 8
.30,
95%
C
I = 0
.95
–73
(p =
0.0
5)2.
No
fall
resu
lted
in a
frac
ture
The
re is
no
evid
ence
to s
uppo
rt
eith
er in
terv
entio
n in
pre
vent
ing
falls
on
a re
habi
litat
ion
war
d

Dückers et al
Safety and risk management in hospitals
38
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
39
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Don
oghu
e,
2005
Aus
tral
ia
UB
A
Acu
te a
ged
care
/eld
er c
are
war
d
N =
3,9
72 O
BD
(20
01),
3,
455
OB
D (
2002
),
num
bers
not
pre
sent
ed fo
r 20
03/2
004
Per
iod
= Ja
nuar
y 20
01
– A
ugus
t 20
02 (
pre
-in
terv
entio
n 19
mon
ths)
, A
ugus
t 20
02 –
Apr
il 20
04
(pos
t-in
terv
entio
n 15
m
onth
s)
Aim
To p
reve
nt h
igh-
risk
inpa
tient
s on
an
acut
e ag
ed c
are
war
d fr
om fa
lling
Inte
rven
tio
nP
atie
nts
at h
igh
risk
of
falli
ng a
re a
ccom
pani
ed b
y vo
lunt
eer C
Os
on w
eekd
ays
8.0
0am
–8.
00p
m. T
heir
prim
ary
obje
ctiv
e w
as to
ob
serv
e pa
tient
s fo
r sig
ns
of in
crea
sing
agi
tatio
n or
ris
ky b
ehav
iour
and
, if
need
ed, t
o re
assu
re th
e pa
tient
or c
onta
ct a
nur
se.
The
CO
s w
ere
also
invo
lved
in
oth
er a
ctiv
ities
, suc
h as
co
nver
satio
ns, p
layi
ng c
ards
, re
adin
g ou
t lou
d, p
layi
ng
mus
ic, p
ract
ical
hel
p in
find
ing
belo
ngin
g sa
nd s
ettin
g up
m
eals
Co
ntr
ol
NA
Fal
l rat
e (p
er 1
,00
0 O
BD
)C
hi-s
quar
e te
st
Sig
nific
antly
dec
reas
ed fa
ll ra
te. 1
5.6
falls
/1,0
00
OB
D (
SD
= 6
.5) (
befo
re)
vers
us 8
.8 fa
lls/1
,00
0 O
BD
(S
D =
3.0
) (a
fter
), O
R =
0.5
6 [9
5% C
I = 0
.45
–0.
68],
p <
0.0
001
Sig
nific
ant p
ositi
ve e
ffec
t of
inte
rven
tion
on fa
ll ra
te
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
40
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
41
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Eva
ns, 2
007
Aus
tral
ia
CB
A
Inpa
tient
car
e on
ICU
s,
surg
ical
uni
ts, m
edic
al u
nits
an
d E
Ds
Inte
rven
tion
(I) u
nits
: N =
10
Con
trol
(C
) uni
ts: N
= 1
0In
eac
h ar
m: 3
5,0
00
OB
Ds
at b
asel
ine
and
durin
g st
udy
perio
d
Inte
rven
tion
rollo
ut w
as
stag
gere
d, fr
om J
une
– A
ugus
t 20
03, w
ith
units
impl
emen
ting
the
inte
rven
tion
over
a 4
0-w
eek
perio
d
Aim
To a
sses
s th
e ef
fect
iven
ess
of a
n in
terv
entio
n pa
ckag
e in
ord
er to
impr
ove
volu
ntar
y in
cide
nt r
epor
ting
Inte
rven
tio
n•
Que
stio
nnai
re a
nd fo
cus
grou
p to
iden
tify
barr
iers
fo
r inc
iden
t rep
ortin
g•
Man
ual t
o im
prov
e kn
owle
dge
• E
duca
tion
sess
ions
• R
edes
ign
of r
epor
ting
proc
esse
s to
add
ress
co
ncer
ns•
One
-pag
e re
port
form
re
plac
ing
the
exis
ting
thre
e-p
age
form
and
a
free
-cal
l tel
epho
ne
serv
ice
• F
our f
eedb
ack
new
slet
ters
and
pr
esen
tatio
ns a
t mee
tings
Co
ntr
ol
No
inte
rven
tion,
ie u
sual
err
or
repo
rtin
g pr
oced
ures
1. In
cide
nt r
epor
ting
rate
s pe
r 10,
00
0 O
BD
or p
er 1
0,0
00
ED
atte
ndan
ces
2. R
epor
ter
desi
gnat
ion
3. R
epor
ting
form
at4.
Typ
es o
f inc
iden
ts
repo
rted
Fis
her’s
exa
ct te
st, b
inom
ial
regr
essi
on a
naly
sis
and
Poi
sson
re
gres
sion
ana
lysi
s
1. S
igni
fican
t inc
reas
e in
rep
ortin
g ra
tes
in in
patie
nt c
are
(add
ition
al
60.3
rep
orts
/10,
00
0 O
BD
[95%
CI
= 23
.8–
96.
8],
p <
0.0
01) a
nd in
ED
s (a
dditi
onal
39.
5 re
port
s/10
,00
0 E
D
atte
ndan
ces
[95%
= C
I 17.
0–
62.0
],
p <
0.0
01)
2. M
ore
repo
rts
wer
e ge
nera
ted
: •
by d
octo
rs in
ED
s (a
dditi
onal
9.5
re
port
s/10
,00
0 E
D a
ttend
ance
s [9
5% C
I = 2
.2–1
6.8
], p
= 0
.001
)•
by n
urse
s in
inpa
tient
are
as
(add
ition
al 5
9.0
repo
rts/
10,0
00
OB
Ds
[95%
CI =
23.
9–
94.1
],
p <
0.0
01)
• an
onym
ousl
y (a
dditi
onal
20.
2 re
port
s/10
,00
0 O
BD
s an
d E
D
atte
ndan
ces
com
bine
d [9
5% C
I =
12.6
–27.
8],
p <
0.0
01)
3. M
ajor
ity (
79%
) of r
epor
ts in
I-un
its
wer
e re
port
ed u
sing
one
-pag
e fo
rm,
with
21%
sub
mitt
ed th
roug
h th
e ca
ll ce
ntre
4. R
elat
ive
num
ber o
f fal
l-re
late
d re
port
s de
crea
sed
in I-
units
(36
.1%
be
fore
ver
sus
23.8
% a
fter
, RR
=
2.01
[95%
CI =
1.7
–2.3
], p
< 0
.001
).
I-un
its h
ad m
ore
docu
men
tatio
n-re
late
d, c
linic
al m
anag
emen
t an
d ag
gres
sion
-rel
ated
inci
dent
s co
mpa
red
with
C-u
nits
The
inte
rven
tion
units
rep
orte
d a
grea
ter v
arie
ty a
nd n
umbe
r of
inci
dent
s du
ring
the
stud
y, w
ith
impr
oved
rep
ortin
g by
doc
tors
fr
om a
low
bas
elin
e. T
here
was
co
nsid
erab
le h
eter
ogen
eity
be
twee
n re
port
ing
rate
s in
di
ffer
ent t
ypes
of u
nits

Dückers et al
Safety and risk management in hospitals
40
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
41
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Fer
tlem
an,
2005
Uni
ted
Kin
gdom
UB
A
Acu
te m
edic
al s
ervi
ces
– ge
nera
l hos
pita
l
N =
62
patie
nts
(p
re-in
terv
entio
n)N
= 5
7 pa
tient
s (in
terv
entio
n)
Per
iod
= A
pril
– Ju
ly 2
003
Aim
To r
educ
e m
edic
atio
n er
rors
an
d pr
escr
ibin
g co
sts
Inte
rven
tio
nA
dditi
on o
f a p
harm
acis
t to
the
post
-tak
e m
edic
al te
am
Co
ntr
ol
NA
1. A
ccur
acy
of
med
icat
ion
hist
ory
2. P
resc
ribin
g co
sts
3. M
edic
atio
n-as
soci
ated
ris
ks
Chi
-squ
are
test
1. D
etec
ted
disc
repa
ncie
s be
twee
n th
e ad
mis
sion
and
the
phar
mac
ist-
deriv
ed d
rug
hist
ory
incr
ease
d fr
om 5
3% to
98%
(pr
e-in
terv
entio
n ve
rsus
inte
rven
tion
perio
d)2.
Mea
n sa
ving
from
dru
gs s
topp
ed
durin
g ad
mis
sion
was
£88
.60
per
patie
nt p
er y
ear d
urin
g in
terv
entio
n pe
riod
vers
us £
5.52
in p
re-
inte
rven
tion
perio
d3.
Maj
ority
of r
ecom
men
datio
ns
by p
harm
acis
t wer
e of
min
or o
r m
oder
ate
sign
ifica
nce
(53%
and
53
% r
espe
ctiv
ely)
and
5%
wer
e cl
assi
fied
as p
reve
ntin
g a
pote
ntia
lly
maj
or in
cide
nt
The
pre
senc
e of
a p
harm
acis
t on
a p
ost-
take
war
d ro
und
impr
oved
the
accu
racy
of
drug
-his
tory
doc
umen
tatio
n,
redu
ced
pres
crib
ing
cost
s an
d de
crea
sed
the
pote
ntia
l ris
k to
pa
tient
s
Frae
nkel
, 20
03
Aus
tral
ia
ITS
(bu
t ana
lyse
d as
UB
A)
ICU
in o
ne h
ospi
tal
N =
12
beds
Per
iod
= Ja
nuar
y 19
95 –
D
ecem
ber 1
998
(23
mon
ths
pre
-inte
rven
tion
and
25
mon
ths
post
-inte
rven
tion)
Aim
To q
uant
ify th
e qu
ality
be
nefit
s an
d st
aff p
erce
ptio
ns
of a
com
pute
rised
clin
ical
in
form
atio
n sy
stem
im
plem
enta
tion
in a
n IC
U
Inte
rven
tio
nC
linic
al in
form
atio
n sy
stem
, rep
laci
ng p
aper
-ba
sed
char
ts o
f pat
ient
ob
serv
atio
ns, c
linic
al r
ecor
ds,
resu
lts r
epor
ting
and
drug
pr
escr
ibin
g
Co
ntr
ol
NA
1. F
requ
ency
of
clin
ical
AE
s2.
