






Languages
Pages
Legal


1
Last Revision 12/20/17 nlf
Risk Management (RM) Program Reporting and Revised Forms
In order for KDHE- Health Facilities Program to better assist facilities with their Risk Management
Programs, Health Facilities Risk Management Reporting is converting to an electronic system/E-files. RM forms
and the RM reporting processes have been revised to maintain a consistent and user-friendly system of E-files and
RM reporting for all.
A major feature working toward consistency is our new centralized Risk Management email mailbox. You may
submit all of your Individual Incident Reports (IIR), Quarterly Reports (QR), RM Plans and any RM inquiries
electronically to [email protected].
Use the KDHE RM mailbox (listed above) for all of your RM submissions.
Private
Secure
Encrypted
Dedicated
Shared by RM Team at KDHE
*Just remember your Who/ What/ When in the Subject Line!
**And your CCN/ State ID # in the document.

2
Last Revision 12/20/17 nlf
Naming Convention Requirements for All Risk Management Communications:
When utilizing communication activities to include the new centralized RM mailbox-- you must complete the
Subject Line with the following 4 Naming Conventions:
Who: Name of Institution
What is the action: Individual Incident Report (IIR); Quarterly Report (QR); Inquiry; RM Plan
Date: Date incident occurred or Date RM Plan submitted to KDHE
In addition- the CNN # or State ID#: (If your facility is not Certified, Include your State ID#) is required
to be on every document when submitted. This includes the IIR, QR, RM Plan, and/or Inquiry.
Note- Clarification regarding the various reporting dates:
Date of the Incident is the Static Date. (This is different than the date sent to KDHE)
Always use this date as your reference date, especially when referring to IIR’s. An example is
(Horton_IIR 4-2-17) (Who/ What/ When)
And then include in document your CCN/ State ID#
Example: Risk Management Mailbox: [email protected].
Naming Convention: Subject line: ABC Company Inc._RM QR1,_3-24-17.
ABC Company Inc._IIR Q3, 4-12-17.
ABC Company Inc._2018 RM Plan 1-15-18
ABC Company Inc. _Inquiry 5-5-17
All facilities should begin using the new system and forms from this point forward.
Note- All reports submitted on or after January 1, 2018 that are not completed on the new forms and are not
following the “Subject Line” protocol of Who, What and When and/or CCN/ State ID#-------------------will be
returned as unprocessable.
The revised forms along with training tools, samples and examples are to assist your facility in building a strong
and successful Risk Management Program can be found on the KDHE website at
http://www.kdheks.gov/bhfr/state_ach_licensure_forms.html.
Scroll down under “Risk Management” to locate various revised forms and sample tools.

3
Last Revision 12/20/17 nlf
Health Facilities would like to thank you for participating every year in the “Survey Monkey”.
Your response provides us with valuable information towards building strong Risk Management Programs.
You can look forward to future Survey Monkeys and training coming your way.
LaDonna Lee
Sr. Administrative Assistant/RM Coordinator
KDHE/BCHS/Health Facilities Program
1000 SW Jackson St., Suite 330
Topeka, KS. 66612-1365
785-296-1249
Fax: (785) 785-559-4250
Nelleda L. Faria, RN, BSN, MBA, PMP, CPHRM
Health Facility Surveyor- Risk Manager/ OASIS Education Coordinator
KDHE/BCHS/Health Facilities Program
1000 SW Jackson St., Suite 330
Topeka, KS. 66612-1365
Ph: 785-296-4714
Fax: 785-559-4250

4
Last Revision 12/20/17 nlf
PAGE LEFT INTENTIONALLY BLANK

5
Last Revision 12/20/17 nlf
TABLE OF CONTENTS
Topic Page #
Introduction to Risk Management Program
Page 1
Individual Incident Reporting (IIR) Instructions
Page 6
Individual Incident Reporting (IIR) Cover Page
Page 9
Individual Incident Reporting (IIR) Form
Page 10
Quarterly Reporting (QR) Instructions
Page 12
Quarterly Reporting (QR) Cover Page
Page 14
Quarterly Reporting (QR) Form
Page 15

