





Languages
Pages
Legal


..... , ::IL ELSEVIER
Journal of Vestibular Research, Vol. 8, No. I, pp. 27-34,1998 Copyright © 1998 Elsevier Science Inc. Printed in the USA. All rights reserved
0957-4271/98 $19.00 + .00
Pll S0957 -4271(97)00034-7
Review
CLINICAL EVIDENCE THAT THE VESTIBULAR SYSTEM PARTICIPATES IN AUTONOMIC CONTROL
Joseph M. Furman,* Rolf G. Jacob,t and Mark S. Redfern:j:
I !
Del'e:rtmeAts ef *OteIElf)'A~ele~y, 1'PsyeRiatf), Otel~AEI-$9telatyA!;J6IemMlA6-lflal:lStfieI~iAeeriA~, ~I University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania
Reprint address: Joseph M. Furman, MD, PhD, The Eye & Ear Institute Building, 200 Lothrop Street, Suite 500, Pittsburgh, PA 15213. Tel: (412) 647-2117; Fax: (412) 647-2080; E-mail: [email protected]
both the peripheral vestibular system, that is, the labyrinth, and the central vestibular system, is known to influence autonomic function in several ways that have clinical implications. This paper discusses evidence for vestibular influences on autonomic control from normal human subjects, evidence for vestibular influences on autonomic control from patients, clinical implications of vestibuloautonomic regulation, and speculations regarding possible clinical implications of vestibulo-autonomic control. Situations that provoke vestibularinduced autonomic responses in normal subjects include vestibular laboratory testing, vehicular motion, simulators, and, possibly, exposure to microgravity. Patients with peripheral and central vestibular abnormalities manifest both symptoms and signs of autonomic dysfunction presumably via vestibulo-autonomic connections. Vestibuloautonomic regulation impacts vestibular diagnosB@ Iesnng, ciimcai dIagnosIs of BaJance msoroers, anci treatment of haianci: disorders. In addition to \\ eI ;'recognizcL periphent: anel ccntra! vestihular disorders. anxie!~ disorcier,; iJ2 V l rcct'ntl~ becn linked tn vcstibu iar dysrunctior: ir , subse: 0' ;1 ... -
tients. In particular. vestihular d~'sfunction has been linked to panic disorder and agoraphobia. Vestibular-autonomic connections may form a basis for an association between vestihular dysfunction and panic attacks. The importance of vestibulo-autonomic regulation in the clinical arena is not fully known. Two speculative areas discussed in this paper include vestibular-induced orthostatic intolerance and the role of vestibular-respiratory pathways on sleep apnea. © 1998 Elsevier Science Inc.
27
balance; orthostatic intolerance; phobia.
Introduction
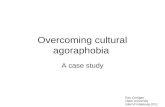
The vestibular system, including both the peripheral vestibular system, that is, the labyrinth, and the central vestibular system, is known to influence autonomic function in several ways that have clinical implications. Figure I illustrates diagrammatically how input from the vestibular labyrinth and other sensory systems combine in the vestibular nuclei to influence socalled vegetative symptoms such as nausea, vomiting, and changes in heart rate and blood pressure. Additionally, sensory signals important PSS spA'. nb".lioR, .8H~ tlu .. hi 1
nuclei. also influence the locus coeruleus. a noradrenerf'ic qfucture though t to be important ir panic c1 i ~ ()"Je' and agorull!1c1bia (J) . AnOlile: i---:~I I ··:~l·Y. ~:··~L·t L:j"~ fG" \'·?s : !~u i:.~ · · ~rJt 'l :10 n: i:'
regulation i~ the cerebellum. which i!-> known to influenct the cardio\'a~cular system (2 .) .
This paper is concerned with the clinical il11-plication!-> of vestibular autonomic regulation and will be organized as follows. There will be a discussion of evidence for vestibular influences on autonomic control from normal human subjects, evidence for vestibular influences on autonomic control from patients, clinical implications of vestibulo-autonomic regulation and,

28
Affective and
Vestibular Nuclei
J. M. Furman et al
Respiratory Canters
Figure 1. An overview of vestibular influences on autonomic control. Ascending projections from the vestibular nuclei to the parabrachial nucleus may participate In producing affective and emotional responses, and dysfunction in this pathway may lead to psychiatric disorders such as agoraphobia. A descending pathway from the vestibular nuclei to bralnstem centers that control respiration and circulation may be responsible for adjusting blood pressure and respiration during movement and changes in posture.
finally, speculations regarding possible clinical implications of vestibulo-autonomic control.