Per
cept
ion
of ti
me
take
n in
nur
sing
do
cum
enta
tion
Chi
-squ
are
test
1. N
umbe
r of c
linic
al A
Es
by c
ateg
ory:
• M
edic
atio
n in
cide
nts
decr
ease
d fr
om 8
5 to
55
(p <
0.0
5)•
Intr
aven
ous
inci
dent
s de
crea
sed
from
140
to 4
6 (p
< 0
.001
)•
Ven
tilat
ion
inci
dent
s de
crea
sed
from
51
to 1
0 (p
< 0
.001
)•
Pre
ssur
e ul
cers
rem
aine
d st
able
(c
hang
ed fr
om 7
1 to
51,
p =
0.1
52)
• O
ther
inci
dent
s in
crea
sed
from
20
1 to
323
(p
< 0.
001
)
2. S
igni
fican
t dec
reas
e in
per
cent
age
of n
urse
s sp
endi
ng le
ss th
an 1
0 m
inut
es d
ocum
entin
g no
tes
(22%
be
fore
ver
sus
82%
aft
er, p
< 0
.001
)
Sig
nific
ant r
educ
tion
in n
umbe
r of
key
AE
s, a
long
side
pos
itive
nu
rsin
g st
aff p
erce
ptio
ns a
bout
tim
e in
vest
men
t
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
42
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
43
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Har
ris, 2
007
US
A
ITS
(bu
t ana
lyse
d as
UB
A)
Med
ical
ICU
, sur
gica
l IC
U
and
card
ioth
orac
ic IC
U
Pre
-inte
rven
tion:
16,
089
patie
nt d
ays
Pos
t-in
terv
entio
n: 1
7,12
6 pa
tient
day
s
Per
iod
= Ja
nuar
y 20
02
– M
ay 2
004
(10
mon
ths
pre
-inte
rven
tion,
14
mon
ths
inte
rven
tion
and
5 m
onth
s po
st-in
terv
entio
n)
Aim
To in
crea
se p
atie
nt-s
afet
y ev
ent r
epor
ting
in th
ree
ICU
s us
ing
a ne
w, v
olun
tary
, car
d-ba
sed
even
t rep
ortin
g sy
stem
an
d to
com
pare
and
eva
luat
e ob
serv
ed d
iffer
ence
s in
re
port
ing
amon
g he
alth
care
w
orke
rs a
cros
s IC
Us
Inte
rven
tio
nIm
plem
enta
tion
of a
n an
onym
ous
pape
r-ba
sed
erro
r rep
ort t
ool (
as o
ppos
ed
to e
xist
ing
onlin
e to
ols)
Co
ntr
ol
NA
1. R
epor
ted
patie
nt-
safe
ty e
vent
s/1,
00
0 pa
tient
day
s2.
Rep
orte
r de
sign
atio
n3.
Sev
erity
of r
epor
ted
inci
dent
s
Chi
-squ
are
test
1. S
igni
fican
t inc
reas
e in
rep
ortin
g ra
tes
(pre
-inte
rven
tion
= 20
.4
even
ts/1
,00
0 pa
tient
day
s ve
rsus
41
.7 r
epor
ted
even
ts/1
,00
0 pa
tient
da
ys p
ost-
inte
rven
tion;
rat
e ra
tio =
2.
05 [9
5% C
I = 1
.79
–2.3
4])
2. N
urse
s su
bmitt
ed th
e m
ajor
ity
of r
epor
ts (
post
-inte
rven
tion:
nu
rses
= 6
7.1%
, doc
tors
= 2
3.1%
, ot
her r
epor
ters
= 9
.5%
). D
octo
rs
expe
rienc
ed th
e gr
eate
st in
crea
se
in r
epor
ting
rate
(do
ctor
s: 4
3-f
old,
nu
rses
: 1.7
-fol
d, o
ther
rep
orte
rs:
4.3
-fol
d) r
elat
ive
to p
re-in
terv
entio
n ra
tes
3. S
igni
fican
t diff
eren
ces
in
the
repo
rtin
g of
har
m b
y jo
b de
scrip
tion:
31.
1% o
f rep
orts
from
nu
rses
, 36.
2% fr
om o
ther
sta
ff
and
17.0
% fr
om d
octo
rs d
escr
ibed
ev
ents
that
did
not
rea
ch/a
ffec
t th
e pa
tient
(p
< 0.
001
); 3
3.9
% o
f re
port
s fr
om d
octo
rs, 2
7.2%
from
nu
rses
and
13.
0%
from
oth
er s
taff
de
scrib
ed e
vent
s th
at c
ause
d ha
rm
(p <
0.0
05)
Rep
ortin
g ra
tes
incr
ease
d si
gnifi
cant
ly, w
ith s
igni
fican
t di
ffer
ence
s in
rep
ortin
g be
havi
our b
y ty
pe o
f hea
lthca
re
wor
ker a
nd IC
U ty
pe

Dückers et al
Safety and risk management in hospitals
42
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
43
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Jain
, 20
06
US
A
UB
A
Med
ical
sur
gica
l IC
U (
28
beds
)
N =
ran
dom
rev
iew
of a
t le
ast 2
0 ch
arts
per
mon
th (±
20
% s
ampl
ing)
Per
iod
= O
ctob
er 2
00
0 –
Oct
ober
20
02 (
base
line)
, O
ctob
er 2
002
– O
ctob
er
2003
(in
terv
entio
n)
Aim
Red
uctio
n in
AE
s in
ICU
s by
Q
I foc
usin
g on
team
wor
k an
d cu
lture
cha
nge
Inte
rven
tio
nC
ombi
ned
inte
rven
tion,
in
clud
ing
:1.
doc
tor-
led
mul
tidis
cipl
inar
y ro
unds
2. d
aily
bed
-flo
w m
eetin
gs to
ac
cess
bed
ava
ilabi
lity
3. im
plem
enta
tion
of
evid
ence
-bas
ed p
ract
ices
re
late
d to
thre
e qu
ality
in
itiat
ives
4. c
ultu
re c
hang
e w
ith a
foru
m
on te
am d
ecis
ion-
mak
ing
The
inte
rven
tions
wer
e im
plem
ente
d on
e-b
y-on
e ov
er
a 12
-mon
th p
erio
d
Co
ntr
ol
NA
1. A
Es
per I
CU
day
2. V
entil
ator
-as
soci
ated
pn
eum
onia
rat
e pe
r 1,
00
0 ve
ntila
tion
days
3. B
lood
stre
am
infe
ctio
n ra
te p
er
1,0
00
line
days
4. N
osoc
omia
l urin
ary
trac
t inf
ectio
n ra
te
per 1
,00
0 ca
thet
er
days
5. L
OS
per
epi
sode
6. M
orta
lity
rate
7. C
osts
per
ICU
ep
isod
e
Chi
-squ
are
test
1. S
tron
g do
wnw
ard
tren
d (s
igni
fican
ce n
ot p
rovi
ded)
2. S
igni
fican
tly lo
wer
infe
ctio
n ra
te
(7.5
at b
asel
ine
vers
us 3
.2 a
t fol
low
-up
, p =
0.0
40)
3. S
igni
fican
tly lo
wer
infe
ctio
n ra
te
(5.9
at b
asel
ine
vers
us 3
.1 a
t fol
low
-up
, p =
0.0
31)
4. N
o si
gnifi
cant
cha
nge
5. D
ownw
ard
tren
d (s
igni
fican
ce n
ot
prov
ided
by
the
auth
ors)
6. N
o si
gnifi
cant
cha
nge
7. D
ecre
ased
by
21%
(fr
om $
3,40
6 to
$
2,97
3, s
igni
fican
ce n
ot p
rovi
ded)
QI m
ay h
ave
cont
ribut
ed to
im
prov
emen
ts
Kin
g, 2
003
Can
ada
CB
A
Pae
diat
ric in
patie
nt c
are
N =
2 m
edic
al in
patie
nt u
nits
(in
terv
entio
n) a
nd 1
med
ical
an
d 2
surg
ical
uni
ts (
cont
rol)
Per
iod
= A
pril
1993
– M
arch
19
96
(bas
elin
e 36
mon
ths)
, A
pril
199
6 –
Dec
embe
r 19
96
(impl
emen
tatio
n 9
mon
ths)
, Jan
uary
199
7 –
Dec
embe
r 199
9 (p
ost-
inte
rven
tion
36 m
onth
s)
Aim
To a
sses
s th
e im
pact
of a
C
PO
E s
yste
m o
n m
edic
atio
n er
rors
and
AD
Es
in p
aedi
atric
in
patie
nts
Inte
rven
tio
nC
PO
E w
ithou
t clin
ical
de
cisi
on s
uppo
rt, i
nter
face
d w
ith th
e la
bora
tory
sys
tem
, bu
t not
with
the
phar
mac
y co
mpu
ter
Co
ntr
ol
Han
dwrit
ten
med
icat
ion
orde
rs
1. M
edic
atio
n er
ror
rate
(pe
r 1,0
00
patie
nt d
ays)
2. P
oten
tial A
DE
s ra
te3.
AD
Es
rate
Poi
sson
ana
lysi
s of
rat
e ra
tios
1. S
igni
fican
t red
uctio
n (R
R =
1.5
4 [9
5% C
I = 1
.27–
1.88
], p
< 0
.001
)2.
Sig
nific
ant i
ncre
ase
(RR
= 0
.24
[95%
CI =
0.0
9–
0.68
], p
< 0
.001
)3.
No
chan
ge (
RR
= 1
.30
[95%
CI =
0.
47–
3.52
], p
= 0
.60
)
The
ove
rall
med
icat
ion
erro
r rat
e an
d po
tent
ial A
DE
s de
crea
sed,
w
ithou
t an
effe
ct o
n A
DE
s
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
44
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
45
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Koz
er, 2
005
Can
ada
RC
T
Pae
diat
ric E
D
N =
376
ord
er s
heet
s (in
terv
entio
n [I
] gro
up)
N =
411
ord
er s
heet
s (c
ontr
ol [C
] gro
up)
Per
iod
= Ju
ly 2
001
Aim
To d
eter
min
e w
heth
er th
e us
e of
a s
truc
ture
d or
der
shee
t red
uces
the
inci
denc
e of
med
icat
ion
erro
rs in
pa
edia
tric
ED
Inte
rven
tio
nU
se o
f pre
-prin
ted,
form
atte
d pr
escr
iptio
n or
der s
heet
s
Co
ntr
ol
Use
of b
lank
pre
scrip
tion
orde
r she
ets
1. M
edic
atio
n er
ror
rate
2. M
edic
atio
n er
ror
seve
rity
Chi
-squ
are
test
and
mul
tivar
iabl
e lo
gist
ic r
egre
ssio
n
1. S
igni
fican
t red
uctio
n (9
.8%
in
I-gr
oup
vers
us 1
6.6%
in C
-gro
up,
OR
= 0
.55
[95%
CI =
0.3
4–
0.9
0],
p
< 0.