6
Last Revision 12/20/17 nlf
Instructions on How to Complete the
Individual Incident Report (IIR)
**Cover Page Must Be Completed and Returned With the Report**
Every finalized SOC III and/or IV incident that occurs within the medical care facility must be reported to KDHE
on the IIR form upon determination of the final SOC. KDHE is the licensing body or agency over your facility or
institution.
Please note that any IIR a Risk Manager (RM) deems necessary can be submitted to KDHE.
All IIRs should be sent to KDHE upon determination of the SOC(s).
Please mark any applicable referral that you make to an individual’s licensing board or agency, if applicable with
the incident.
Cover Page
Please complete the name and address listed on the facility license. Do not use initials.
Be sure to enter the CNN#. This is the # assigned by CMS when your facility became certified. It always starts with 17_ _
_ _
Note: *CCN is CMS Certification Number: If your facility is not CMS Certified, please list State ID#
Type of facility: If you are a general hospital with a psychiatric unit, check “Hospital.” only.
Facility Address Information
Risk Manager Name and Title with contact information.
Risk Manager Attestation Signature and Date
Regarding patients: Always remember to redact patient name(s), dates of birth, social security numbers, and other
individually identifiable information from the report submitted to KDHE.
Regarding staff: Always remember to redact staff names(s), dates of birth, licensure numbers and other individually
identifiable information from the report submitted to KDHE.

7
Last Revision 12/20/17 nlf
Instructions on How to Complete the
Individual Incident Report (IIR)
IIR Report Form
1. Facts of the Incident section is where the detailed description of what happened is put. This section answers the
Who, What, When, Where, Why and How (5W1H).
2. Standard of Care (SOC) Determination and Assignment- Please list the various owners and the associated SOC
assigned for each.
3. Describe the corrective actions taken to remediate the incident or prevent occurrence/ re-occurrence:
4. Select the corrective action category taken to remediate the incident or prevent occurrence/ re-occurrence:
5. Complete findings from Root Cause Analysis (RCA) for failure/ Specify recommendations for Minimizing Future Occurrences from the system failure or identified cause.
6. Indicate the category type of incident/occurrence
7. Mark on the IIR form which licensing agency(ies) the referral was sent to.
8. Submit your IIR to the E-file address listed below.
9. Please remember to submit any Risk Management correspondence using the revised Naming Convention
Policy of otherwise your documentation will be returned.
Who
What
When (use the Date of the Incident as your date)
CCN#
Example: ABC Inc. QR2 7-25-16
Kansas Department of Health and Environment
Bureau of Community Health Systems
Risk Management Program
1000 SW Jackson Street, Suite 330
Topeka, Kansas 66612-1368
8
Last Revision 12/20/17 nlf
Email to [email protected]
Or Fax to (785) 559-4250
Retain the original of the IRR forms and attach it with the Quarterly Report (QR) summary for each
applicable reporting quarter.
All SOC III and IV IIR reports are submitted as soon as the final SOC determinations are made.
If there is a concern regarding an Incident that is egregious, potential for headlines, or other high profile
or unique situation that may need discussion or recommendations--- please call the KDHE Risk Manager.

9
Last Revision 12/20/17 nlf
Confidential Cover Page
RISK MANAGEMENT INDIVIDUAL INCIDENT REPORT (IIR) FORM
Risk Management SOC 3 AND 4
28-52-2. Incident reporting. (a) Each medical care facility shall identify a written form on which employees and
health care providers shall report clinical care concerns to the risk manager, chief of staff, or administrator. The
original or complete copy of the incident report shall be sent directly to the risk manager, chief of staff, or
administrator, as authorized in the facility's risk management plan. (b) The risk manager, chief of staff, or
administrator shall acknowledge the receipt of each incident report in writing. This acknowledgment may be made
in the following manner: (1) file stamping each report; (2) maintaining a chronological risk management reporting
log; (3) signing or initialing each report in a consistent fashion; Or (4) entering pertinent information into a
computer database. (c) Incident reports, investigational tools, minutes of risk management committees, and other
documentation of clinical analysis for each reported incident shall be maintained by the facility for not less than
one year following completion of the investigation. (Authorized by and implementing K.S.A. 65-4922; effective
Feb. 27, 1998.)
Name of Facility *CCN# 17-_________
Facility Type: Hospital [ ] Psychiatric Hospital [ ] Ambulatory Surgical Center [ ] Other [ ]____________
Address City ___________________________
Name and Title of Risk Manager_________________________________________________________
Email address ________________________________________________________________________
Phone Number Date: _____________________________ *CCN is CMS Certification Number: If your facility is not CMS Certified, please list State ID#
With this submission, as the above listed Risk Manager I hereby attest that the report submitted to Kansas Department of Health and Environment is true, complete and accurate to the best of my knowledge without known errors or omissions.
Signature ___________________________Date___________________