Evidence for Vestibular Influences on Autonomic Control from Normal
HdiIISII 5d6]@(G
The vestibular system is known to influence the sympathetic nervous system, the parasym-pat e IC nervous sys ern, an e respir 0
system. Although the respiratory system is not formally part of the autonomic nervous system, the involuntary nature of respiratory control and its importance in vomiting prompted its inclusion herein. Evidence for vestibular influences on autonomic control from normal human subjects includes the occurrence of both autonomic "symptoms," that is, perception on the part of subjects, and "signs," that is, objective findings that can be observed. Vestibular-induced auto-
nomic symptoms include nausea, malaise, drowsiness, abdominal awareness, anxiety, distress, dread, and reduced vigilance. Vestibular-induced autonomic signs include changes in salivation, changes in gastric motility, vomiting, endocrine responses, "cold" sweating, pallor, increased blOOd hOw to §k@1@M hld§Ei@§, Mid CIIMIg8§ hi heart rate and heart rate variability.
Situations that provoke vestibular-induced autonomic responses include clinical vestibular a ora 0 eng, re
tory testing, vehicular motion, simulators. and exposure to microgravity. The latter three circumstances can lead to motion sickness, simulator sickness, and space sickness, respectively. The term "sickness" refers to the autonomic signs and symptoms that result from a combination of vestibular stimulation, visual motion, and visual-vestibular interaction. Vestibular-induced motion sickness has been conceptualized as a "poison response" that includes a combination

-
Clinical Evidence for Autonomic Control
of "stomach emptying" and a "stress response" (3). Stomach emptying includes a combination of symptoms of the act of vomiting, argininevasopressin (A VP) release, and increased activity in the parasympathetic nervous system. The "stress response" includes symptoms of anxiety or discomfort, endocrine release. and predominantly sympathetic nervous system changes.
There are several issues regarding vestibularinduced autonomic changes that are unresolved.
x'fhese mell!6e-iflEW/iQy&:l1!&ri~aipn&bi"'UCSptibility to vestibular-induced autonomic changes, the relative influence of the semicircular canals compared with the otolith organs. and the cause
Evidence for Vestibular Influences on Autonomic Control from Patients
Evidence for vestibular influences on autonomic control from patients includes the effects of acute unilateral peripheral vestibular loss, vestibular compensation for unilateral peripheral loss, and the effects of central vestibular lesions on autonomic control including lesions both of the brainstem and of the cerebellum. Acutely, unilateral peripheral vestibular disease causes vegetative symptoms such as nausea. vomiting, and malaise. These symptoms and signs are unquestionably related to direct and indirect connection~ from the vestibula .. system [(, til::- autonomIC nervow, system (..j.). ~k' usefuJnes\ n' these symptoms and sign~ physiologlcall) i~ uncertain, \"itll the pr, )..:es~ of"\ estibular compensmion" (:'i L which re'lIlt~ in ,I re~()luti(Jn
of vestibulo-ocular and ve~tibulo-spinal imbalances. patients typically have a resolution of their vegetative symptoms ane! signs. In partiClllar, vomiting typically resolves over a period of hours. Nausea and malaise may be more longstanding and can continue for days to weeks, even in patients who eventually fully recover their functional abilities.
Many patients with central nervous system disorders that adversely affect central vestibular structures have accompanying autonomic symptoms and signs tll':\ ,n:1\' hI' "dated to the disc'"
29
der primarily, or may be related to the effect of the disorder on central vestibular function. Such disorders as brainstem or cerebellar infarction (6), migraine (7,8), the effects of neurotoxins (9), and neurodegenerative disorders (10), all can affect central vestibular function and/or autonomic function . For example. the highly prev-alent nausea and occasional vomiting that ac-companies migraine headache (11) may be due, in part, to abnormalities in vestibulo-autonomic
f.
