







Languages
Pages
Legal


Royal Free Hospital, London
Endoscopic Endoscopic Surgery:Surgery:
Risk Management Risk Management and Medico-Legal and Medico-Legal
issuesissues

Royal Free Hospital, London
Laparoscopic complicationsLaparoscopic complications
1. Complications are less common than with laparotomy, but when they do occur, they are potentially more serious.
2. Patients assume “key hole” surgery is “minor surgery” and so should not be associated with “major complications”.

Royal Free Hospital, London
Possible laparoscopic Possible laparoscopic complicationscomplications
Injury to:
Major blood vessels
Anterior abdominal wall vessels
Large bowel
Small bowel
Bladder
Ureter
Liver
Stomach
Spleen
Subcutaneous emphysema
Pneumothorax
Pneumomediastinum
Gas embolism
Hypercarbia
Post-operative shoulder pain
Persistence of pneumoperitoneum
Cardiac arrhythmia
Cardiac arrest
Nerve injury (e.g. brachial plexus injury)

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London
Medico-legal cases involving Medico-legal cases involving operative laparoscopy I have operative laparoscopy I have
given an opinion on:given an opinion on:Injury to external iliac artery
Injury to common iliac
vessels
Injury to pelvic side-wall
vessels
Injury to aorta
Cardiac arrest
Post-operative bleeding
Injury to sigmoid colon
Injury to ascending colon
Injury to transverse colon
Injury to small bowel
Injury to bladder
Injury to ilio-inguinal nerve

Royal Free Hospital, London
Risk managementRisk management
1. Identify risk2. Analyse risk
- Publications- Incident reporting- Complaints- Medico-legal claims
3. Modify practice to prevent, control or minimize risk in future

Royal Free Hospital, London
What factors increase the risk What factors increase the risk of laparoscopic complications?of laparoscopic complications?
1. Complex surgery
2. Older patient
3. Extremes of weight
4. Previous abdominal surgery/adhesions
5. Poor surgical technique/inexperience
6. Faulty/incorrect equipment

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London
What factors increase the risk What factors increase the risk of laparoscopic complications?of laparoscopic complications?
1. Complex surgery
2. Older patient
3. Extremes of weight
4. Previous abdominal surgery/adhesions
5. Poor surgical technique/inexperience
6. Faulty/incorrect equipment

Royal Free Hospital, London

Royal Free Hospital, London
What factors increase the risk What factors increase the risk of laparoscopic complications?of laparoscopic complications?
1. Complex surgery
2. Older patient
3. Extremes of weight
4. Previous abdominal surgery/adhesions
5. Poor surgical technique/inexperience
6. Faulty/incorrect equipment

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London
What factors increase the risk What factors increase the risk of laparoscopic complications?of laparoscopic complications?
1. Complex surgery
2. Older patient
3. Extremes of weight
4. Previous abdominal surgery/adhesions
5. Poor surgical technique/inexperience
6. Faulty/incorrect equipment

Royal Free Hospital, London

Royal Free Hospital, London
What factors increase the risk What factors increase the risk of laparoscopic complications?of laparoscopic complications?
1. Complex surgery
2. Older patient
3. Extremes of weight
4. Previous abdominal surgery/adhesions
5. Poor surgical technique/inexperience
6. Faulty/incorrect equipment

Royal Free Hospital, London

Royal Free Hospital, London
Laparoscopic procedure
No. of procedures to
reach proficiency
CholecystectomyFundoplicationColectomyHerniorrhaphySplenectomy
20 (8 to 200)28 (20 to 60)40 (13 to 70)30 (20 to 50)20 (16 to 20)

Royal Free Hospital, London
Experienced surgeon Trainee surgeon

Royal Free Hospital, London

Royal Free Hospital, London
What factors increase the risk What factors increase the risk of laparoscopic complications?of laparoscopic complications?
1. Complex surgery
2. Older patient
3. Extremes of weight
4. Previous abdominal surgery/adhesions
5. Poor surgical technique/inexperience
6. Faulty/incorrect equipment

Royal Free Hospital, London
Endoscopy cart for Endoscopy cart for laparoscopylaparoscopy
Light source
Electrosurgicalgenerator
High flow insufflator Video monitors
Suction/irrigation unit
Electronic morcellatorCamera unit