10
Last Revision 12/20/17 nlf
INDIVIDUAL REPORTABLE INCIDENT REPORT FORM
SOC 3 / 4 RISK MANAGEMENT
Date of the Incident:_______________ Date Incident Reported to RM:__________________
1. Facts of the Incident (Detailed description to include who, what, where, when, why, and how ): (Please attach
additional sheets as needed)
2. Standard of Care (SOC) Determination and Assignment:
3. Specify corrective actions taken to remediate the incident or prevent occurrence/ re-occurrence:

11
PRIVACY & CONFIDENTIALITY NOTICE: This communication as part of Risk Management is protected information and non-discloseable
or discoverable. This is including any attachments, may contain confidential information and is intended only for the individual or entity to which
it is addressed as part of the Risk Management Program. Any review, dissemination, or copying of this communication by anyone other than the
intended recipient is strictly prohibited.
INDIVIDUAL REPORTABLE INCIDENT REPORT FORM
SOC 3 / 4 RISK MANAGEMENT
4. Indicate the corrective action taken such as □ Policy / Procedure Change □ Suspension of Privileges
□Termination □ Counseling / Education □ Restriction of Privileges □ Revocation of Privileges □ Pending
□ Other: __________________________________
5. Root Cause Analysis (RCA) for failure/ Specify recommendations for Minimizing Future Occurrences:
6. Indicate the category type of incident/occurrence such as:
□ Fall □ Abuse, Neglect or Exploitation □ Assessment/treatment □ Professional licensure event □
Delay □ Facility process or system-related □ Scope of Practice □ Impairment due to drug, alcohol or
cognition □ Falsification □ Documentation of Narcotics □ Medication Error □ Improper Procedure □
EMTALA-Related □ IV line mix-up □ Drug Diversion □ Unprofessional conduct □ IV infiltration
□ Other: __________________________________
7. All reports are submitted to KDHE as the licensing agency. In addition, please indicate any referral
reports sent to following additional licensing agencies. There is no need to attach evidence of referral.
Board of Healing Arts Board of Nursing Board of
Pharmacy Other

12
PRIVACY & CONFIDENTIALITY NOTICE: This communication as part of Risk Management is protected information and non-discloseable
or discoverable. This is including any attachments, may contain confidential information and is intended only for the individual or entity to which
it is addressed as part of the Risk Management Program. Any review, dissemination, or copying of this communication by anyone other than the
intended recipient is strictly prohibited.
Instructions on How to Complete the Risk Management Quarterly Report
(QR)
**Cover Page Must Be Completed and Returned With the Report**
Please complete the name and address listed on the facility license. Do not use initials.
Be sure to enter the CNN#. This is the # assigned by CMS when your facility became certified. It always starts with
17_ _ _ _ If your facility is not CMS Certified, please list the Facility State ID#__________.
All reportable incidents must be reported to KDHE on the IIR form upon determination of the final numbers.
All quarterly reports should be sent to KDHE within 30 days of the end of the report quarter.
The due dates are April 30th
, July 31st
, October 31st
and January 31st
10. Type of facility: If you are a general hospital with a psychiatric unit, check “Hospital.” only.
Year: Make sure you document the year and the quarter that is listed.
First quarter = January, February and March
Second quarter = April, May and June
Third quarter = July, August and September
Fourth quarter = October, November and December
11. If you have an IIR that has occurred during your current Quarterly Reporting quarter but you are waiting
on a determination from your facility Advisory Board---
a. Check the box indicating this on the QR form and submit another REVISED QR for said quarter
when you receive the determination.
b. When submitting the REVISED QR to KDHE be sure and check the appropriate box. Also include
any IIR and referral hashes, when appropriate.
12. Total number of final SOC determinations by the facility’s risk management program this quarter:
Reporting of SOC III and IV determinations are mandated but you may report anything at any time.
13. Specify the individual number of referrals sent to each of the individual licensing agencies. If you select
“Other” please provide explanation.
14. Identify the appropriate category type of each individual incident (IIR). If you select “Other” please
explain.
15. Submit your QR to the E-file address listed below. Please remember to submit any Risk Management
correspondence using the revised Naming Convention Policy of otherwise your documentation will be

