







Languages
Pages
Legal

Resilience and Posttraumatic Growth
Resilience
• dynamic developmental process
• positive adaption
• despite adversity or trauma
• ≠ personality trait or attribute
• Two-dimensional construct– Exposure to adversity– Positive adjustment outcomes
Posttraumatic Growth (PTG)
• growth process
• experienced positive change
• as a result of traumatic experience
• ≠ traumatic event itself, but aftermath
• Change beyond effective coping– Beyond pre-trauma level of adaption– Qualitative change across different domains
Posttraumatic Growth

Some changes associated with PTG
• Increased sense of personal strength• discover new perspectives about relationships• Identify salient characteristics in others
(pos. and neg.)• Modified priorities, shift in perspectives and
value systems– appreciate ‘smaller things’ in life– increased appreciation of life in general– richer religious, spiritual, and existential lives
(Calhoun & Tedeschi, 2004; Tedeschi & Calhoun, 2004)
PTG and posttraumatic stress symptoms
• Although benefits and positive change• Still distress and struggle• Less emotional well-being in individual reporting PTG
(compared to resilient)– contributes to growth process– facilitates constructive cognitive processing of trauma
• Attempts to make sense of trauma and aftermath• Productive ruminative process yields schema change• Supportive others
– provide means to craft narratives– offer new perspectives(Calhoun & Tedeschi, 2004)
Factors (potentially) affecting PTG
• Age (older)• Gender (female)• Severity and type of stressor/trauma• Higher income• More time since traumatic event• Existential awareness (life’s fragility)• Religiosity• Higher levels of social support
Calhoun & Tedeschi, 1999, 2004 (Milam et al., 2004)
Discussion
• Does this sound a bit like a cliché to you?
• So, what’s the evidence?
Measures of PTG
• Qualitative (indirect) measures– Secondary analysis of PTSD interviews– Coding for elements of PTG(Salter & Stallard, 2004)
• Quantitative measures– For adults: Posttraumatic Growth Inventory (Tedeschi
& Calhoun, 1996)– PTGI-Revised for Children and Adolescents
(Yaskowich, 2002)– Posttraumatic Growth Inventory for Children Revised
(PTGI-C-R) (Kilmer et al., 2009)– Perception of Changes in Self scale (Kazak et al., 2001)
Posttraumatic Growth Inventory for Children Revised (PTGI-C-R)
• Kilmer et al. (2009), used with 7-10 year-olds
• Two open ended questions• 10 items assessing PTG in five domains
– New possibilities– Relating to others– Personal strength– Appreciation of life– Spiritual changes

Other measures for children and adolescents
• Posttraumatic Growth Inventory for Children (PTGI-C) (Cryder et al., 2006)– 21 items from pool of 29 items (same five domains as
PTGI-C-R)
• PTGI-Revised for Children and Adolescents (Yaskowich, 2002)– 21 items (same five domains)
• Perception of Changes in Self scale (Kazak et al., 2001)– 1 open-ended question– 9 items
Other measures for children and adolescents
• Secondary analysis of PTSD interviews (Salter & Stallard, 2004)
– ‘framework’ technique (Ritchie & Spencer, 1994)
• Five steps (Familiarization, thematic framework, indexing, charting, interpretation)
– 3 areas of PTG• Perception of Self• Interpersonal relationships• Philosophy of life

PTG in children and adolescents
• Empirical studies with children and adolescents– Milam, Ritt-Olson & Unger (2004)– Barakat, Alderfer & Kazak (2006)
• Studies with young children– Salter & Stallard (2004)– Cryder, Kilmer, Tedeschi & Calhoun (2004)– Kilmer et al. (2009)
Adolescent with negative life events Milam, Ritt-Olson & Unger (2004)
• 435 adolescents (grades 9-12, m= 15.8y)– Predominantly Hispanic
• PTGI• Negative life events (within previous 3 years)
– Closed-ended checklist of ‘life change units’, including 10 major neg. events (Coddington et al, 1972)
– Common neg. life events• Death of family member (34%)• Move to new home (16%)• Loss of close friend (11%)• Major illness to family member (10%)• Parents divorce/separation (10%)