05)
2. S
igni
fican
t red
uctio
n (3
.7%
in
I-gr
oup
vers
us 8
.8%
in C
-gro
up,
OR
= 0
.39
[95%
CI =
0.2
1–0.
77],
p
< 0.
05)
The
use
of p
re-p
rinte
d st
ruct
ured
ord
er fo
rms
sign
ifica
ntly
red
uces
med
icat
ion
erro
r rat
es a
nd s
ever
ity o
f the
er
rors
am
ong
paed
iatr
ic p
atie
nts
in th
e E
D
Lane
, 199
9
US
A
UB
A
Med
ical
-sur
gica
l/cr
itica
l ca
re p
atie
nts
N =
101
(ba
selin
e)N
= 9
8 (p
ost-
inte
rven
tion)
Per
iod
= 19
88 (
base
line)
, 19
95 (
post
-inte
rven
tion)
Aim
To e
valu
ate
the
effe
ctiv
enes
s of
a fa
lls p
reve
ntio
n pr
ogra
mm
e in
red
ucin
g pa
tient
fall
rate
Inte
rven
tio
nF
alls
pre
vent
ion
prog
ram
me,
in
clud
ing
:•
iden
tifyi
ng p
atie
nts
at r
isk
of fa
lling
• es
tabl
ishi
ng g
uide
lines
for
inte
rven
tions
pro
mot
ing
patie
nt s
afet
y fo
r pat
ient
s
at r
isk
Co
ntr
ol
NA
1. F
all r
ate
(fal
ls p
er
1,0
00
patie
nt d
ays)
2. In
jury
rat
e af
ter f
all
(num
ber o
f inj
urie
s pe
r 10
0 fa
lls)
Sta
tistic
al m
etho
dolo
gy is
unc
lear
1. N
o ch
ange
in fa
ll ra
te (
2.27
[b
asel
ine
] ver
sus
3.89
[pos
t-in
terv
entio
n],
p >
0.0
5)2.
Dec
reas
e in
inju
ry r
ate
(27.
7%
[bas
elin
e] v
ersu
s 8.
2% [p
ost-
inte
rven
tion
], p
-val
ue n
ot p
rovi
ded)
No
effe
ct o
f fal
ls p
reve
ntio
n pr
ogra
mm
e in
inpa
tient
s at
ris
k of
falli
ng

Dückers et al
Safety and risk management in hospitals
44
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
45
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Lars
en, 2
005
US
A
UB
A
Pae
diat
ric in
patie
nt c
are
N =
12,
109
infu
sion
dos
es
(pre
-inte
rven
tion)
N =
12,
377
infu
sion
dos
es
(pos
t-in
terv
entio
n)
Per
iod
= 20
02 (1
2 m
onth
s pr
e-in
terv
entio
n), 2
003
(12
mon
ths
post
-inte
rven
tion)
Aim
To d
eter
min
e if
com
bini
ng
stan
dard
dru
g co
ncen
trat
ions
w
ith s
mar
t-pu
mp
tech
nolo
gy
redu
ces
repo
rted
med
icat
ion-
infu
sion
err
ors
Inte
rven
tio
n1.
Sta
ndar
d dr
ug
conc
entr
atio
ns
deve
lopm
ent
2. ‘S
mar
t’ sy
ringe
pum
ps
sele
ctio
n cr
iteria
3. H
uman
-eng
inee
red
med
icat
ion
labe
ls r
epla
cing
ph
arm
acy-
gene
rate
d la
bels
Co
ntr
ol
NA
1. R
epor
ted
CM
I err
or
rate
(pe
r 1,0
00
dose
s)2.
Adh
eren
ce to
in
terv
entio
n
2-sa
mpl
e te
st o
f pro
port
ion
1. E
rror
rat
e de
crea
sed
from
3.1
to
0.8
per 1
,00
0 do
ses
(abs
olut
e ris
k re
duct
ion
= 2.
3 [9
5% C
I = 1
.1-3
.4],
p
< 0.
001
)2.
87%
of C
MIs
in n
eona
tal I
CU
s an
d >
99%
in o
ther
are
as o
f the
hos
pita
l us
ed s
tand
ard
drug
con
cent
ratio
ns
afte
r the
impl
emen
tatio
n
The
use
of s
tand
ard
drug
co
ncen
trat
ions
, sm
art s
yrin
ge
pum
ps a
nd u
ser-
frie
ndly
la
bels
red
uces
rep
orte
d er
rors
as
soci
ated
with
CM
Is. S
tand
ard
drug
con
cent
ratio
ns c
an b
e ch
osen
to a
llow
mos
t neo
nate
s to
rec
eive
nee
ded
med
icat
ions
w
ithou
t con
cern
s re
late
d to
ex
cess
flui
d ad
min
istr
atio
n
Leap
e, 1
999
US
A
CB
A
Inte
nsiv
e ca
re
Inte
rven
tion
(I) g
roup
:N
= 7
5 (p
re-in
terv
entio
n)N
= 7
5 (p
ost-
inte
rven
tion)
Con
trol
(C
) gro
up:
N =
50
(pre
-inte
rven
tion)
N =
75
(pos
t-in
terv
entio
n)
Per
iod
= F
ebru
ary
1993
–
July
199
3 (p
re-in
terv
entio
n),
Oct
ober
199
4 –
July
199
5 (p
ost-
inte
rven
tion)
Aim
To m
easu
re th
e ef
fect
of
phar
mac
ist p
artic
ipat
ion
on
med
ical
rou
nds
in th
e IC
U o
n th
e ra
te o
f pre
vent
able
AD
Es
caus
ed b
y or
derin
g er
rors
Inte
rven
tio
nS
enio
r pha
rmac
ist
part
icip
ates
in d
octo
rs’ r
ound
s (e
ach
mor
ning
), is
pre
sent
in
the
unit
for c
onsu
ltatio
n an
d as
sist
ance
to th
e nu
rsin
g st
aff
durin
g th
e re
st o
f the
mor
ning
, an
d is
ava
ilabl
e on
cal
l as
nece
ssar
y th
roug
hout
the
day
Co
ntr
ol
Usu
al p
ract
ice
whe
re th
e ph
arm
acis
t is
avai
labl
e in
the
unit
for p
art o
f the
day
, but
do
es n
ot m
ake
roun
ds
1. R
ate
of A
DE
s (p
er
1,0
00
patie
nt d
ays)
2. R
ate
of p
reve
ntab
le
AD
Es
in th
e or
derin
g st
age
(per
1,
00
0 pa
tient
day
s)3.
Acc
epta
nce
of in
terv
entio
n re
com
men
ded
by
the
phar
mac
ist
Unp
aire
d t-
test
1. S
igni
fican
t red
uctio
n (1
1.6
[I-g
roup
, af
ter]
ver
sus
46.6
[C-g
roup
, aft
er],
p
< 0.
001
)2.
Sig
nific
ant r
educ
tion
(3.5
[I-g
roup
, af
ter]
ver
sus
12.4
[C-g
roup
, aft
er],
p
< 0.
001
)3.
Maj
ority
(36
6 of
398
) of t
he
phar
mac
ist i
nter
vent
ions
wer
e re
late
d to
dru
g or
derin
g, o
f whi
ch
362
(99
%) w
ere
acce
pted
by
doct
ors
Pre
senc
e of
pha
rmac
ist w
as
asso
ciat
ed w
ith a
sub
stan
tially
lo
wer
AD
E r
ate
and
high
ac
cept
ance
rat
e
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
46
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
47
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Lehm
ann,
20
07
US
A
ITS
(bu
t ana
lyse
d as
UB
A)
Med
ical
uni
vers
ity h
ospi
tal
N =
1 h
ospi
tal
Per
iod
= O
ctob
er 1
999
– A
pril
2007
(in
terv
entio
n st
arte
d in
Oct
ober
20
00
)
Aim
Dev
elop
men
t of a
non
-pu
nitiv
e re
port
ing
syst
em
and
CP
OE
to d
ecre
ase
the
pote
ntia
l for
dru
g ha
rm
Inte
rven
tio
n•
Str
ateg
y se
ssio
ns w
ith
seni
or m
anag
emen
t abo
ut
non-
puni
tive
repo
rtin
g (A
utum
n 19
99)
• R
evis
ed m
edic
atio
n ev
ent
repo
rtin
g po
licy
(Oct
ober
20
00
)•
Impl
emen
tatio
n of
CP
OE
th
roug
hout
the
orga
nisa
tion
(Dec
embe
r 20
05)
Co
ntr
ol
NA
1. T
he n
umbe
r of e
rror
re
port
s re
ceiv
ed
per m
onth
2. T
he ty
pe o
f re
port
ed e
rror
s
AN
OV
A
1. S
igni
fican
t inc
reas
e (1
9 re
port
s be
fore
inte
rven
tion
star
ted
vers
us
102
repo
rts
afte
r sta
rt, p
< 0
.001
)2.
The
type
of r
epor
ted
erro
rs
chan
ged.
In p
re-in
terv
entio
n ph
ase,
maj
ority
of r
epor
ted
inci
dent
s oc
curr
ed a
fter
med
icat
ion
adm
inis
trat
ion,
lead
ing
to a
ctua
l pa
tient
har
m o
r del
ayed
car
e. In
po
st-in
terv
entio
n ph
ase,
maj
ority
of
rep
orte
d er
rors
occ
urre
d du
ring
med
icat
ion-
use
proc
esse
s be
fore
ac
tual
dru
g ad
min
istr
atio
n
Sig
nific
ant i
ncre
ase
in th
e nu
mbe
r of r
epor
ts a
nd
subs
tant
ial c
hang
e in
type
of
repo
rted
err
ors

Dückers et al
Safety and risk management in hospitals
46
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
47
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Man
ning
, 20
07
US
A
RC
T
Hos
pita
l dis
char
ge p
atie
nts
N =
138
Per
iod
= M
ay 2
004
–
Feb
ruar
y 20
05
Aim
To d
eter
min
e w
heth
er th
e 3D
m
edic
atio
n di
scha
rge
form
, re
lativ
e to
MD
W, r
educ
es
self-
repo
rted
med
icat
ion
erro
rs a
nd im
prov
es
patie
nt s
atis
fact
ion
and
unde
rsta
ndin
g
Inte
rven
tio
nA
new
edu
catio
n to
ol (
3D).