13
PRIVACY & CONFIDENTIALITY NOTICE: This communication as part of Risk Management is protected information and non-discloseable
or discoverable. This is including any attachments, may contain confidential information and is intended only for the individual or entity to which
it is addressed as part of the Risk Management Program. Any review, dissemination, or copying of this communication by anyone other than the
intended recipient is strictly prohibited.
returned.
Who
CCN#
What
Date submitted to KDHE
Example: ABC Inc. QR2 7-25-16
Kansas Department of Health and Environment
Bureau of Community Health Systems
Risk Management Program
1000 SW Jackson Street, Suite 330
Topeka, Kansas 66612-1368
Email to [email protected]
Or Fax to (785) 559-4250

14
PRIVACY & CONFIDENTIALITY NOTICE: This communication as part of Risk Management is protected information and non-discloseable
or discoverable. This is including any attachments, may contain confidential information and is intended only for the individual or entity to which
it is addressed as part of the Risk Management Program. Any review, dissemination, or copying of this communication by anyone other than the
intended recipient is strictly prohibited.
Confidential Cover Page
Quarterly Report (QR) Pursuant to KSA 65-4923(d)
(d) Each review and executive committee referred to in subsection (a) shall submit to the secretary of health and environment, on a
form promulgated by such agency, at least once every three months, a report summarizing the reports received pursuant to
subsections (a)(2) and (a)(3) of this section. The report shall include the number of reportable incidents reported, whether an
investigation was conducted and any action taken.
Reporting Year ___________ Reporting Quarter ____________
Check this box if this is an amendment to a previous QR report submitted. What Quarter? _____
Check this box if you have an IIR occurred but not reported this QR because waiting on decision from Advisory
Board as to the determination and you will be submitting KDHE and amended QR after determination.
Name of Facility *CCN# 17-_________
Address City ________________
Name and Title of Risk Manager
Email address ________________________________________________________________________
Phone Number Date Sent to KDHE: ____________
*CCN is CMS Certification Number: If your facility is not CMS Certified, please list State ID#
With this submission, as the above listed Risk Manager I hereby attest that the report submitted to Kansas Department of Health and Environment is true, complete and accurate to the best of my knowledge without known errors or omissions.
Signature Date______________________
15
PRIVACY & CONFIDENTIALITY NOTICE: This communication as part of Risk Management is protected information and non-discloseable
or discoverable. This is including any attachments, may contain confidential information and is intended only for the individual or entity to which
it is addressed as part of the Risk Management Program. Any review, dissemination, or copying of this communication by anyone other than the
intended recipient is strictly prohibited.
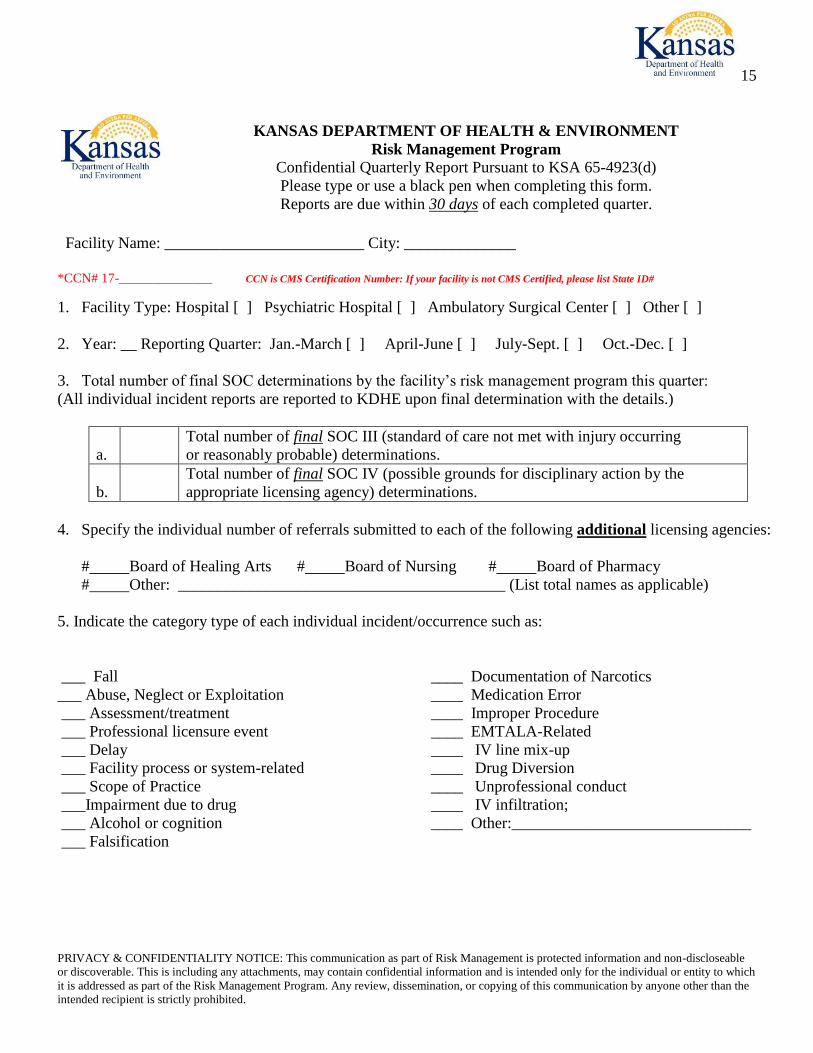