cOllIlectioDs duriDg J! migrainous ep=is=o""d""e""" -=S~iIru=' ----..... 11--larly, the autonomic symptoms and signs asso-ciated with lateral medullary infarction (Wal-lenberg's syndrome) may be a result of direct
Clinical Implications of Vestibulo-Autonomic Regulation
Diagnostic Testing of the Vestibular System
Current diagnostic testing methods used in the evaluation of vestibular disorders include caloric testing, rotational testing, and platform posturography. A limitation of each of these methods pertains to autonomic symptoms induced' by vestibular stimulation. For caloric testing. in our experience, nausea is induced in most patients and vomiting occurs in about 5% of patients, l\utonomic symptom" require disC(\l1linuatio; of caloric te:.;tiJ1~ prior to complt tiOI, of hinaural hithcrma: tcstiJ1f in aOl)ut )(,( of (lUi' pal i~nt.-,. Com cnuoJ1a! i'(ltaU,)na icqing,
\\'herei" patien;s are genli:- Sfll!I' wh ~ lc s~ated ir a compUler-C(lIllroJlec, (nUlL ;'areJ~ re:--Ull, ill
autonomic ~ymrtoms thai are severe enough to warrant discontinuation of testing, Another lype of rotational testing. still in the development stage. is designed to assess the otolith-ocular reflex and uses off-vertical axis rotation. For this test, patients are tilted while rotating. Offvertical axis rotation leads to significant autonomic symptoms that ultimately may limit the clinical applicability of this new technique (12). Measures to reduce autonomic symptoms in_'luclc assuring that the ambient temperature in

30
the test ella! 'I ~ r is below 65°F • .llllllhat total test time is strictly limited. Dynamic posturography rarely induces significant autonomic symptoms. However, future refinements of and additions to platform posturography, including assessment of visually induced sway (13), may lead to significant autonomic symptoms.
Balance Disorders and AnxieTY Symptoms
Manv vestibular Jisorders .1fe associated with aU[ol1omic sympt(1!:1S and ~ign~. For '=XLlI11!':e. ')eripheral vcslibuiar disorders. ~uch as .\r!e:llere·:, Jisease. are often associatet.! with nausea ant.! vomiting in addition [0 vertigo . .-\s :-toted above. presumably, the nausea and vomiting are a result of the influence of peripheral vestibular signals on the autonomic nervous system. Also, as noted above, central vestibular disorders can lead to abnormal autonomic nervous system activity.
In addition to well-recognized peripheral and central vestibular disorders, certain anxiety disorders recently have been linked to vestibular dysfunction in a subset of patients (14,15). In particular, vestibular dysfunction has been linked to panic disorder and agoraphobia (16-21). Panic attacks are characterized by sudden onset of autonomic symptoms, hyperventilation, and dizziness. The autonomic symptoms include heart palpitations, sweating, trembling, hot or cold flashes, and gastrointestinal distress; the symptoms of hyperventilation include shortness of breath, feeling like choking, chest discom-
J. M. Furman et al
malities (22). Based upon the symptol"" 01 patients with anxiety, many are likely to be suffering from alterations in vestibulo-autonomic regulation. This idea is supported by the knowledge that patients with bonafide panic attacks have autonomic symptoms as an accompaniment of their attacks.
Patients with panic disorder often develop agoraphobia. characterized by avoidance of situations such as heights. elevators. supermar-
. ket~ . .;hopping malls . ..:ro\vds. theaters. ~tacliLLl11s. rraveiing. bridges. and [unnels (24). The high iJrevaknce !)r' 'eslibui:.u~ dy,,!'unction in ')anic disllrder .. vith igorapilnbia .-uggesls a func' Jonal
. relationship be[ween these ..:onditions. The [)fesenc~ of such a relationship :~ also supported by findings that panic attacks and agoraphobic avoidance are prevalent among otoneurological patients with balance complaints and objectively demonstrated vestibular dysfunction. Eagger and colleagues (25) found that one third of patients with peripheral vestibular disorders had panic and agoraphobic symptoms. Similarly, Stein and colleagues (26) found a prevalence of panic disorder of 41 % in patients with vestibular disorders; Clark and colleagues (14) found panic attacks in 37% of patients with vestibular disorders as compared to a 0% prevalence of panic in patients with mild hearing loss.
Current theories of the epidemiology of panic disorder include (1) dysregulation of brainstem noradrenergic systems (for example 27-29); (2) involvement of central serotonergic pathways (30); and (3) respiratory dysfunction (31,32).
~ - • ~. • ~~ - . - _.... _ ... . . • • • • • •• ". II _ . • • ~ • . _. ... .. " _.. '." ..... _ , . ..