F
eatu
res
incl
ude:
1. S
pace
in w
hich
a ta
blet
or
pill
is a
ffix
ed a
nd d
ispl
ayed
2. T
rade
nam
e3.
Uni
t str
engt
h4.
Num
ber (
and
/or f
ract
ion)
of
units
to b
e ta
ken
5. P
urpo
se (
indi
catio
n)6.
Com
men
t/ca
utio
n7.
Lar
ger f
ont
8. C
ard
stoc
k du
rabi
lity
9. A
rec
onci
liatio
n fe
atur
e
Co
ntr
ol
Sta
ndar
d M
DW
1. N
umbe
r of
self-
repo
rted
m
edic
atio
n er
rors
2. P
atie
nt s
atis
fact
ion
with
dis
char
ge fo
rm3.
Pat
ient
un
ders
tand
ing
of p
resc
ribed
m
edic
atio
n in
stru
ctio
ns
T-te
st a
nd M
ann-
Whi
tney
U-t
est
1. N
o ef
fect
(I-
grou
p ve
rsus
C-g
roup
=
0.78
[SD
= 0
.42
] ver
sus
0.79
[SD
=
0.41
], p
= 0
.876
)2.
No
effe
ct (
I = g
roup
ver
sus
C-g
roup
=
4.24
[SD
= 0
.70
] ver
sus
4.26
[SD
=
0.88
], p
= 0
.520
4)3.
Bet
ter u
nder
stan
ding
of m
edic
atio
n in
stru
ctio
ns (
I-gr
oup
vers
us
C-g
roup
= 1
.96
[SD
= 0
.76
] ver
sus
1.66
[SD
= 0
.69
], p
= 0
.028
2)
Bot
h to
ols
are
asso
ciat
ed w
ith
high
leve
ls o
f pat
ient
sat
isfa
ctio
n an
d lo
w r
ates
of s
elf-
repo
rted
m
edic
atio
n er
ror.
3D a
ppea
rs to
pr
omot
e pa
tient
und
erst
andi
ng
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
48
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
49
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Pao
lett
i, 20
07
US
A
CB
A
Inpa
tient
nur
sing
uni
ts
Inte
rven
tion
1 (c
ardi
ac
tele
met
ry u
nit)
:N
= 3
08 d
oses
(p
re-in
terv
entio
n)
N =
318
dos
es (
post
-in
terv
entio
n)
Inte
rven
tion
2 (m
edic
al-
surg
ical
uni
t):
N =
320
dos
es
(pre
-inte
rven
tion)
N =
310
dos
es (
post
-in
terv
entio
n)
Con
trol
(ca
rdia
c te
lem
etry
un
it):
N =
30
6 do
ses
(pre
-inte
rven
tion)
N
= 3
06
dose
s (p
ost-
inte
rven
tion)
Per
iod
= 20
03–2
005
(im
plem
enta
tion
perio
d =
Aug
ust 2
003
– J
uly
2004
)
Aim
The
impl
emen
tatio
n of
a
mul
tidis
cipl
inar
y ap
proa
ch
to s
yste
mat
ical
ly d
ecre
ase
med
icat
ion
erro
rs
Inte
rven
tio
nT
he u
se o
f obs
erva
tion
met
hodo
logy
, ele
ctro
nic
med
icat
ion-
adm
inis
trat
ion
reco
rds
and
bar-
code
d m
edic
atio
n ad
min
istr
atio
n
Co
ntr
ol
Usu
al c
are
1. M
edic
atio
n er
ror
rate
2. A
ccur
acy
rate
of
med
icat
ion
adm
inis
trat
ion
Sta
tistic
al m
etho
dolo
gy is
unc
lear
1. M
edic
atio
n er
ror r
ates
dec
reas
ed
(-35
.9%
cha
nge
from
bas
elin
e,
p =
0.03
5) in
inte
rven
tion
grou
p 2,
was
unc
hang
ed in
inte
rven
tion
grou
p 1
(-24
.1%
cha
nge
from
ba
selin
e, p
= 0
.065
) and
was
un
chan
ged
in c
ontr
ol g
roup
(5.
1%
chan
ge fr
om b
asel
ine,
p =
0.7
62).
2.
Impr
oved
acc
urac
y ra
te (
86.5
%
befo
re v
ersu
s 97
% a
fter
, p-v
alue
no
t pro
vide
d)
Mul
tidis
cipl
inar
y ap
proa
ch
redu
ced
erro
r rat
es, b
ut d
id n
ot
reac
h st
atis
tical
sig
nific
ance

Dückers et al
Safety and risk management in hospitals
48
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
49
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Ple
ws-
Oga
n,
2004
US
A
UB
A
Am
bula
tory
inte
rnal
m
edic
ine
prac
tice
N =
NC
Per
iod
= 1
year
bef
ore
and
1 ye
ar a
fter
the
impl
emen
tatio
n
Aim
To d
eter
min
e th
e fe
asib
ility
an
d ef
fect
iven
ess
of c
linic
ian-
base
d ne
ar m
iss/
AE
vol
unta
ry
repo
rtin
g, c
oupl
ed w
ith
syst
em a
naly
sis
and
rede
sign
as
a m
odel
for c
ontin
uous
qu
ality
impr
ovem
ent i
n th
e am
bula
tory
set
ting
Inte
rven
tio
n•
Rep
ortin
g sy
stem
for n
ear
mis
s or
AE
s•
Roo
t cau
se a
naly
sis
by
com
mitt
ee•
Impr
ovem
ents
of p
ract
ice,
ed
ucat
ion,
sys
tem
s an
d eq
uipm
ent
Co
ntr
ol
NA
1. C
linic
al-b
ased
nea
r m
isse
s an
d A
Es
2. T
ype
of r
epor
ter
3. T
ype
of e
rror
4. A
ccep
tanc
e of
re
com
men
datio
ns
Sta
tistic
al m
etho
dolo
gy is
unc
lear
1. N
umbe
r of r
epor
ts in
crea
sed
from
5
to 1
00
repo
rts
(incl
udin
g 83
nea
r m
isse
s an
d 17
AE
s)2.
44%
of t
he e
vent
s w
ere
repo
rted
by
doct
ors,
22%
by
resi
dent
s, 3
1% b
y nu
rses
and
3%
by
man
ager
s3.
Err
ors
invo
lved
med
icat
ion
(47%
), la
b or
X-r
ay (
22%
),
offic
e ad
min
istr
atio
n (2
1%) a
nd
com
mun
icat
ion
proc
esse
s (1
0%
)4.
75%
of r
ecom
men
datio
ns w
ere
impl
emen
ted
durin
g th
e st
udy
perio
d
The
inte
rven
tion
was
eff
ectiv
e in
incr
easi
ng e
rror
rep
ortin
g an
d in
pro
mot
ing
syst
em c
hang
e to
im
prov
e ca
re a
nd p
reve
nt e
rror
s
Poo
n, 2
00
6
US
A
UB
A
Tert
iary
car
e (7
35-b
ed)
acad
emic
med
ical
cen
tre
N =
155
,16
4 (p
re-
inte
rven
tion)
and
253
,98
4 (p
ost-
inte
rven
tion)
di
spen
sed
med
icat
ion
dose
s
Per
iod
= 20
03–2
004
(20
m
onth
s)
Aim
Red
uctio
n in
dis
pens
ing
erro
rs a
nd p
oten
tial A
DE
s by
ba
r-co
de te
chno
logy
Inte
rven
tio
nA
bar
-cod
e-a
ssis
ted
stor
age
and
retr
ieva
l sys
tem
im
plem
ente
d in
thre
e co
nfig
urat
ions
(in
two,
all
dose
s w
ere
scan
ned
once
du
ring
the
disp
ensi
ng p
roce
ss
and
in o
ne, a
dos
e w
as
scan
ned
if se
vera
l dos
es o
f th
e sa
me
med
icat
ion
wer
e be
ing
disp
ense
d)
Co
ntr
ol
NA
Pri
mar
y o
utc
om
es1.
Tar
get d
ispe
nsin
g er
ror r
ate
2. T
arge
t pot
entia
l A
DE
s ra
te
Sec
on
dar
y o
utc
om
e3.
Nat
ure
of ta
rget
er
rors
Fis
her e
xact
test
Ove
rall
effe
ct, a
cros
s th
e th
ree
conf
igur
atio
ns:
1. 8
5% r
educ
tion
(err
or r
ate
pre
= 0.
37%
ver
sus
post
= 0
.06%
)2.
74%
red
uctio
n (A
DE
rat
e pr
e =
0.17
% v
ersu
s po
st =
0.0
4%)
3. D
ecre
ase
in w
rong
med
icat
ion
erro
r ra
te (
56%
red
uctio
n)
Sub
stan
tial d
ecre
ase
in
disp
ensi
ng e
rror
s an
d po
tent
ial
AD
Es
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
50
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
51
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Ram
nara
yan,
20
06a
Uni
ted
Kin
gdom
UB
A
Pae
diat
ric e
mer
genc
y ro
om
N =
751
cas
e ep
isod
es,
hand
led
by 7
6 do
ctor
s (ie
co
nsul
tant
, reg
istr
ar, s
enio
r ho
use
offic
er o
r stu
dent
)
Per
iod
= F
ebru
ary
– A
ugus
t 20
02
Aim
To a
sses
s th
e im
pact
of a
no
vel d
iagn
ostic
rem
inde
r sy
stem
(IS
AB
EL)
on
the
qual
ity o
f clin
ical
dec
isio
ns
mad
e by
var
ious
gra
des
of c
linic
ians
dur
ing
acut
e as
sess
men
t
Inte
rven
tio
nW
eb-b
ased
dia
gnos
tic
rem
inde
r sys
tem
that
su
gges
ts im
port
ant d
iagn
oses
du
ring
clin
ical
ass
essm
ent,
ie
a C
DS
S
Co
ntr
ol
NA
Pri
mar
y o
utc
om
e1.
Num
ber o
f di
agno
stic
err
ors
of
omis
sion
Sec
on
dar
y o
utc
om
es2.
Qua
lity
of
diag
nost
ic te
st
orde
ring
and
trea
tmen
t pla
n3.
Num
ber o
f irr
elev
ant
diag
nose
s co
ntai
ned
with
in th
e di
agno
stic
wor
kup
4. P
ropo
rtio
n of
ca
se e
piso
des
in w
hich
at l
east
on
e ad
ditio
nal
‘impo
rtan
t’ di
agno
sis,
test
or
trea
tmen
t dec
isio
n w
as c
onsi
dere
d by
the
doct
or a
fter
C
DS
S c
onsu
ltatio
n5.