Adolescent with negative life events Milam, Ritt-Olson & Unger (2004)
• Mean PTG score was 3.56 (=mild amount)• No different in PTG between types of
events• No different in amount of PTG for gender,
ethnicity• Correlations between PTG and
– Age (+)– Religiosity (+) – Substance use (-)

Adolescent cancer survivorsBarakat et al. (2006)
• 150 adolescents cancer survivors (11-19 years)
• Hypothesis– More time since, and higher perceived
intensity of treatment = more PTG– Older age at diagnosis = more PTG
• PTG Measure– Perceptions of Changes in Self (PCS)
Kazak et al., 1996, 2001
Adolescent cancer survivorsBarakat et al. (2006)
• 84.7% of adolescents reported at least one positive consequence– 53% think about life– 42% plans for future– 41% how careful
• 32% reported 4+ pos. conseq.• PTG and other variables (correlations)
– Age at diagnosis (+), time since treatment (-), household income (n.s.)
– (perceived) past and current life threat, treatment intensity, PTSS (IES-R) (all correlations = +)
Children in road traffic accidentSalter & Stallard (2004)
• 158 7-18y old children• Secondary qualitative analysis of PTSD
interviews (CAPS-C), IES• 42% report PTG
– 37% of them also PTSD– Mean age of children reporting PTG = 16y
• Domains of PTG– Perception of Self
• least applicable• None used words ‘survivor’ or ‘victim’• Face reality of vulnerability