III I .' I • ....1 .. •• .1 ..1 • • • •• I. • •• .: •• •• •• I.':'
disorders is uncertain, possibly, It IS medIated panic disorder and vestIbular dysfunctIOn. Relaby autonomic circuits involving the locus co- tionships between the vestibular system and emleas, a sffilet1:1fe that inFffienee:esHallfm~Oll!s*t-Ee""'1'eef'1ry,..! --ls*mAI:l:lEe~tel:1lFFt!elSS--Eo*f-liIflB,ateM'Fe:esS4~;-jftee~F-'ffl*laBIfIHIM:e~8i:lE' BIeOIFlFa~e~F~llf' BlEefHhlM:l:a:lEe~-"".I---part of the brainstem and spinal cord (1). (1) connections between the locus coeruleus ~
A commonly used diagnostic term for pa- and the lateral vestibular nucleus, as well as altients with dizziness and anxiety without con- terations in vestibular processing after iontocomitant symptoms that clearly define a vestib- phoretic administration of clonidine to the locus ular syndrome such as Meniere's disease or coeruleus (33-36); (2) vestibular input to the migraine is "psychogenic dizziness" (22). Ned- raphe nuclei (37-39) as well as serotonergic efzelski and colleagues (23) have proffered a defi- fects on vestibular processing (40,41); and (3) nition for psychogenic dizziness. Their definition vestibular-respiratory connections (42-44). Also, is problematic because many patients labeled as the nucleus parabrachialis receives vestibular psychogenic may have vestibular system abnor- and visceral input and is connected with struc-

Clinical Evidence for Autonomic Control
tures of the limbic system, including the amygdala (45). The amygdala and other parts of the limbic system are known to be essential for the conditioning of fear responses (46).
Although these neuroanatomical findings suggest a relationship between vestibular dysfunction and panic attacks, they may not easily account for the observations. within patients with panic disorder, of a specific relationship betHleep vestibular Oysfupctip9 2nd ?scxapilgGiQ avoidance. However, "pseudo-agoraphobic" syndromes in patient with vestibular disorders have long been recognized. including "street neurosis"
(50), "space phobia" (51.52) , and "visual vertigo" (53). In larger samples, the most common fears reported by patients with balance disorders include heights (1 4,25 ,54) and boats (1 4). In fact, it has been suggested that the psychiatric condition of height phobia is related to vestibular dysfunction (55).
"Space and motion discomfort" (56) represents a unifying theme among the situations enumerated above. The concept of SMD is based on the notion that, in many patients with chronic, perhaps partially compensated, vestibular dysfunction, vestibular symptoms are situation-specific. This situational specificity, in turn. is related to a sensory integration strategy in which visual and proprioceptive information is used to replace the defective information in the vestibular channel. Individuals utilizing thi ~ strategy would be expectcG to be particu larl) sensitive to (a ) inadequ at ~· 0 ; l11 i!-. leadin.g vi sual information (J :'.57 , 0; " tc' in sLal1il lt \ 0:' the ,>uppor: ... urface (SS.S LI I.
SM! may be a con~eq ucnce of increased dependenc:c on nOI1\ e~ tibLl l ar spatia; informati on combined wi th II1appropriate sell:.ory integration. The situation~ thal trigger SMD are characterized by inadequate or non vestibular spatial cues and include heights. boats, crowds, and the "particularly rich or repetitive visual patterns" (53) occuning in supermarkets, and certain floor, wallpaper, or traffic patterns. We believe that in patients with panic disorder, SMD can contribute to the development of agoraphobic avoidance. This theory is supported by our findings I! ..• , I) patients with anxiety disorders selected
31
for prominent SMD showed an increased postural sensitivity to optic flow stimuli (57), and (2) agoraphobics, known to have high levels of SMD (56), exhibited a surface-dependent sway pattern on computerized dynamic posturography (59).
To summarize, central vestibulo-autonomic relationships, along with the situational specificity of vestibular symptoms leading to SMD, pi9"i98 M:l6 easis fur the role o()f the 'Vestibul1lf'----I.--system in certain anxiety disorders. Specifically, vestibular-autonomic connections may form a basis for association with panic attacks. Also,
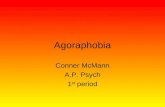
terns is facilitated, including agoraphobia. Figure 2 (I) summarizes these relationships, imbedded with other possibilities not specifically discussed here. For example, increased arousal and the behavior of hyperventilation, both common in panic disorder, may affect vestibular function (60-62).