KANSAS DEPARTMENT OF HEALTH & ENVIRONMENT
Risk Management Program
Confidential Quarterly Report Pursuant to KSA 65-4923(d)
Please type or use a black pen when completing this form.
Reports are due within 30 days of each completed quarter.
Facility Name: _________________________ City: ______________
*CCN# 17-______________ CCN is CMS Certification Number: If your facility is not CMS Certified, please list State ID#
1. Facility Type: Hospital [ ] Psychiatric Hospital [ ] Ambulatory Surgical Center [ ] Other [ ]
2. Year: __ Reporting Quarter: Jan.-March [ ] April-June [ ] July-Sept. [ ] Oct.-Dec. [ ]
3. Total number of final SOC determinations by the facility’s risk management program this quarter:
(All individual incident reports are reported to KDHE upon final determination with the details.)
a.
Total number of final SOC III (standard of care not met with injury occurring
or reasonably probable) determinations.
b.
Total number of final SOC IV (possible grounds for disciplinary action by the
appropriate licensing agency) determinations.
4. Specify the individual number of referrals submitted to each of the following additional licensing agencies:
# Board of Healing Arts # Board of Nursing # Board of Pharmacy
# Other: _________________________________________ (List total names as applicable)
5. Indicate the category type of each individual incident/occurrence such as:
___ Fall
___ Abuse, Neglect or Exploitation
___ Assessment/treatment
___ Professional licensure event
___ Delay
___ Facility process or system-related
___ Scope of Practice
___Impairment due to drug
___ Alcohol or cognition
___ Falsification
____ Documentation of Narcotics
____ Medication Error
____ Improper Procedure
____ EMTALA-Related
____ IV line mix-up
____ Drug Diversion
____ Unprofessional conduct
____ IV infiltration;
____ Other:______________________________

PRIVACY & CONFIDENTIALITY NOTICE: This communication as part of Risk Management is protected information and
non-discloseable or discoverable. This is including any attachments, may contain confidential information and is intended only
for the individual or entity to which it is addressed as part of the Risk Management Program. Any review, dissemination, or
copying of this communication by anyone other than the intended recipient is strictly prohibited.
Nelleda L. Faria, RN, BSN, MBA, PMP, CPHRM
Health Facility Surveyor- Risk Manager/ OASIS Education Coordinator
KDHE/BCHS/Health Facilities Program
1000 SW Jackson St., Suite 330
Topeka, KS. 66612-1365
Ph: 785-296-4714
Fax: 785-559-4250
Return this report to:
LaDonna Lee
Sr. Administrative Assistant/RM Coordinator
KDHE/BCHS/Health Facilities Program
1000 SW Jackson St., Suite 330
Topeka, KS. 66612-1365
785-296-1249
E-mail report to [email protected]
Fax: (785) 785-559-4250
Data Collection Purpose: The purpose of the data collection activity is solely for usage as business analytics for the KDHE Risk
Management Program. This includes but is not limited to overall Risk Management Program business intelligence, enterprise
information management, enterprise performance management, analytic applications, and governance, risk, and compliance.
Top Related