Children in road traffic accidentSalter & Stallard (2004)
• Domains of PTG– Interpersonal Relationships
• improved IR: 12% general, 20% with people involved in accident
• Relationships ‘closer’ ‘cemented’→ learning to disclose more about feeling, and ability to
express more openly – Philosophy of Life
• Most common theme• Appreciation of life (31%)• Reevaluation of what was important (13%)• Feeling ‘if there is something that you want to do, try do it-
don’t wait’• Few reports of a more relaxed approach to life
Children affected by a natural disaster (Cryder et al., 2004)
• Hurricane Floyd (Sept 1999)– 1 year later
• Of 321 contacted only 46 (15%)– 6-15 years (m=9.54y)– 50% evacuated/displaced
• PTGI-C• PTG score 37-84 (m=65.11)• Correlations with other variables
– Sign. corr. with competency belief– No other sign. corr. (e.g. age, gender, severity, social
support)
Children affected by a natural disaster (Kilmer et al., 2009)
• Hurricane Katrina (Aug 2005)– T1=1y later, T2=2y later
• 68 7-10 year olds (m=8.3y)– Majority African American– 73.5% prior Trauma
• PTGI-C-R (range 0-30)– T1=20, T=19.2 (50% avg., 10.6% little)
• No gender difference
– Correlations with other variables• Sign corr. With subjective response to HK and PTSS (only PTSS in
regression)• No corr. with age• T1 PTG only sign. predictor of T2 PTG
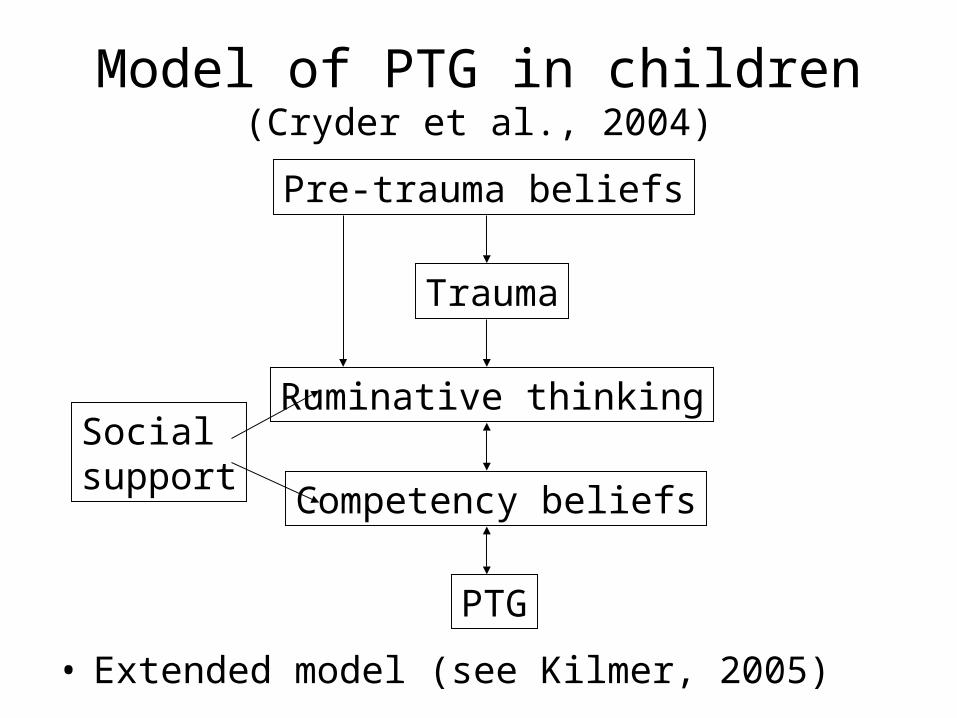
Model of PTG in children(Cryder et al., 2004)
• Extended model (see Kilmer, 2005)
Pre-trauma beliefs
Trauma
Ruminative thinkingSocialsupport
Competency beliefs
PTG
Critique
• Hypothesized model– Several factors remain untested– Cryder et al. discuss link between PTG and
social support (but no sign. Corr.)
• No control groups– Normal developmental process?
• Positive bias
A positive bias?
• N=276 adults• Two factors
– Exposure (to traumatic event)• 42.5% exposure
– Method (PTGI)• linked to stressful event• not linked to specific event (generally past 4 years)
• PTG higher in unlinked group (with event exposure) – sign. Interaction exposure x method
• Suggests that growth underestimated, rather than inflated
– PTGI usually linked to specific event
Development and PTG
• Cognitive maturity and ‘psychological mindedness’– Interpersonal awareness and insight (Cryder et al., 2004)
• Affective quality of change and learning• Response reflects dev. level/task