Royal Free Hospital, London
How to reduce laparoscopic complicationsHow to reduce laparoscopic complications
1. Complications related to laparoscopic entry
2. Complications related to the operative procedure
3. Complications related to pneumoperitoneum
4. Complications related to patient position
5. Complications related to anaesthesia

Royal Free Hospital, London
How to reduce laparoscopic complicationsHow to reduce laparoscopic complications
1. Complications related to laparoscopic entry
2. Complications related to the operative procedure
3. Complications related to pneumoperitoneum
4. Complications related to patient position
5. Complications related to anaesthesia

Royal Free Hospital, London
How to reduce How to reduce complications complications
related to related to laparoscopic laparoscopic
entryentry

Royal Free Hospital, London
Summary data for major laparoscopic Summary data for major laparoscopic complicationscomplications
Overall complication rate Intestinal Vascular Urinary tract
7-12.6 per 10001.6 to 2.4 per 10000.3 per 10002 to 8.5 per 1000
Complication during setup phase 1:3
Conversion to laparotomy 2%
Complication not recognised 1:4
Mortality rate 4.4 per 100,000
Mortality after hysterectomy for benign indications
150 per 100,000

Royal Free Hospital, London

Royal Free Hospital, London
Remember, bowel injury during Remember, bowel injury during abdominal entry also occurs with abdominal entry also occurs with
conventional surgeryconventional surgery

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London
Alternative entry techniquesAlternative entry techniques
Optical Veress needle
Microlaparoscopy
Optical trocar
Safety-shield
ENDOTIP cannula
Step Radial Expanding System
Palmer’s point

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London
Subumbilical insufflation and insertion of primary Subumbilical insufflation and insertion of primary trocar and cannulatrocar and cannula
1. Palpate for aorta2. Elevate anterior abdominal wall (to increase distance
between needle and bowel/major vessels)3. Aim Veress needle and trocar and cannula towards the
hollow of the sacrum (away from major vessels)4. Create a high pressure pneumoperitoneum prior to inserting
umbilical trocar and cannula (to increase distance between needle and bowel/major vessels)
5. Insert trocar and cannula no more than a few centimetres into the peritoneal cavity (to reduce risk of bowel or vascular injury
6. Avoid Trendelenburg tilt (head down) until laparoscope has been inserted (to avoid bringing major vessels closer to umbilicus)
7. Avoid excessive force during insertion (to limit the distance the instruments advance into the peritoneal cavity.

Royal Free Hospital, London
Palpation for aortic bifurcationPalpation for aortic bifurcation

Royal Free Hospital, London
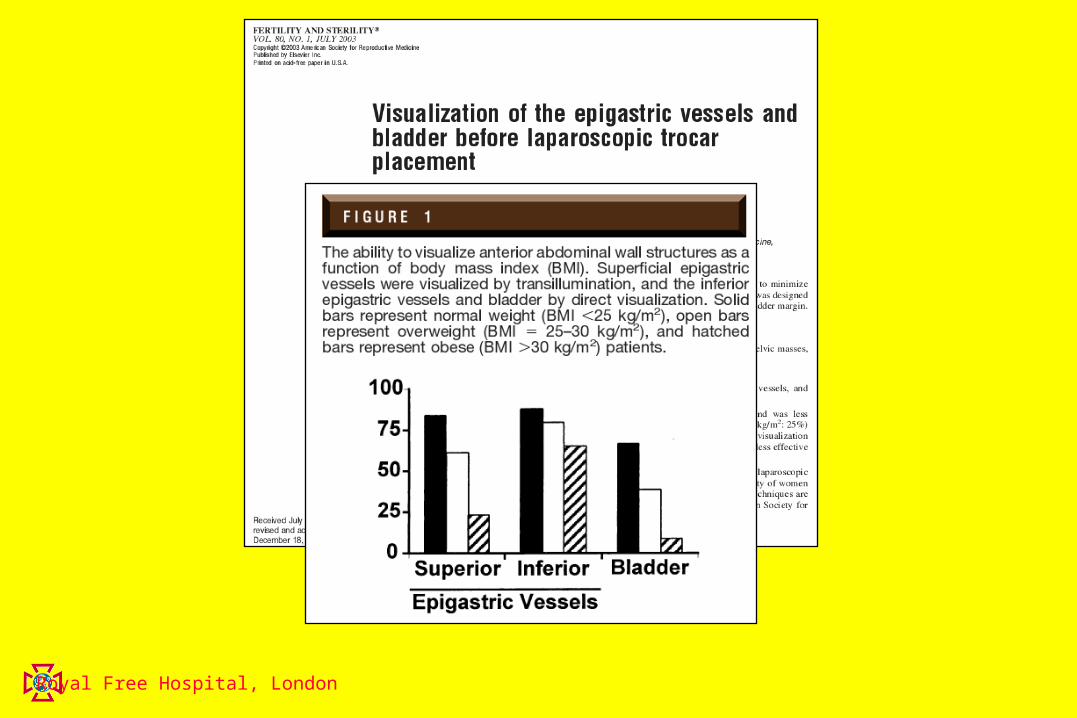
Body mass index Body mass index