Add
ition
al ti
me
take
n fo
r CD
SS
co
nsul
tatio
n
Two
-way
mix
ed-m
odel
AN
OV
A
1. S
igni
fican
t red
uctio
n (5
.5 [S
D =
1.6
] er
rors
bef
ore
vers
us 5
.0 [S
D =
1.5
] er
rors
aft
er, p
< 0
.001
)2.
Mea
n di
agno
stic
qua
lity
scor
e in
crea
sed
sign
ifica
ntly
(in
crea
se =
0.
044,
95%
CI =
0.0
32–
0.05
4,
p <
0.0
01).
Als
o qu
ality
of t
est-
orde
ring
plan
s an
d tr
eatm
ent p
lan
impr
oved
sig
nific
antly
3. N
umbe
r of i
rrel
evan
t dia
gnos
es
incr
ease
d fr
om 0
.7 to
1.4
(in
crea
se
= 0.
7, 9
5% C
I = 0
.5–
0.75
), b
ut
num
ber o
f irr
elev
ant o
r del
eter
ious
te
sts
and
trea
tmen
ts r
emai
ned
unch
ange
d4.
In 1
2.5%
of c
ases
at l
east
one
di
agno
stic
dec
isio
n w
as a
dded
; in
9.3%
of c
ases
one
test
dec
isio
n w
as a
dded
; in
6.5%
one
trea
tmen
t st
ep w
as a
dded
5. M
edia
n ad
ditio
nal t
ime
take
n fo
r C
DD
S c
onsu
ltatio
n w
as 1
min
(IQ
R
= 30
sec
–2 m
in 4
sec
)
The
pro
visi
on o
f pat
ient
- and
co
ntex
t-sp
ecifi
c re
min
ders
re
duce
d di
agno
stic
om
issi
ons
acro
ss a
ll su
bjec
t gra
des
for a
ra
nge
of c
ases
, and
incr
ease
d di
agno
stic
and
trea
tmen
t qua
lity,
w
ithou
t a la
rge
incr
ease
in
wor
kloa
d

Dückers et al
Safety and risk management in hospitals
50
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
51
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Ram
nara
yan,
20
06b
Uni
ted
Kin
gdom
UB
A
Acu
te a
mbu
lato
ry p
aedi
atric
ca
re
N =
177
pat
ient
s, a
cros
s 4
care
uni
ts
Per
iod
= D
ecem
ber 2
002
–
Apr
il 20
03
Aim
To e
xam
ine
the
impa
ct o
f a
web
-bas
ed d
iagn
ostic
re
min
der s
yste
m o
n cl
inic
ians
’ de
cisi
ons
in a
n ac
ute
paed
iatr
ic s
ettin
g du
ring
asse
ssm
ents
cha
ract
eris
ed
by d
iagn
ostic
unc
erta
inty
Inte
rven
tio
nC
DS
S fo
r dia
gnos
tics
Co
ntr
ol
NA
Pri
mar
y o
utc
om
e 1.
Pro
port
ion
of
‘uns
afe’
dia
gnos
tic
wor
kups
follo
win
g C
DS
S c
onsu
ltatio
n
Sec
on
dar
y o
utc
om
es2.
Qua
lity
scor
es fo
r di
agno
stic
wor
kup
and
clin
ical
act
ion
plan
s3.
Tim
e ta
ken
by s
ubje
cts
to
com
plet
e C
DS
S
usag
e4.
Num
ber o
f di
agno
ses
incl
uded
in
the
diag
nost
ic
asse
ssm
ent
McN
emar
test
for p
aire
d pr
opor
tions
1. S
igni
fican
t dec
reas
e (4
5.2%
uns
afe
wor
kups
bef
ore
and
32.7
% u
nsaf
e w
orku
ps a
fter
CD
SS
con
sulta
tion,
p
< 0.
001
)2.
Dia
gnos
tic q
ualit
y sc
ores
incr
ease
d by
6.8
6 po
ints
(95
% C
I = 4
.0–
9.7)
af
ter C
DS
S c
onsu
ltatio
n. C
linic
al
plan
sco
res
impr
ovem
ent w
as
smal
ler i
n m
agni
tude
(1.5
poi
nts
incr
ease
, SD
= 6
.7)
3. M
edia
n tim
e sp
ent o
n th
e C
DS
S =
1
min
38
sec
(IQ
R =
50
sec–
3 m
in
21 s
ec)
4. N
umbe
r of d
iagn
oses
incr
ease
d fr
om 2
.2 to
3.2
, whe
reas
num
ber o
f te
sts
orde
red
rose
from
2.7
to 2
.9
The
qua
lity
of d
iagn
ostic
s im
prov
ed s
igni
fican
tly a
nd
diag
nost
ic o
mis
sion
err
ors
wer
e re
duce
d
Rob
inso
n, 2
00
6
US
A
UB
A
Pae
diat
ric o
ncol
ogy
N =
NC
Per
iod
= 20
01–2
004
(in
terv
entio
n in
20
02)
Aim
To a
sses
s th
e im
pact
of
iden
tifyi
ng th
e el
emen
ts
of r
isk
and
impl
emen
ting
appr
opria
te s
trat
egie
s
Inte
rven
tio
nU
se o
f fai
lure
mod
e an
d ef
fect
s an
alys
is (
FM
EA
) to
iden
tify
risk
and
for
impl
emen
ting
stra
tegi
es.
Str
ateg
ies
coul
d be
im
plem
ente
d in
thre
e ar
eas:
1. P
resc
ribin
g pr
oces
s2.
Dis
pens
ing
proc
ess
3. A
dmin
istr
atio
n pr
oces
s
Co
ntr
ol
NA
1. P
resc
ribin
g er
ror
rate
2. D
ispe
nsin
g er
ror
rate
3. A
dmin
istr
atio
n er
ror
rate
4. U
sage
rat
e of
re
prin
ted
stan
dard
or
der s
ets
Sta
tistic
al m
etho
dolo
gy is
unc
lear
1. T
he p
oten
tial p
resc
ribin
g er
ror r
ate
decr
ease
d fr
om 2
3% to
14%
2. A
ctua
l dis
pens
ing
erro
rs d
ecre
ased
fr
om 3
to 1
3. A
ctua
l adm
inis
trat
ion
erro
rs
decr
ease
d fr
om 4
to 3
4. U
se o
f rep
rinte
d st
anda
rd o
rder
se
ts in
crea
sed
from
22%
to 4
5% in
20
03 a
nd 7
6% in
20
05
The
CP
OE
sys
tem
, whi
ch w
as
desi
gned
bas
ed o
n an
FM
EA
, im
prov
es th
e pr
escr
ibin
g st
age
of th
e ch
emot
hera
py p
roce
ss
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
52
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
53
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Sch
neid
er,
200
6
US
A
RC
T
3 co
mm
unity
hos
pita
ls
N =
30
nurs
es (1
5 in
in
terv
entio
n an
d 15
in
cont
rol g
roup
)
Per
iod
= 6
wee
ks
(1 w
eek
base
line,
2
wee
ks a
fter
com
plet
ion
of th
e in
terv
entio
n/p
ost-
inte
rven
tion
asse
ssm
ent)
Aim
To e
xam
ine
the
impa
ct o
f an
inte
ract
ive
CD
-RO
M
prog
ram
me
on th
e ra
te o
f m
edic
atio
n ad
min
istr
atio
n er
rors
mad
e by
nur
ses
Inte
rven
tio
nE
duca
tiona
l CD
-RO
M: B
asic
M
edic
atio
n A
dmin
istr
atio
n
Co
ntr
ol
Usu
al c
are;
no
inte
rven
tion
1. E
rror
rat
e du
e to
de
viat
ion
from
sa
fe a
dmin
istr
atio
n pr
actic
es2.
Pre
para
tion
and
adm
inis
trat
ion
erro
r ra
te3.
Err
or r
ate
due
to
devi
atio
ns fr
om
pres
crib
ed th
erap
y
AN
OV
A a
nd lo
gist
ic r
egre
ssio
n an
alys
is
1. S
igni
fican
t dec
reas
e (O
R =
0.3
8 [9
5% C
I = 0
.19
–0.
74],
p =
0.0
04)
2. E
rror
rat
es in
crea
sed
(OR
= 1
.92
[95%
CI =
0.8
1–4.
58],
p =
0.1
4)3.
No
diff
eren
ce in
err
or r
ate
betw
een
grou
ps (
OR
= 1
.03
[95%
CI =
0.
23–
4.62
], p
= 0
.97)
An
inte
ract
ive
CD
-RO
M e
nabl
ed
nurs
es to
app
ly th
e in
form
atio
n le
arne
d to
iden
tify
erro
rs in
m
edic
atio
n ad
min
istr
atio
n an
d to
impr
ove
adhe
renc
e to
saf
e m
edic
atio
n ad
min
istr
atio
n pr
actic
es. O
ther
cat
egor
ies
of m
edic
atio
n er
rors
wer
e no
t af
fect
ed
Sch
wen
dim
ann,
20
06
Sw
itzer
land
ITS
Inte
rnal
med
icin
e, g
eria
tric
an
d su
rger
y in
patie
nt
depa
rtm
ents
N =
34,
972
patie
nts
Per
iod
= 19
99–2
003
(60
m
onth
s) w
ith in
terv
entio
n st
artin
g in
20
00
Aim
To e
xam
ine
inpa
tient
fall
rate
s an
d co
nseq
uent
in
jurie
s be
fore
and
aft
er
the
impl
emen
tatio
n of
th
e in
terd
isci
plin
ary
falls
pr
even
tion
prog
ram
me
(IF
P)
Inte
rven
tio
nIF
P:
• S
cree
ning
of a
ll pa
tient
s at
adm
issi
on fo
r ris
k of
fa
lls•
Exa
min
atio
n of
pat
ient
s co
nsid
ered
at r
isk
of
falli
ng•
Inte
rven
tions
for a
ll pa
tient
s to
pro
vide
saf
ety
in th
e ho
spita
l•
Inte
rven
tion
in p
atie
nts
cons
ider
ed a
t ris
k of
fa
lling
• R
eass
essm
ent o
f tho
se
patie
nts
who
fell
Co
ntr
ol
NA
1. In
patie
nt fa
ll ra
te
(per
1,0
00
patie
nt
days
)2.