– Lieberman & Van Horn (2004)• Understand + internalize depending upon
cognitive/emotional capacities (Osofsky, 2004)• Cognitive capabilities may influence understanding +
appraisal of trauma (Hasan & Power, 2004)– Attributions about circumstances– Repertoire of coping skills/strategies– Ability to marshal resources effectively– Capacity to attend to and report internal experiences (Cryder et
al. 2004)
Development and PTG
• Possibly years before PTG (on some dimensions) manifests in children
• Positive relationship between age and PTG (Milman et al., 2004)– Cognitive maturity necessary
• PTG process maybe qualitatively different in children– Schemas not as clearly set in children– New experiences incorporated into internal
representations– Children more vulnerable (Janoff-Bulman, 1992)
Age and PTG
• Barakat et al. (2006)– Age 5y at diagnosis as cutoff– Age 5 shift in cognitive functioning, better process and
reflect on their experiences (Alderfer et al., 2003)
– < 5y fewer positive consequences• Only 6.3% reported 3+ positive changes• In comparison: 44% of > 5y reported 3+ pos. changes
• Childe age >5y more PTSS– But sign. Correlation between PTG and PTSS in both
>5y and <5y
Relevant research areas‘Theory of mind (ToM)’
• Understanding of own and others mental states– Desires, beliefs, emotions, intentions
• Important area in developmental psyc
• Age 5y important shift in development
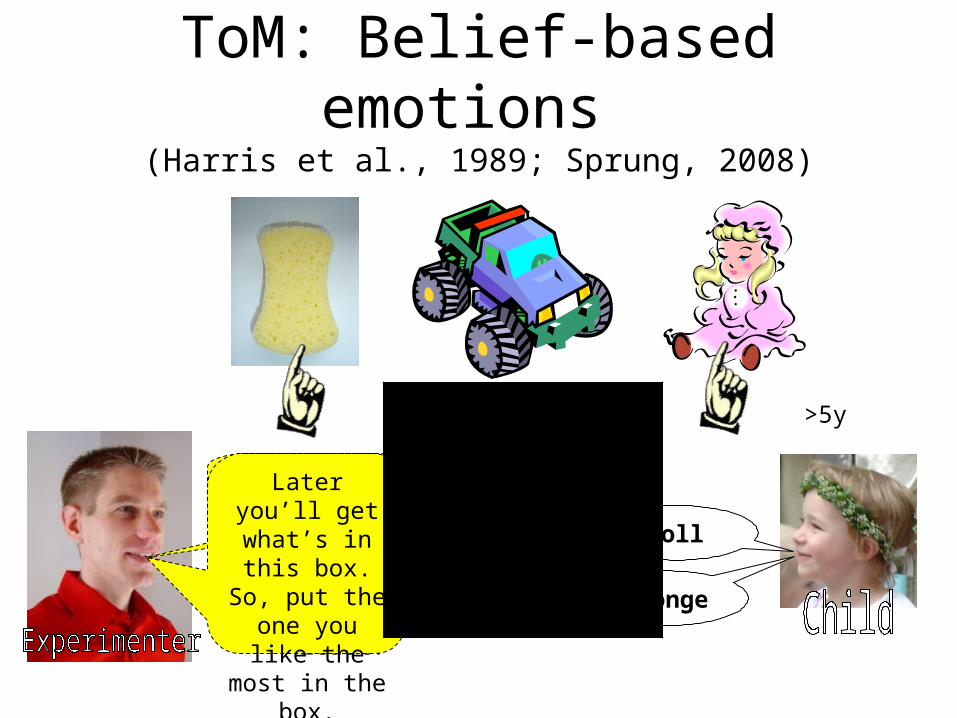
ToM: Belief-based emotions (Harris et al., 1989; Sprung, 2008)
Which one do you like the most?
spongeWhich one do you like the least?
doll
Later you’ll get what’s in this box. So, put the one you
like the most in the box.
>5y
ToM: Belief-based emotions (Harris et al., 1989; Sprung, 2008)
Now, let’s work on another task and later you’ get what’s in
the box.
How do you feel now, about what’s in the box?
>5y
ToM: Belief-based emotions (Harris et al., 1989; Sprung, 2008)
Very good, now you get what’s
in the box.
How do you feel now?
What’s in the box?What did you think is in the
box?
Before you open the box, how did
you feel
sponge
doll
< 5y
ToM: Introspection(Flavell et al., 1995)
Do not Do not thinkthink
While you where sitting in the no thinking chair, did you have no thoughts or did you have some thoughts?
No thoughts
…easy having no thoughts
< 8 years