Royal Free Hospital, London
Body mass index Body mass index

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London
Midclavicular linebelow costal margin
Palmer’s point: laparoscopic entry site in “high Palmer’s point: laparoscopic entry site in “high risk” casesrisk” cases
Use in cases ofPrevious laparotomyPrevious peritonitisLarge pelvic mass
Inflammatory bowel disease

Royal Free Hospital, London

Royal Free Hospital, London
Vessels of the lower anterior Vessels of the lower anterior abdominal wallabdominal wall

Royal Free Hospital, London
Insert ancillary ports under Insert ancillary ports under direct visiondirect vision

Royal Free Hospital, London
The inferior epigastric vessels are always outside to The inferior epigastric vessels are always outside to the safe trianglethe safe triangle

Royal Free Hospital, London
The inferior epigastric vessels are always outside to The inferior epigastric vessels are always outside to the safe trianglethe safe triangle
X
Royal Free Hospital, London

Royal Free Hospital, London
How to reduce How to reduce complications complications related to the related to the laparoscopic laparoscopic procedureprocedure

Royal Free Hospital, London
Causes of laparoscopic Causes of laparoscopic operative injuriesoperative injuries
Cutting (eg. scissors, laser, monopolar
electrosurgery)
Burning (eg. electrosurgery, laser)
Tearing (eg. blunt dissection)
Ligating (eg. sutures, clips, staples)

Royal Free Hospital, London
Safe laparoscopic surgerySafe laparoscopic surgery
Ensure structures are well visualisedDo not tear tissue by applying too
much force when probing or retractingBe careful during during sharp
dissection (eg. division of adhesions)Be very careful using thermal energy
(eg. electrosurgery, laser) near bowel, ureter and other vital structures.

Royal Free Hospital, London

Royal Free Hospital, London
Some complications are not Some complications are not recognisedrecognised
Overall complication rate Intestinal Vascular Urinary tract
7-12.6 per 10001.6 to 2.4 per 10000.3 per 10002 to 8.5 per 1000
Complication during setup phase 1:3
Conversion to laparotomy 2%
Complication not recognised 1:4
Mortality rate 4.4 per 100,000
Mortality after hysterectomy for benign indications
150 per 100,000
Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London
GMC guidance: GMC guidance: Making and Making and Using Visual and Audio Using Visual and Audio Recordings of Patients Recordings of Patients