The model depicted in Figure 2 (1) is still incomplete. Importantly, we need to further develop our understanding of why vestibular dysfunction contributes to anxiety disorders in some individuals and not in others. The nature of the underlying vestibulopathy (that is, whether acute or chronic, compensated or uncompensated) and the degree of anxiety proneness (as indicated, for example, by a family history of anxiety dis-orders) are likely moderators of the relation-ship . Even though vestibular dysfunction may no; be the ultimate caLl ~e 0; panic disorder. it appear\ \() contribute to it ~ phenomenoiog:. par-[iculari ~ the dcwiopmeni of agoraollOblu.
Trearl11ent qf Pariellls 'with Balance Disorders
Treatment for vestibular disorders currently includes pharmacotherapy, physical therapy, and surgery. An emerging technology that may be applied to the treatment of patients with dizziness and balance disorders is that of virtual environments (63). Autonomic side effects from physical therapy can be a limiting factor in treatment options. Similarly, as virtual envim ':ments evolve as an additional treatmellt modality, au-
i,

32 J. M. Furman et al ._--------------------------------
I Other Visceral Input I I ,
Vestibular Dysfunction Autonomic Activity
I t I Hyperventilation I ,
Space / Motion "-
I Panic Disorder I ) I
I Discomfort I
~ J~ Other Agoraphobic
/ \ I I Mechanisms ~
, r
Agoraphobia without Panic
?anlc Disoroer I with Agoraphobia fooo, ~t---------------'
Figure 2. Overview of relationships between vestibular dysfunction and certain anxiety disorders. From Jacob and colleagues (1).
tonomic side effects also are likely to be a limiting factor, as with physical therapy, since exposure to virtual environments in nonnal subjects is well known to cause autonomic symptoms (64). Such symptoms may be immediate, delayed, and/or prolonged. Possibly, with improved understanding of vestibulo-autonomic regulation, the side effects of physical therapy or from virtual environments can be minimized. Also, physical therapy techniques typically used for patients with vestibular disorders may become useful for a subset of patients with anxiety disorders, particularly those anxious patients with objectifi-
Further Speculations Regarding Clinical Implications
The importance of vestibulo-autonomic regulation in the clinical arena is as yet unknown. Two . peculative areas of application include vestibular-induced orthostatic intolerance and the role of vestibular-respiratory pathways on sleep apnea. Although these issues are only being explored in a very preliminary fashion, orthostatic intolerance experienced by astronauts returning to Earth (65) may have as a
component abnormal vestibulo-autonomic regulation. Further research regarding vestibuloautonomic connection, particularly otolith-autonomic influences, may improve our understanding of "Earth sickness." Also, although patients with vestibular disorders rarely complain of orthostatic hypotension, they avoid making sudden changes in posture that would require rapid readjustments in circulation.
Upper airway muscle tone is known to be influenced by head position (43,66-68). Such influences may be mediated by vestibulo-respiratory circuits. Possibly, by altering the activity in
ameliorated by vestibular stimulation.
Conclusions
In conclusion, vestibulo-autonomic pathways impact the field of vestibular and balance disorders. In particular, patients with either peripheral and central vestibular abnonnalities manifest both symptoms and signs of autonomic dysfunction. Vestibular autonomic regulation affects the assessment, diagnosis, and treatment of patients with vestibular disorders.

Clinical Evidence for Autonomic Control 33
REFERENCES
1. Jacob RG, Funnan 1M, Perel 1M. Panic, phobia, and vestibular dysfunction. In: Yates Bl, Miller AD, editors. Vestibular autonomic regulation. Boca Raton (FL): CRC Press; 1996. p 197-228.
" Balaban C. The role of the cerebellum in vestibular autonomic function. In: Yates BJ. Miller AD. editors. Vestibular autonomic regulation. Boca Raton (FL): CRC Press; 1996. pI27-46.
3. Money K, Lackner 1, Cheung R. The autonomic nervous system and motion sickness. In: Yates BJ, Miller o P '1;5055 ¥'spb"'er pHlepeTic rcwJ1etjP2 Roca Raton (FL): CRC Press, 1996. pI47-74.
4. Yates BJ, Miller AD. Overview of vestibular autonomic regulation. In: Yate~ Bl. Miller AD. editors. Vestibular autonomic regulation. Boca Raton (FL): CRC Press:
compensation). Brain Res Rev 1991;16:117-33. 6. Adams RD, Victor M. Principles of neurology (4th ed.).