Theory of mind
• Not mentioned in literature on PTG– Although Kilmer mentions ‘psychological
mindedness’
• Theory of mind and Trauma– More advanced ToM = more reports of PTSS
Sprung (2008)– PTG not assessed

Other relevant research areas‘internal working models’
• John Bowlby
• Attachment theorist (‘strange situation’)
• First caregiver-child, later extended to other people/situations
• Also not addressed in PTG lit.
Vulnerability versus protection
• Basic assumptions (safety, protection from harm, predictability) violated (Goldman, 2002)
• Loss of trust, meaning, faith• Formation of traumatic expectation distorting (Pynoos et
al., 1995)– Emotional, cognitive, moral concepts– Inner representations of self, object relations, social environment
• Disrupt sense of self/others, emotion regulation, explorative learning (Lieberman & Van Horn, 2004)
• Trauma in infancy/early childhood derails normative developmental course – (Lieberman & Van Horn, 2004)– Pynoos (1990)– Difficulties in multiple domains (Bosquet, 2004)
Vulnerability versus protection
• Children’s basic assumptions less firmly entrenched/embedded– Open to adaptive inputs– Protective
• Factors to help buffer against traumatic impact– Emotional caring/interpretive effort of others
(especially parents)– Supportive environment for child to attempt
understand, incorporate – Input of others can guide interpretation, reframe,
transform(Janoff-Bulman, 1992)
Discussion
• Do you think PTG in young children is possible?
• Some problems:– Extend of literature (two fields: clin. and dev.)– Dev. lit: children’s understanding quite
sophisticated• struggle about similar issues
– But limitations (e.g. introspection)
PTG: reality or illusion
• Real vs. illusory process (Sumalla et al, 2009)
• Real (positive) identity change
• Illusory process– Coping strategy