Royal Free Hospital, London
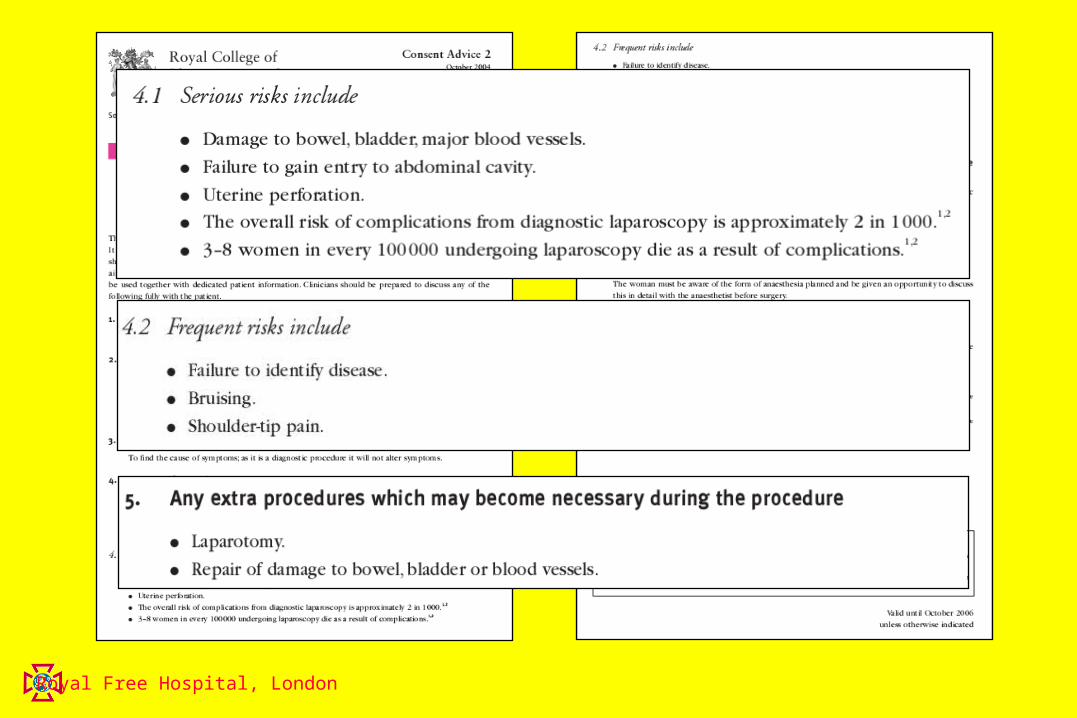
Informed Informed consentconsent

Royal Free Hospital, London
Laparoscopic complicationsLaparoscopic complications
1. Complications are less common than with laparotomy, but when they do occur, they are potentially more serious.
2. Patients assume “key hole” surgery is “minor surgery” and so should not be associated with “major complications”.

Royal Free Hospital, London
Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London

Royal Free Hospital, London
Electrosurgical generatorElectrosurgical generator
Monopolar circuit
Blend
Bipolar circuit
Cutting Coagulation

Royal Free Hospital, London
Electrosurgical generatorElectrosurgical generator
Monopolar circuit
Blend
Bipolar circuit
Cutting Coagulation
Increasingvoltage

Royal Free Hospital, London
Management of laparoscopic Management of laparoscopic vascular injuryvascular injury
Minor oozing Inspect under low pressure
Moderate intraperitoneal bleeding
Control with electrosurgery, suturing or clips
Major intraperitoneal bleeding
Immediate laparotomy, pressure and call surgeons
Retroperitoneal bleeding Observe haematoma and laparotomy if enlarging

Royal Free Hospital, London
Management of laparoscopic Management of laparoscopic vascular injuryvascular injury
Minor oozing Inspect under low pressure
Moderate intraperitoneal bleeding
Control with electrosurgery, suturing or clips
Major intraperitoneal bleeding
Immediate laparotomy, pressure and call surgeons
Retroperitoneal bleeding Observe haematoma and laparotomy if enlarging

Royal Free Hospital, London
Management of laparoscopic Management of laparoscopic bowel injurybowel injury
Sharp, partial thickness Laparoscopic suture
Full thickness, small volume contamination
Laparoscopic suture, check for leakage
Full thickness, large volume contamination
LAPAROTOMY
Small bipolar injury Laparoscopic suture
Large bipolar injury LAPAROTOMY
Monopolar injury LAPAROTOMY

Royal Free Hospital, London
Management of laparoscopic Management of laparoscopic bowel injurybowel injury
Sharp, partial thickness Laparoscopic suture
Full thickness, small volume contamination
Laparoscopic suture, check for leakage
Full thickness, large volume contamination
LAPAROTOMY
Small bipolar injury Laparoscopic suture
Large bipolar injury LAPAROTOMY
Monopolar injury LAPAROTOMY

Royal Free Hospital, London
Management of laparoscopic urinary Management of laparoscopic urinary tract injurytract injury
Bladder perforation < 2 cm
Prolonged bladder drainage
Bladder perforation > 2 cm
Surgical repair (by laparoscopy or laparotomy)
Ureteric transection Surgical repair (by laparoscopy or laparotomy)
Ureteric ligation Remove suture

Royal Free Hospital, London
Management of laparoscopic urinary Management of laparoscopic urinary tract injurytract injury
Bladder perforation < 2 cm
Prolonged bladder drainage
Bladder perforation > 2 cm
Surgical repair (by laparoscopy or laparotomy)
Ureteric transection Surgical repair (by laparoscopy or laparotomy)
Ureteric ligation Remove suture
Top Related