New York: McGraw-Hill Information Services Company; 1989.
7. Harker LA. Migraine-associated vertigo. In: Baloh RW, Halmagyi GM, editors. Disorders of the vestibular system. New York: Oxford University Press ; 1996. p407-17.
8. Cass SP. Funnan JM, Ankerstjerne 1. Balaban C, Yetiser S, Aydogan B. Migraine-related vestibulopathy. Ann Otol Rhinol LaryngoI1997;106:181-9.
9. Hodgson MJ, Funnan JM, Ryan C, Durrant ID, Kern E. Encephalopathy and vestibulopathy following a shorttenn hydrocarbon exposure. J Occup Med 1989;31(1): 51-4.
10. Gilman S, Bloedel JR, Lechtenberg R. Disorders of the cerebellum. Contemporary neurology series. Philadelphia: FA Davis Company; 1981.
II. Davidoff RA. Migraine: Manifestations, pathogenesis, and management. Philadelphia: FA Davis: 1995.
12. Furman 1M, Schor R. Schumann T. Off-vertical axis rotation: a test of the otolith-ocular-reflex. Ann Otol Rhinol Laryngol 1992; I 0](8):643-50.
13. Redfern MS. Funnan JM. Postural sway ot' patient, with vestibular disorders during optic flow . J Ve,tih Res 1994:4(3)::;~ I-:Hl.
14. Clark DB. Hirsch BE. Smith MG Furman.lM JalOb RG. Panic 111 ntolaryngClI(!!;\ pall':Ill" presel1l1n!; WHI, dlzzine:-- or hearing los!--. An .I ['''y-:hiall I 1Il).j:l:iI' 1223-5
15 . .Iacob I<G . Furman .Iil'i. Gal<ln<lll .:[.; 1--\ ,11J.lln. aspect~ of ve:--tibular di:--orliers. In: Balol · R\\ . Halmagyi Gl'vl. editor:--. Handl)(lol, ' (If neurotolog~'I\' estihu
lar system. Ne\\ Yorl.: Oxiord Univer~ll~ Pres:, IYlitJ pI97-1::!7.
16. Jacob RG. Moller MB. Turner SM. Wall CW Ill. Otoneurological examination of panic disorder and agoraphobia with panic attacks: a pilot study. Am J Psychiatr 1985; 142:715-20.
17. SkJare DA, Stein MB. Pikus AM, Uhde TW. Disequilibrium and audiovestibular function in panic disorder: symptom profiles and test finding. Am J Otol 1990; 11:338-41.
18. Hoffman DL. O'Leary DP, Munjack Dl. Autorotation test abnonnalities of the horizontal and vertical vestibulo-ocll' .' i,:f1exes in panic disorder. Otolaryngol Head Neck SUlg I Y9 \. ' : rJ:25 ~-69.
19. Yardley L, Luxon L, Lear S, Britton 1, Bird 1. Vestibular and posturographic test results in people with symptoms of panic and agoraphobia. J Audiol Med 1994: 3:48-65.
20. Yardley L. Britton J. Lear S. Bird J. Luxon L. Relationship between balance system function and agoraphobic avoidance. Behav Res Ther 1995:33:435-9.
21. lacob RG. Funnan 1M, Durrant lD, Turner SM. Panic. agoraphobia and vestibular dysfunction: clinical test results. Am 1 Psychiatr 1996;153:503-12.
22 BUTleR 1M 'acob BO PSYShjapjr djzzjness Nynep! 1997;48(5): 1161-6.
23. Nedzelski 1M. Barber HO. McIlmoyl L. Diagnoses in a dizziness unit. J Otolaryngol 1986:15: 101-4.
24. Jacob RG. Panic disorder and the vestibular system. Clin of North Am 1:361-74.
ular disorder: a clinical and neuro-otological study. J Neurol Neurosurg Psych 1993:55:383-7.
26. Stein MB. Gordon JG, Asmundson GJF. Ireland D, Walker JR. Panic disorder in patients attending a clinic for vestibular disorders. Am J Psychiatr 1994; 151 : 1697-700.
27. Charney DS , Heninger GR, latlow PI. Increased anxiogenic effects of caffeine in panic disorders. Arch Gen Psychol 1985;42:233-43.
28. Charney DS, Heninger GR. a2-adrenergic and opiate receptor blockade: synergistic effects on anxiety in healthy subjects. Arch Gen Psychiatr 1986;43: 1037-41.