Resilience
Three facets of resilienceLepore & Revenson (2006)
• Recovery– Tree will bend to accommodate wind, so it won’t
break, and will return to upright position when wind stops
• Resistance– Tree stands still, undisturbed, in face of howling wind
• Reconfiguration– Tree not simply make temporary accommodation,
then resume original shape– instead, it changes its shape (making it more resitant
to break in future winds)
Three facets of resilienceLepore & Revenson (2006)
• Recovery– Stressor disrupts a person’s normal state of functioning,– When stressor passes, person resumes her normal pre-stressor
level of functioning
• Resistance– People who exhibit normal functioning before, during, and after a
stressor (even long after a stressor)
• Reconfiguration– Individuals reconfigure their cognitions, beliefs, and behaviors in
manner that allows them to adapt to traumatic experiences– Possibly withstanding future trauma

Discussion
• What’s normal response following traumatic event?– E.g. loss of a loved one
Resilience an ordinary phenomena(Masten, 2001)
• Originally (1970s): something special, remarkable about resilient children (‘invulnerable’)
• But ordinary phenomenon– Common operation of basic human adaption
systems– If major systems intact function well– If impaired, adversity = risk
Two kinds of judgments
(1) Threat (Not resilient, if no threat)– Risks, such as: low SES, negative life events,
community trauma, etc. (also cumulative)– Co-occur with psychosocial competence,
psychopathology, health– Risk gradients can be inverted to ‘assets’ or
‘resources’– Pure risk = car accident, pure asset = talent or friend– Mostly pos. and neg. end
• e.g. good parenting vs. poor parenting• Competent parents produce fewer stressful fam. life events
(risks), choose to live in neighborhoods with low crime (risks), good community resources (assets), more likely to hire tutors (assets)

Two kinds of judgments
(2) Quality of adaption or dev. outcome assessed or evaluated as ‘good’ or ‘OK’(a) Meeting major expectations of a given
society or culture (=salient developmental tasks, competence criteria, cultural age expectation) (Elder, 1998; Masten et al., 1998)
(b) Absence of psychopathology or low level of symptoms and impairment (Tiet et al., 1998)
(c) Both a+b (Greenberg et al., 1999)
Related question
• External adaption criteria– Accommodation, achievement, absence of
delinquency
• Internal– Psychological well-being, low level of distress
• Or both (Luther et al. 2000)
Historical overview
• Atypical schizophrenics (Garmezy, 1970)• Children from mothers with schizophrenia (Garmezy, 1974;
Masten et al., 1990)• Emmy Werner’s groundbreaking studies with Children in
Hawaii (Werner et al., 1971; Werner & Smith, 1977)• Studies of multiple adverse conditions (search for
protective factors)– Low SES– Parental mental illness– Urban poverty – Community violence– Chronic illness– Catastrophic live events