Con
sequ
ent i
njur
y ra
te (
per y
ear)
Gen
eral
line
ar m
odel
, AN
OV
A,
Chi
-squ
are
test
1. F
all r
ates
fluc
tuat
ed fr
om 9
.1 fa
lls
per 1
,00
0 pa
tient
day
s in
the
first
ha
lf of
199
9 to
8.6
falls
in th
e se
cond
hal
f of 2
003
(p
= 0.
086
)2.
Ann
ual p
ropo
rtio
n of
min
or in
jurie
s de
crea
sed
from
32.
6% in
199
9 to
28.
1% in
20
03 (
p =
0.01
5) a
nd
annu
al p
ropo
rtio
n of
maj
or in
jurie
s in
crea
sed
from
2.5
% in
199
9 to
3.
9%
in 2
003
(p
= 0.
014)
Fal
l rat
es d
id n
ot c
hang
e af
ter
the
impl
emen
tatio
n of
the
IFP,
w
here
as m
inor
inju
ry r
ate
decr
ease
d an
d m
ajor
inju
ry r
ate
incr
ease
d

Dückers et al
Safety and risk management in hospitals
52
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
53
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Sha
mliy
an,
2007
Wor
ldw
ide
Rev
iew
Set
ting
: In
patie
nt (
N=
10),
out
patie
nt
(N =
1),
em
erge
ncy
depa
rtm
ent (
N =
1)
Num
ber o
f inc
lude
d st
udie
s:N
= 1
2 (1
RC
T, 9
UB
A a
nd 2
un
clea
r)
Sea
rch
perio
d: 1
990
–20
05
Eng
lish
Cou
ntrie
s: n
o re
stric
tions
Aim
To te
st th
e hy
poth
esis
th
at m
edic
atio
n er
rors
an
d ad
vers
e cl
inic
al
even
ts d
ecre
ase
afte
r co
mpu
teris
atio
n co
mpa
red
with
han
dwrit
ten
phys
icia
n or
ders
in p
aedi
atric
and
ad
ult p
atie
nts,
inde
pend
ent
of p
atie
nt a
nd p
rovi
der
char
acte
ristic
s
Inte
rven
tio
nC
PO
E s
yste
m C
on
tro
lH
andw
ritte
n ph
ysic
ian
orde
rs
1. M
edic
atio
n er
rors
2. W
rong
dru
g du
e to
pr
escr
ibin
g er
rors
3. W
rong
dos
e du
e to
pr
escr
ibin
g er
rors
4. A
DE
s
Met
a-an
alys
is w
ith fi
xed
and
rand
om
effe
cts
mod
els
1. S
igni
fican
t red
uctio
n (p
oole
d O
R =
0.
14 [9
5% C
I = 0
.05
–0.
43])
2. N
o ch
ange
(po
oled
OR
= 0
.80
[9
5% C
I = 0
.27–
2.36
])3.
Sig
nific
ant r
educ
tion
(poo
led
OR
=
0.44
[95%
CI =
0.2
3–
0.85
])4.
Sig
nific
ant r
educ
tion
(poo
led
OR
=
0.52
[95%
CI =
0.3
0–
0.91
])
Impl
emen
tatio
n of
CP
OE
was
as
soci
ated
with
a s
igni
fican
t re
duct
ion
in m
edic
atio
n er
rors
. R
esul
ts s
houl
d be
inte
rpre
ted
with
cau
tion:
pos
sibl
e ov
eres
timat
ion
due
to u
sing
no
n-ra
ndom
ised
unc
ontr
olle
d in
terv
entio
ns. U
se o
f CP
OE
not
as
soci
ated
with
a s
ubst
antia
l im
prov
emen
t in
patie
nt s
afet
y.
Stu
dies
do
not a
llow
bro
ad
gene
ralis
abili
ty
Silv
er, 2
00
0
US
A
UB
A
Acu
te c
are
hosp
itals
Bas
elin
e: 1
2 ho
spita
ls, 3
41
com
plet
ed s
urve
ysF
ollo
w-u
p: 9
hos
pita
ls, 2
19
com
plet
ed s
urve
ys
Per
iod
= A
utum
n 19
97
(bas
elin
e), A
utum
n 19
98
(fol
low
-up)
Aim
Im
prov
e th
e ho
spita
l’s
med
icat
ion
syst
em, i
n or
der t
o re
duce
med
icat
ion
erro
r rat
es
Inte
rven
tio
nB
reak
thro
ugh
Ser
ies
mod
el:
• te
ams
(QI,
phar
mac
y,
med
ical
sta
ff)
• im
prov
ing
info
rmat
ion
acce
ss•
stan
dard
isin
g an
d si
mpl
ifyin
g m
edic
atio
n pr
oced
ures
• re
stric
ting
phys
ical
ac
cess
to p
oten
tially
le
thal
dru
gs•
educ
atin
g cl
inic
al s
taff
ab
out m
edic
atio
ns•
QI f
acili
tato
rs•
enha
nced
err
or r
epor
ting
Co
ntr
ol
NA
A. R
espo
nden
t ob
serv
ing
med
icat
ion
erro
r:1.
All
erro
rs2.
Med
iatio
n or
derin
g3.
Tra
nscr
iptio
n an
d ve
rific
atio
n4.
Dis
pens
ing
and
deliv
ery
5. M
edic
atio
n ad
min
istr
atio
n
B. R
espo
nden
t in
dica
ting
erro
rs
wer
e di
scov
ered
and
pr
even
ted
C. R
espo
nden
t in
dica
ting
mos
t rec
ent
obse
rved
err
or w
as
repo
rted
:1.
All
erro
rs2.
Err
or r
each
ing
the
patie
nt
Logi
stic
reg
ress
ion,
with
pos
t-ho
c an
alys
is
A1:
sig
n –
decr
ease
from
20.
8% to
15
.2%
(O
R =
0.6
2, p
= 0
.00
6)
A2
: non
-sig
n –
decr
ease
from
23.
0%
to
16.
4% (
OR
= 0
.63,
p =
0.0
68)
A3
: sig
n –
decr
ease
from
24.
4% to
15
.7%
(O
R =
0.4
7, p
= 0
.003
)
A4:
non
-sig
n –
decr
ease
from
20.
2%
to 1
6.2%
(O
R =
0.6
8, p
= 0
.127
)
A5
: non
-sig
n –
decr
ease
from
15.
5%
to 1
2.5%
(O
R =
0.7
3, p
= 0
.278
)
B: s
ign
– in
crea
se fr
om 5
1.2%
to
57.6
% (
OR
= 1
.32,
p =
0.0
32)
C1:
non
-sig
n –
incr
ease
from
29.
0%
to
32.3
% (
OR
= 1
.16,
p =
0.3
37)
C2
: sig
n –
incr
ease
from
43.
9%
to
54.
5% (
OR
= 1
.67,
p =
0.0
13)
Sur
vey
resu
lts s
ugge
st th
at th
e ch
ange
s im
plem
ente
d in
the
orga
nisa
tions
may
hav
e re
duce
d m
edic
atio
n er
rors
and
impr
oved
ca
paci
ty fo
r err
or d
etec
tion
and
prev
entio
n
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
54
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
55
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Sim
, 20
02
US
A
UB
A
Com
mun
ity h
ospi
tal w
ith a
w
ide
varie
ty o
f acu
te c
are,
cr
itica
l car
e, e
mer
genc
y ca
re a
nd s
urgi
cal a
nd
diag
nost
ic s
ervi
ces
N =
NC
Per
iod
= M
ay 2
001
–
Janu
ary
2002
(9
mon
ths)
Aim
To a
ddre
ss m
edic
atio
n-re
late
d pa
tient
saf
ety
initi
ativ
es
Inte
rven
tio
nA
mul
tidis
cipl
inar
y te
am
was
form
ed to
add
ress
m
edic
atio
n-re
late
d pa
tient
sa
fety
initi
ativ
es, f
ocus
ing
on:
• le
ader
ship
• st
rate
gic
plan
ning
• an
alys
es o
f AE
s•
fost
erin
g ef
fect
ive
team
wor
k•
impr
ovin
g ca
re-d
eliv
ery
proc
esse
s •
enga
ging
pat
ient
s in
car
e de
liver
y
Co
ntr
ol
NA
Num
ber o
f rep
orts
of
med
icat
ion
varia
nces
Sta
tistic
al m
etho
dolo
gy n
ot r
epor
ted
The
num
ber o
f rep
orts
dou
bled
With
in a
nin
e-m
onth
per
iod
the
num
ber o
f var
ianc
e re
port
s do
uble
d. A
sub
com
mitt
ee
was
form
ed w
ith th
e sp
ecifi
c re
spon
sibi
lity
of r
evie
win
g th
e re
port
s on
a w
eekl
y ba
sis
Sim
on, 2
005
US
A, U
nite
d K
ingd
om,
Aus
tral
ia, H
ong
Kon
g/C
hina
, C
anad
a
Rev
iew
Num
ber o
f inc
lude
d st
udie
s:N
= 1
1 (4
con
trol
led
obse
rvat
iona
l stu
dies
and
7
unco
ntro
lled
obse
rvat
iona
l st
udie
s)
Sea
rch
perio
d =
1994
–20
04
Lang
uage
: Eng
lish
Aim
To a
sses
s th
e ef
fect
iven
ess
of h
ospi
tal i
ncid
ent r
epor
ting
syst
ems
in im
prov
ing
hosp
ital
and
clin
ic p
erfo
rman
ce
in te
rms
of p
atie
nt s
afet
y,
clin
ical
out
com
e, c
osts
and
op
erat
ions
Inte
rven
tio
nIn
cide
nt r
epor
ting
syst
ems
Co
ntr
ol
No
inci
dent
rep
ortin
g sy
stem
; us
ual c
are
1. M
edic
al e
rror
s2.
AE
s3.
Acc
urac
y of
in
cide
nt r
epor
ting
syst
ems
Nar
rativ
e an
alys
is
1.+
2. M
ajor
ity o
f the
stu
dies
(7
out
of 1
1) r
epor
ted
no r
educ
tion
in
med
ical
err
ors
and
AE
s af
ter
impl
emen
tatio
n of
inci
dent
rep
ortin
g sy
stem
s 3.