29. Asnis GM, van Praag HM. The norepinephrine system in panic disorder. In: Asnis GM, van Praag HM, editors. Panic disorder: clinical, biological, and treatment ~ aspects. New York: John Wiley & Sons; 1995. pI 19-50.
30. Kahn RS, Westenberg HGM, Moore C. Increased serotonin function and panic disorder. In: Asnis GM, van Praag HM, editors. Panic disorder: clinical, biological and treatment aspects. New York: John Wiley & Sons; 1995. pI51-80.
31. Klein DF. False suffocation alarms. spontaneous panics, and related conditions. Arch Gen Psychiatr 1993; 50:306-17.
31. Papp U· .. Klein DF. Gorman Ji\'i Carhon diOXide hyper:--elhitivit~ . hyperventilation. and p,mic disorder. ·,111 J PS~:':lliatl 199:: l:i( ': 114"-:i-
:;., S~hllerge' R.i. Balaban CD. Tile dl<.tl'lhuliOI n n(lrdUrell': rg 1(.' dAon, am; _~I I b ,die: 11th. \ ~qinliia IlIl-'ic
. ~) o~·r~I:;ni~ . ., l .. d·,.,i; ... .:~ J. -: -.S::':'" ,- I' .. - .. - .: " .'_ S~huerger RJ. Balahan CD. Immunohlsw;:- henll(;al
dc:mollstration of regiOn,dl~ SekCtl\'L' project' 11'<1111 lo<.:u' coerulcus to the vest ihulm nuc lei 111 rat:--. Exp Brain Re~ 19<).1:<)2:351-9.
35. Schuerger RJ. Balaban CD. Noradrenergic projection:-to the vestibular nuclei (VN) in monkey labstract]. Soc Neuroscience Abstr 1993:19: 136.
36. Schuerger RJ, Schor RH, Balaban CD. Alpha-2 adrenergic drug injections in the vestibular nuclei modify modulation of electromyographic responses to off-vertical axis rotation stimulation in decerebrate rats. 1996 Midwinter Research Meeting of the Association for Research in Otolaryngology, Vol. 20, Abstract #80.
37. Yates BJ, Goto T, Bolton PS. Responses of neurons in the caudal medullary raphe nuclei of the cat to stimulation of the vestibular ne!";\!. i:xp Brall Res 1992;89: 323-32.

c _~ ,
34
38. Yates Bl, Goto T, Kerman L, Bolton PS. Responses of caudal medullary raphe neurons to natural vestibular stimulation. 1 Neurophysiol 1993;70:938--46.
39. Licata F, LiVolsi G, Maugeri G, Santagelo F. Effects of 5-hydroxytryptamine on the firing rates of neurons of the lateral vestibular nucleus in the rat. Exp Brain Res 1990;79:293.
-10. Steinbusch HWM. Distribution of serotonin-immunoreactivity in the central nervous system of the rat cell bodies and terminals. Neurosci 1981 :6:557-618.
-II. Licata F. liVolsi G. Maug.:ri G. Ciranna L. Santangelu F. Serotonln-e\,okell mollifications 01' ih.: neuronal firing rate in the: sup':riur '!estibular lIucku~: a I1llC ro ionlOpilllretic , tllliy in Ihe rat. Neurosci 1 ()93:':~:'J-II -q .
,""\ ':' ~ : tc~; 3J . ~ .. :~~ ; .; . ~ . ~ ,' l : ~! ;;? :' ,'-. !:' . \i'.-: :;~: b l!!:!:· ~ tT.:' .. "· ' 1 " ,:~ -
j~ .'.
;) iral () r~; Uuu'! o\V in 'lhe d~c:!n.: b ra[e '.: al. 3r:lIn I ~..!" l )U i : (121) :2(J1)-1 - . .Vliller A.D. 'i ini ala \ ·IS . ··J l! stihu'Ia r dfl!ct, ,m ' he upper IIrw<ly. Brain Re~ Il) l ll1:736: 160--1..
-I-J.. \ 'Irller . .1,0. Yamaguchi T. Siniaala MS. Yates BJ. Ventral respiratory group bulbospinal inspiratory neurom participate in vestibular-respiratory retlexes. J Neurophysiol 1995:73: 1303-07.
45. Balaban CD. Vestibular nucleus projections to the parabrachial nucleus in rabbits: implications for vestibular influences on the autonomic nervous system. Exp Brain Res 1996;108:367-81.