Models/approach to resilience(Masten, 2001)
• Variable focused– Link among measures of degree of risk/or
adversity, outcome, potential quality of individual or environment (to compensate/protect)
• Person focused– Compare people with different profiles (within
or across time) on sets of criteria to ascertain what differentiates resilient from non resilient children
Variable focused studies
• Compensatory effects– Enough positive assets could offset the
burden in child’s life from one or many risk influences
• Three models– Main effect– Indirect– Interaction
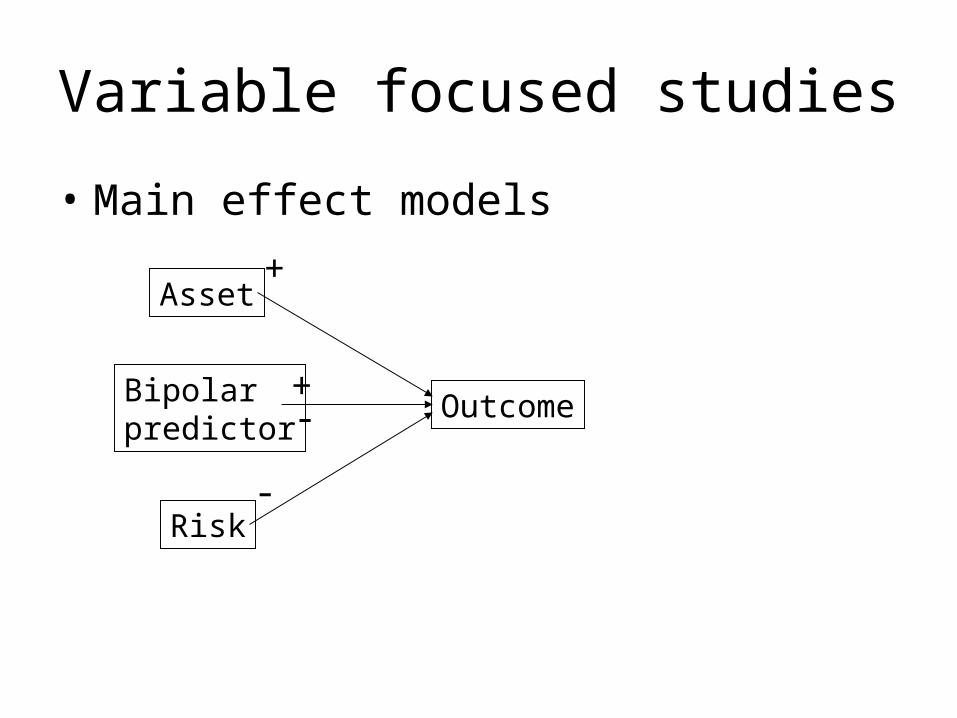
Variable focused studies
• Main effect models
Asset
Bipolarpredictor
Risk
Outcome
-
+
-+
Variable focused studies
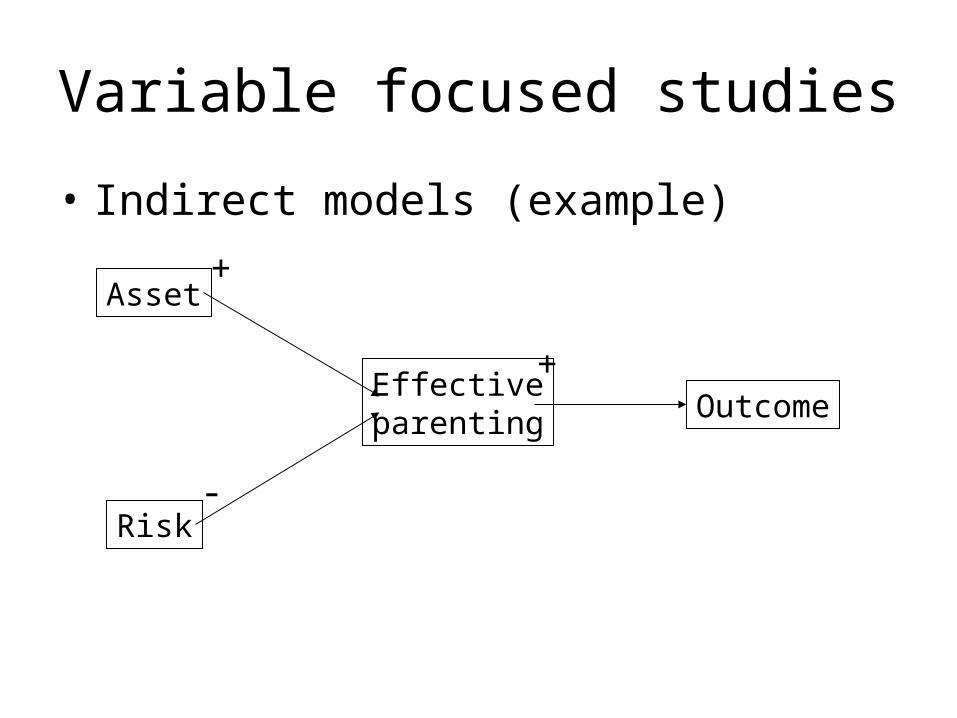
• Indirect models (example)
Asset
Effectiveparenting
Risk
Outcome
-
+
+
Variable focused studies
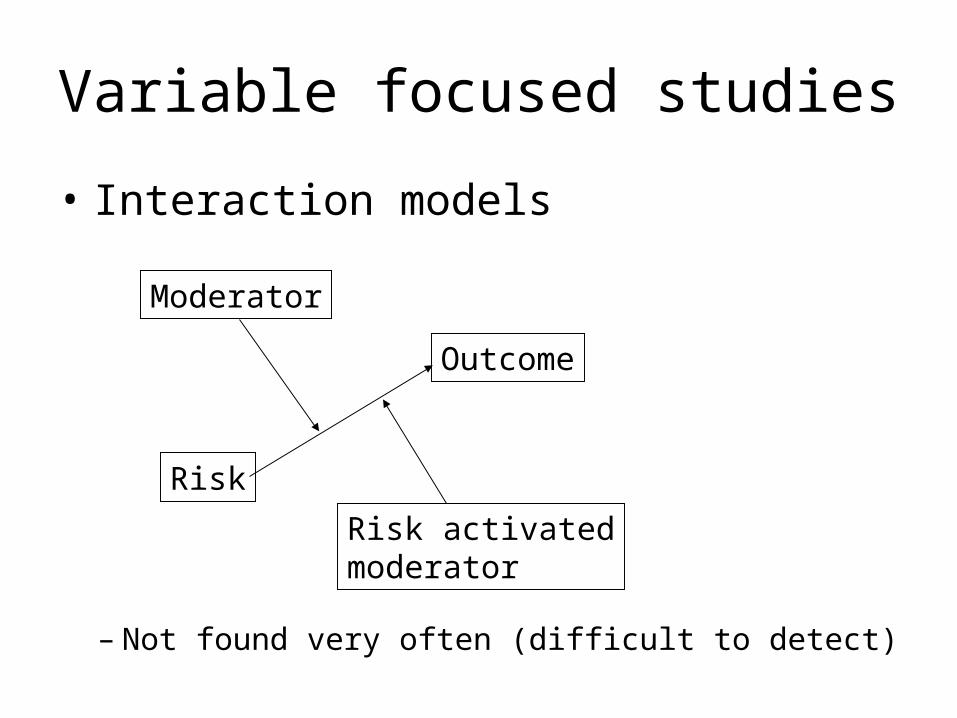
• Interaction models
Moderator
Risk activatedmoderator
Risk
Outcome
– Not found very often (difficult to detect)

Variable focused studies
• Factors emerging– Parenting quality– Intellectual functioning– SES– Positive self-perception
• Broad, pervasive corr. with multiple domains of adaptive behavior

Person focused studies
• Single case studies (Masten & O’Connor, 1984)• Groups of individuals with patterns of good
versus poor adaptive functioning (in context or high vs. low risk/threat)– Two groups from same high-risk groups (Werner &
Smith, 1982; Cowen et al., 1984)– Low risk groups– Variety of ‘stress-affected’ and ‘stress-resilient’

Person focused studies
• Emerging profile (Masten, 2001)– Average or better competence on three
salient domains• Academic• Conduct• Social
– Resulting in similar psychosocial resources• intellectual functioning• Parenting quality• Positive self-concepts

Pros and Cons
• Variable focused+ Max. stats power, suitable for searching
specific links between predictor and outcome- Fail to capture striking patterns in lives of real
people, risk of losing sense of the whole
• Person focused+ variables assembled in naturally occurring
configuration, well suited for search for common and uncommon patterns in lives
- Can obscure specific linkages
Positive Psychology
• The role of positive emotions– Frederickson’s ‘broaden-and-built theory’
• More positive emotions = more resilient?
Top Related