Inci
dent
rep
ortin
g an
d ch
art-
revi
ew
dete
ctio
n ar
e le
ss a
ccur
ate
than
di
rect
obs
erva
tion
Inci
dent
rep
ortin
g ca
n pr
ovid
e va
luab
le q
ualit
ativ
e an
d qu
antit
ativ
e da
ta r
elev
ant
to in
cide
nts
and
AE
s, w
hich
in
turn
can
pot
entia
lly g
uide
or
gani
satio
nal a
nd c
linic
al
inte
rven
tions
to d
ecre
ase
risks
. How
ever
, the
ben
efits
of
inci
dent
rep
ortin
g ar
e no
t wel
l es
tabl
ishe
d

Dückers et al
Safety and risk management in hospitals
54
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
55
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Sim
pson
, 20
04
Uni
ted
Kin
gdom
ITS
Neo
nata
l IC
U
N =
NC
Per
iod
= Ja
nuar
y 20
02 –
Ja
nuar
y 20
03
Aim
To d
escr
ibe
the
med
icat
ion
erro
rs o
ccur
ring
with
in a
ne
onat
al IC
U, a
nd a
sses
s th
e im
pact
of a
com
bine
d ris
k m
anag
emen
t/cl
inic
al
phar
mac
ist-
led
educ
atio
n pr
ogra
mm
e on
thes
e er
rors
Inte
rven
tio
nC
ombi
ned
risk
man
agem
ent/
clin
ical
pha
rmac
ist-
led
educ
atio
n pr
ogra
mm
e
Co
ntr
ol
NA
1. M
edic
atio
n er
ror
rate
(pe
r 1,0
00
activ
ity d
ays)
2. M
edic
atio
n er
ror
type
3. M
edic
atio
n er
ror
caus
e
Stu
dent
’s t-
test
1. M
onth
ly m
edic
atio
n er
ror r
ates
fell
from
a m
ean
(SD
) of 2
4.1
(1.7
) per
1,
00
0 ne
onat
al a
ctiv
ity d
ays
to 5
.1
(3.6
) per
1,0
00
days
(p
< 0.
001
) in
the
follo
win
g th
ree
mon
ths.
T
he s
ubse
quen
t cha
nge
of ju
nior
m
edic
al s
taff
was
ass
ocia
ted
with
a
sign
ifica
nt in
crea
se in
med
icat
ion
erro
rs to
12.
2 (3
.6) p
er 1
,00
0 ne
onat
al a
ctiv
ity d
ays
(p =
0.0
37)
2. A
tota
l of 1
05 e
rror
s w
ere
iden
tifie
d:
4 se
rious
, 45
pote
ntia
lly s
erio
us
and
56 m
inor
. The
4 s
erio
us
erro
rs in
clud
ed tw
o te
nfol
d do
se
mis
calc
ulat
ions
3.
Mos
t (71
%) o
f the
err
ors
wer
e du
e to
poo
r pre
scrib
ing
The
inte
rven
tion,
with
in th
e co
ntex
t of a
ris
k m
anag
emen
t pr
ogra
mm
e, is
eff
ectiv
e in
re
duci
ng m
edic
atio
n er
ror r
ates
Sni
jder
s, 2
007
Wor
ldw
ide
Rev
iew
Neo
nata
l IC
U
Num
ber o
f inc
lude
d st
udie
s:N
= 1
0 (8
pro
spec
tive
stud
ies
and
2 re
tros
pect
ive
stud
ies)
Sea
rch
perio
d: J
anua
ry
1980
– J
anua
ry 2
00
6
Lang
uage
s: E
nglis
h,
Ger
man
, Dut
ch, F
renc
h
Aim
To e
xam
ine
the
char
acte
ristic
s of
inci
dent
re
port
ing
syst
ems
in n
eona
tal
ICU
s in
rel
atio
n to
type
, ae
tiolo
gy, o
utco
me
and
prev
enta
bilit
y of
inci
dent
s
Inte
rven
tio
nV
ario
us m
odes
of i
ncid
ent
repo
rtin
g sy
stem
s
Co
ntr
ol
NC
Cha
ract
eris
tics
of
inci
dent
rep
ortin
g sy
stem
s
Nar
rativ
e an
alys
is
Ove
rall,
med
icat
ion
inci
dent
s w
ere
mos
t fre
quen
tly r
epor
ted.
Tot
al e
rror
ra
te w
as m
uch
high
er in
stu
dies
usi
ng
volu
ntar
y re
port
ing
than
in a
stu
dy
usin
g m
anda
tory
rep
ortin
g. M
ulti-
inst
itutio
nal r
epor
ting
iden
tifie
d ra
re
but i
mpo
rtan
t err
ors.
A s
ubst
antia
l nu
mbe
r of i
ncid
ents
wer
e po
tent
ially
ha
rmfu
l. W
hen
a sy
stem
app
roac
h w
as u
sed,
man
y co
ntrib
utin
g fa
ctor
s w
ere
iden
tifie
d. In
form
atio
n ab
out t
he
impa
ct o
f sys
tem
cha
nges
on
patie
nt
safe
ty w
as s
carc
e
Mul
ti-in
stitu
tiona
l, vo
lunt
ary,
no
n-pu
nitiv
e, s
yste
m-b
ased
in
cide
nt r
epor
ting
is li
kely
to
gene
rate
val
uabl
e in
form
atio
n on
type
, aet
iolo
gy, o
utco
me
and
prev
enta
bilit
y of
inci
dent
s in
the
neon
atal
ICU
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
56
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
57
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Stu
mp,
20
00
US
A
ITS
Hos
pita
l car
e
N =
1 h
ospi
tal
Per
iod
= F
irst q
uart
er 1
997
– se
cond
qua
rter
of 2
00
0 (in
terv
entio
n st
arte
d in
199
7 an
d co
mpl
eted
in J
une
1999
)
Aim
To r
edes
ign
the
med
icat
ion
erro
r rep
ortin
g pr
oces
s
Inte
rven
tio
nA
ser
ies
of in
terv
entio
ns w
as
impl
emen
ted
to o
ptim
ise
med
ical
err
or r
epor
ting.
C
ompa
red
with
the
hist
oric
al
repo
rtin
g pr
oces
s, th
e ne
w
proc
ess
incl
uded
:•
non
-pun
itive
rep
ortin
g•
cen
tral
pha
rmac
y de
part
men
t rec
eivi
ng
repo
rt w
ithin
48
hour
s ra
ther
than
2–
3 m
onth
s•
a u
nifie
d da
taba
se in
stea
d of
a fr
agm
ente
d pr
oces
s•
nea
r mis
ses
capt
ured
in
eve
ry s
tage
of
med
icat
ion-
use
proc
ess
and
not o
nly
in d
ispe
nsin
g pr
oces
s•
str
uctu
red
chec
k-bo
x re
port
s in
stea
d of
ha
ndw
ritte
n fr
ee te
xt•
sta
ff a
t ope
ratio
nal l
evel
in
volv
ed in
rev
iew
ing
data
Co
ntr
ol
NA
Num
ber o
f rep
orte
d ev
ents
Sta
tistic
al m
etho
dolo
gy is
unc
lear
Incr
ease
in n
umbe
r of r
epor
ted
even
ts
from
app
roxi
mat
ely
45 to
276
per
qu
arte
r with
in o
ne y
ear o
f the
sta
rt o
f th
e im
plem
enta
tion
Alte
rnat
ive
med
ical
err
or
repo
rtin
g pr
oces
s in
crea
ses
the
num
ber o
f rep
orte
d in
cide
nts

Dückers et al
Safety and risk management in hospitals
56
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
57
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Tid
eiks
aar,
1993
US
A
RC
T
Ger
iatr
ic h
ospi
tal u
nit
N =
70
patie
nts
(35
inte
rven
tion
+ 35
con
trol
)
Per
iod
= 9
mon
ths
Aim
To e
xam
ine
the
clin
ical
ef
ficac
y of
a b
ed a
larm
sy
stem
in r
educ
ing
falls
from
be
d on
a g
eria
tric
eva
luat
ion
and
trea
tmen
t uni
t
Inte
rven
tio
nB
ed a
larm
sys
tem
dur
ing
hosp
ital s
tay
Co
ntr
ol
Usu
al c
are,
with
out b
ed a
larm
1. N
umbe
r of p
atie
nts
sust
aini
ng fa
ll fr
om
bed
2. N
umbe
r of p
atie
nts
sust
aini
ng o
ther
fa
lls
1. N
o st
atis
tical
diff
eren
ce in
falls
from
be
d be
twee
n th
e ex
perim
enta
l (N
= 1
) and
con
trol
(N
= 4
) gro
up
(p =
1.0
0)
2. C
linic
al tr
end
tow
ards
red
uced
falls
in
the
expe
rimen
tal g
roup
The
dat
a su
gges
t tha
t bed
al
arm
sys
tem
s ar
e be
nefic
ial i
n gu
ardi
ng a
gain
st b
ed fa
lls a
nd
are
an a
ccep
tabl
e m
etho
d of
pr
even
ting
falls
Voe
ffra
y, 2
00
6
Sw
itzer
land
ITS
Che
mot
hera
py u
nit o
f the
ph
arm
acy
serv
ice
with
in a
ho
spita
l
N =
940
pre
scrip
tions
(pr
e-
inte
rven
tion)
N =
978
pre
scrip
tions
(po
st-
inte
rven
tion)
Per
iod
= 36
mon
ths
(15
mon
ths
pre
-inte
rven
tion,
21
mon
ths
post
-inte
rven
tion)
Aim
Red
ucin
g th
e nu
mbe
r of
pre
scrip
tion
erro
rs b
y im
plem
entin
g a
CP
OE
sys
tem
Inte
rven
tio
nC
PO
E, s
uch
that
a
pres
crip
tion
by a
juni
or d
octo
r is
firs
t val
idat
ed b
y a
seni
or
doct
or o
nlin
e be
fore
bei
ng
proc
esse
d. A
fter
val
idat
ion
the
orde
r is
auto
mat
ical
ly
tran
sfer
red
to n
ursi
ng s
taff
an
d ph
arm
acy
serv
ices
. A
ny c
orre
ctio
n on
initi
al
pres
crip
tion
is tr
ansm
itted
to
all p
rofe
ssio
nals
invo
lved
Co
ntr
ol
NA
Pre
scrip
tion
erro
r rat
e (p
er 1
00
pres
crip
tion
prot
ocol
s)
Bin
omia
l tes
t
1. S
igni
fican
t red
uced
err
or r
ate
(15%
be
fore
ver
sus
5% a
fter
)2.