46. LeDoux JE. Emotion, memory and the brain. Sci Am 1994;50-7.
47. Levy I, O'Leary JL. Incidence of vertigo in neurologic conditions. Trans Am Otol Soc 1947;35:329--47.
48. McCabe BF. Diseases of the end organ and vestibular nerve. In: Naunton RF, editor. The vestibular system. New York: Academic Press; 1975. p299-302.
49. Rudge R, Chambers BR. Physiological basis for enduring vestibular symptoms. 1 Neurol Neurosurg Psychiatr 1982;45: 126-30.
50. Page NGR, Gresty MA. Motorists' vestibular disorientation syndrome. J Neurol Neurosurg Psychiatr 1985: 48: 729-35.
51. Marks I, Bebbington P. Space phobia: syndrome or agoraphobic variant? Br Med 11976;12:30-3.
52. Marks 1. Space "phobia": a pseudo-agoraphobic syndrome. J Neurol Neurosurg Psychiatr 1981 ;+4:387-91.
53. Bronstein AM. Visual vertigo syndrome: clinical and PQSg,rograpb~ findings J Ne"w' Nenms"'S 1995'59-472 76.
J. M. Furman et al
54. Hallam R, Hinchcliffe R. Emotional stability: its relationship to confidence in maintaining balance. 1 Psychom Res 1991;35:421-30.
55. Pogany E. Uber den Hohenschwindel. Monatsschrift der Ohrenheilkunde Laryngorhinol 1958;92:209-13.
56. lacob RG, Woody SR, Duncan DB. Lilienfeld SO, Hirsch BE, Kucera GO, Furman JM, Durrant 1D. Discomfort with space and motion: a possible marker of vestibular dysfunction assessed by the ~itllational characteristics Ylll!stionnairc. J Psychopath B.:hav Assess 1994: 15::99-324.
57 . .Jac()b Rl~. Retlfern .vIS. Furman .1M. Optic tlowindu~etl ,way in :Ul.'(let~. Ji~urdt!r, ,l"OCI<lteL1 with 'pace ,1IlJ motion Jisc(Jmr'ort. J -\nx Disnrd ll)lJ) :'.l:-I 11-2:'.
-'~ . iO'urlll<ln !\-1. ') .. "urogr:mhy: u,e' Uld limitations. Baillie,c', C:i!1 :"-iC:lII'ol !LJ!)-I:.'(:UOI-13.
.5 1) . .Jacob :~(j. Furman :VI. Durralll . D. rurner 'iN!. l)urfac<! ,i':P~IIJl!IlCt:: ,l 1alanct! C 11111'01 ,trat<!':!~ in panic disorder ·.vnh agoraphubla. p,~ chol1l \-lell lin press).
00. Furman ,::vt. O'Leary DP. W()lfe JW. Changes in the hOrizontal vestlbulo-ocular retlex uf the rhesus monkey with behavioral and pharmacological alerting. Brain Res 1981 :206:490--1..
61. Theunissen EJ. Huygen PL. Golgering HT. Vestibular hyperactivity and hyperventilation. Clin Otolaryngol 1986: II: 161-9.
62. Yardley L. Watson S, Britton J, Lear S, Bird J. Effects of anxiety arousal and mental stress on the vestibulo-ocular reflex. Acta Otolaryngol (Stockh) 1995; 115:597-602.
63. Rothman BO, Hodges LF, Kooper R, Opdyke 0, Willard IS, North N. Effectiveness of computer generated (virtual reality) graded exposure in the treatment of acrophobia. Am J Psychiatr 1995;152(4):626-8.
64. Kennedy RS, Hettinger LJ, Lilienthal MG. Simulator sickness. In: Crampton GH, editor. Motion and space sickness. Boca Raton (FL): CRC Press, Inc.; 1990. p317--41.
65. Jennings RT. Managing space motion sickness. J Vestib Res (in press).
66. Elmund 1. Bowman JP. Morgan RJ. Vestibular influence on tongue activity. Exp Neurol 1983;8 I: 126--1.0.
67. Mameli 0, Metis F, Deriu PL. Visual and vestibular projections to tongue motoneurons. Brain Res Bull 1994;33:7-16.
68. Rossiter CD. Yates BJ. Vestibular intluences on hypoglossal geO'e actiyiQl" implicatiops too gb§W'f'fiYS apnea. Neurosci Lett 1996:211 :25 8.
Top Related