Ave
rage
err
or r
ate
with
han
dwrit
ten
pres
crip
tions
gre
ater
than
with
co
mpu
teris
ed p
resc
riptio
ns (1
3.1%
ve
rsus
0.6
%)
3. N
umbe
r of e
rror
s re
duce
d dr
amat
ical
ly w
hen
50%
of p
roto
cols
w
ere
pres
crib
ed th
roug
h C
PO
E
Err
ors
alm
ost d
isap
pear
ed a
fter
im
plem
enta
tion
of C
PO
E
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
58
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
59
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Wal
sh, 2
008
US
A
ITS
Pae
diat
ric s
ervi
ce in
a
gene
ral h
ospi
tal
N =
627
adm
issi
ons
Per
iod
= S
epte
mbe
r 20
01 –
May
20
02 (
pre
-in
terv
entio
n), A
pril
2002
–
June
20
02 (
impl
emen
tatio
n)
Sep
tem
ber 2
002
– M
ay
2003
(po
st-in
terv
entio
n)
Aim
To e
valu
ate
the
effe
ct o
f C
PO
E o
n th
e ra
te o
f inp
atie
nt
paed
iatr
ic m
edic
atio
n er
rors
Inte
rven
tio
nU
se o
f a c
omm
erci
al
CP
OE
sys
tem
. Aft
er o
rder
en
try,
the
syst
em u
ses
a w
eigh
t-ba
sed
dosa
ge
calc
ulat
or to
aut
omat
ical
ly
chec
k m
edic
atio
n do
sage
, ge
nera
ting
wro
ng d
osag
e al
erts
. Oth
er fe
atur
es in
clud
e dr
ug–
drug
inte
ract
ion
aler
ts
and
alle
rgy
aler
ts. A
ll C
PO
E
user
s at
tend
ed a
two
-hou
r tr
aini
ng s
essi
on
Pre
-CP
OE
situ
atio
n: n
ursi
ng
med
icat
ion
reco
rds
wer
e pa
per b
ased
, and
onl
y th
e ho
spita
l pha
rmac
y w
as
auto
mat
ed w
ith a
sys
tem
to
chec
k dr
ug–
drug
inte
ract
ion
and
alle
rgie
s
Co
ntr
ol
NA
1. O
vera
ll m
edic
atio
n er
ror r
ate
2. S
erio
us m
edic
atio
n er
ror r
ate
3. N
on-in
terc
epte
d se
rious
inte
ract
ions
4. P
reve
ntab
le A
DE
s5.
Rat
e of
dos
ing
erro
rs6.
Rat
e of
ad
min
istr
atio
n er
rors
Tim
e se
ries
anal
ysis
(P
roc
Aut
oreg
) an
d un
ivar
iate
ana
lysi
s
1. N
o ch
ange
(44
.7 e
rror
s/1,
00
0 pa
tient
day
s [b
efor
e] v
ersu
s 50
.9
erro
rs [a
fter
], IR
R =
1.1
4 [9
5% C
I =
0.80
–1.5
1])
2. N
o ch
ange
(31
.7 e
rror
s/1,
00
0 pa
tient
day
s [b
efor
e] v
ersu
s 33
.0
erro
rs [a
fter
], IR
R =
1.0
4 [9
5% C
I =
0.70
–1.5
4])
3. N
o ch
ange
(23
.1 e
rror
s/1,
00
0 pa
tient
day
s [b
efor
e] v
ersu
s 20
.6
erro
rs [a
fter
], IR
R =
0.8
9 [9
5% C
I =
0.69
–1.7
8])
. Tim
e se
ries
anal
ysis
sh
owed
a s
tatis
tical
ly s
igni
fican
t dr
op (
7%, p
= 0
.049
5).
4. N
o ch
ange
(7.
9 er
rors
/1,0
00
patie
nt d
ays
[bef
ore
] ver
sus
6.5
erro
rs [a
fter
], IR
R =
0.8
3 [9
5% C
I =
0.37
–1.8
74])
5. N
o ch
ange
(8
erro
rs/1
,00
0 pa
tient
day
s [b
efor
e] v
ersu
s 11
er
rors
/1,0
00
patie
nt d
ays
[aft
er];
p
= N
C)
6. N
o ch
ange
(6
erro
rs/1
,00
0 pa
tient
da
ys [b
efor
e] v
ersu
s 4
erro
rs/1
,00
0 pa
tient
day
s [a
fter
]; p
= N
C)
CP
OE
in p
aedi
atric
inpa
tient
ca
re is
not
eff
ectiv
e in
red
ucin
g m
edic
atio
n er
rors

Dückers et al
Safety and risk management in hospitals
58
Appendix E: Included studies, sorted by alphabetical order
Dückers et al
Safety and risk management in hospitals
59
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Will
iam
s, 2
007
Aus
tral
ia
UB
A
Med
ical
war
ds o
f 1 h
ospi
tal
N =
1,3
57 p
atie
nt
adm
issi
ons
Per
iod
= D
ecem
ber 2
002
–
May
20
04 (
Dec
embe
r 20
02 –
May
20
03 p
re-
inte
rven
tion,
Dec
embe
r 20
03 –
May
20
04 p
ost-
inte
rven
tion)
Aim
To e
valu
ate
a sy
stem
atic
, co
-ord
inat
ed a
ppro
ach
to
limit
the
seve
rity
of fa
lls a
nd
min
imis
e th
eir n
umbe
r in
an
acut
e ca
re h
ospi
tal
Inte
rven
tio
nP
atie
nts
wer
e cl
assi
fied
base
d on
thre
e le
vels
of
risk:
low
, med
ium
, hig
h.
App
ropr
iate
inte
rven
tions
(e
nviro
nmen
t, m
obili
ty,
elim
inat
ion)
wer
e de
velo
ped
for e
ach
risk
leve
l in
an
indi
vidu
al fa
ll ca
re p
lan
Co
ntr
ol
NA
1. N
umbe
r of f
alls
per
1,
00
0 O
BD
2. S
ever
ity o
f fal
ls
The
Man
n-W
hitn
ey U
-tes
t and
S
tude
nt’s
t-te
st
1. S
igni
fican
t red
uctio
n in
falls
(9
.5/1
,00
0 O
BD
[bef
ore
] ver
sus
8.0
/1,0
00
OB
D [a
fter
] [95
% C
I of
the
diff
eren
ce =
-0.
14–
-0
.16
], p
< 0
.001
)2.
No
chan
ge in
sev
erity
of f
alls
App
roac
h w
as e
ffec
tive
in
redu
cing
fall
inci
denc
e
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.

Dückers et al
Safety and risk management in hospitals
60
Appendix E: Included studies, sorted by alphabetical order
Fir
st a
uth
or,
ye
ar, c
ou
ntr
yS
tud
y d
esig
nIn
terv
enti
on
Ou
tco
me
mea
sure
sA
nal
ysis
an
d r
esu
lts
Ove
rall
con
clu
sio
n
Wol
ff, 2
002
Aus
tral
ia
UB
A
ED
N =
2,5
75 (
pre
-inte
rven
tion)
N =
2,3
71, 2
,461
, 2,3
92,
2,66
4, 2
,720
, 2,3
73 a
nd
2,49
4 (p
ost-
inte
rven
tion)
Per
iod
= O
ctob
er –
D
ecem
ber 1
997
(pre
-in
terv
entio
n), J
anua
ry 1
998
– S
epte
mbe
r 199
9 (p
ost-
inte
rven
tion)
Aim
To d
eter
min
e if
retr
ospe
ctiv
e m
edic
al r
ecor
d sc
reen
ing
and
clin
ical
rev
iew
follo
wed
by
app
ropr
iate
act
ion
can
effe
ctiv
ely
dete
ct a
nd r
educ
e A
Es
in a
n E
D
Inte
rven
tio
nR
etro
spec
tive
scre
enin
g of
pa
tient
file
s in
two
phas
es:
by c
ompu
ter w
ith 5
gen
eral
pa
tient
out
com
e cr
iteria
; ‘p
ositi
ve’ f
iles
by h
and
by
nurs
e. E
D d
irect
or s
cree
ned
AE
s. T
hen,
pre
vent
ive
actio
n w
as ta
ken:
• c
hang
es in
hos
pita
l po
licie
s•
foc
used
aud
iting
• s
taff
dis
cuss
ion
• g
uide
line
impl
emen
tatio
n•
wee
kly/
quar
terly
rep
orts
• p
rom
otio
n of
clin
ical
-in
cide
nt r
epor
ting
Co
ntr
ol
NA
Num
ber o
f ED
at
tend
ance
s as
soci
ated
with
an
AE
Chi
squ
are
test
Sig
nific
ant d
ecre
ase
from
84
(3.2
6%)
in fi
rst q
uart
er to
12
(0.4
8%) i
n la
st
quar
ter (
RR
red
uctio
n =
85.3
% [9
5%
CI =
62.
7%–1
00
%],
p <
0.0
001
)
AE
s in
ED
s ca
n be
eff
icie
ntly
de
tect
ed a
nd th
eir r
ate
redu
ced
usin
g re
tros
pect
ive
med
ical
re
cord
scr
eeni
ng to
geth
er w
ith
clin
ical
rev
iew
, ana
lysi
s an
d ac
tion
to p
reve
nt r
ecur
renc
es
AD
E =
adv
erse
dru
g ev
ent;
AE
= a
dver
se e
vent
; AN
CO
VA
= a
naly
sis
of c
ovar
ianc
e; A
NO
VA
= a
naly
sis
of v
aria
nce;
C =
con
trol
gro
up; C
DS
S =
clin
ical
dec
isio
n su
ppor
t sys
tem
; CI =
con
fiden
ce in
terv
al;
CP
OE
= c
ompu
teris
ed p
hysi
cian
ord
er e
ntry
; CM
I = c
ontin
uous
med
icat
ion
infu
sion
; CO
= c
ompa
nion
obs
erve
rs; E
D =
em
erge
ncy
depa
rtm
ent;
I = in
terv
entio
n gr
oup;
ICU
= in
tens
ive
care
uni
t;
IQR
= in
ter
quar
tile
rang
e; IT
S =
inte
rrup
ted
time
serie
s; L
OS
= le
ngth
of s
tay;
MD
W =
med
icat
ion
disc
harg
e sh
eet;
ME
T =
med
ical
em
erge
ncy
team
; N =
num
ber;
NA
= n
ot a
pplic
able
; NC
= n
ot c
lear
; N
SA
ID =
non
-ste
roid
al a
nti-i
nfla
mm
ator
y dr
ug; O
BD
= o
ccup
ied
bed
day;
OR
= o
dds
ratio
; PD
A =
per
sona
l dig
ital a
ssis
tant
; QI =
qua
lity
impr
ovem
ent;
RC
T =
ran
dom
ised
con
trol
led
tria
l; R
R =
rel
ativ
e ris
k;
SD
= s
tand
ard
devi
atio
n; U
BA
= u
ncon
trol
led
befo
re-a
fter.
Top Related