






Languages
Pages
Legal

Regulation of peripheral circulation: introduction
Ion channels, membrane potential & vascular tone.Intrinsic control of resistance vessels
Metabolic controlAutoregulationEndothelial factorsExtrinsic control of resistance vessels
RMP = resting membrane potential
VSM = vascular smooth muscle
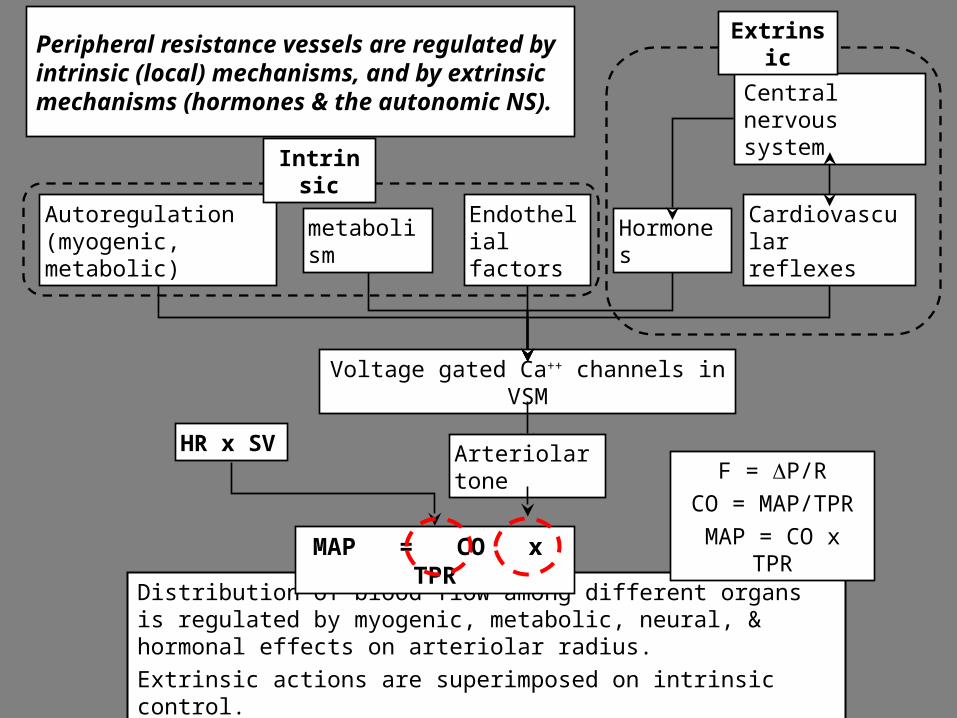
Peripheral resistance vessels are regulated by intrinsic (local) mechanisms, and by extrinsic mechanisms (hormones & the autonomic NS).
Distribution of blood flow among different organs is regulated by myogenic, metabolic, neural, & hormonal effects on arteriolar radius.
Extrinsic actions are superimposed on intrinsic control.
F = DP/R
CO = MAP/TPR
MAP = CO x TPR
Voltage gated Ca++ channels in VSM
HR x SV
Endothelial factors
metabolismAutoregulation (myogenic, metabolic)
Intrinsic
Arteriolar tone
Cardiovascular reflexes
Hormones
Central nervous system
MAP = CO x TPR
Extrinsic

Excitation contraction coupling in vascular smooth muscle
SERCA = sarcoplasmic reticulum Ca++ ATPase
Ca++
Extracellular Ca++
Ca++ stores
Ca++
Ryanodine receptor(SR Ca++ release channel)
Contractile mechanism
Sarcoplasmic recticulum
SR Ca++ ATPase
Ca++
Ca++Na+
L-type Ca++ channels (dihydropyridine receptors) are voltage gated, open with depolarization of cell membrane
No T tubules and no fast Na+ channels.Ca++ enters cells via L-type Ca++ channels.
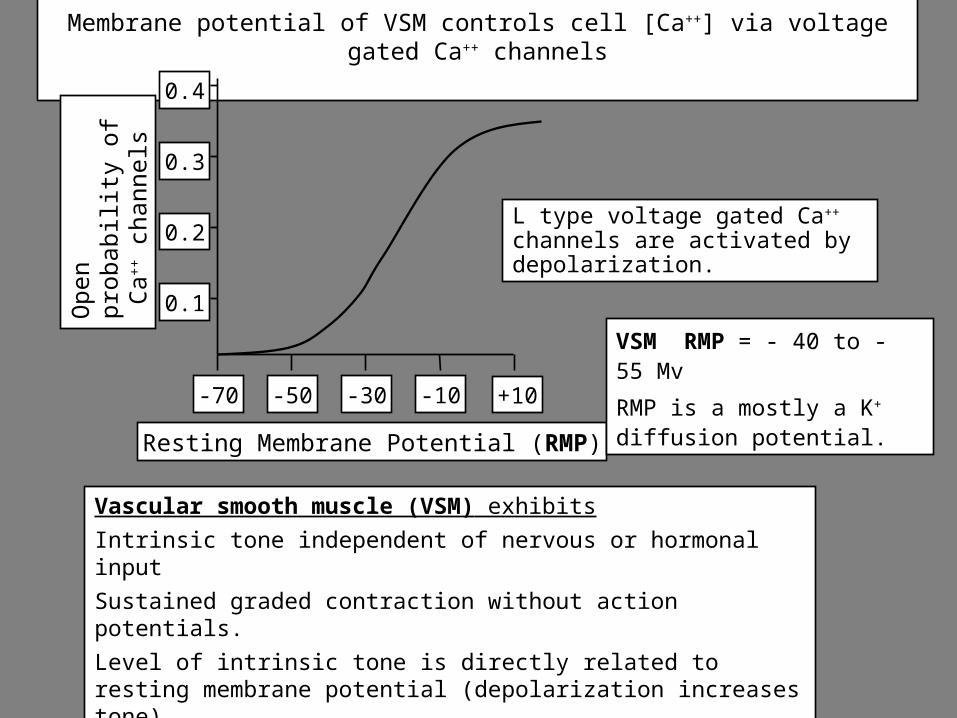
Membrane potential of VSM controls cell [Ca++] via voltage gated Ca++ channels
Vascular smooth muscle (VSM) exhibits
Intrinsic tone independent of nervous or hormonal input
Sustained graded contraction without action potentials.
Level of intrinsic tone is directly related to resting membrane potential (depolarization increases tone).
Nervous & hormonal control is superimposed on intrinsic tone.
-70 -50 -30 -10 +10
Ope
n pr
obab
ility
of
Ca+
+ c
hann
els
0.2
0.1
0.3
0.4
Resting Membrane Potential (RMP)
L type voltage gated Ca++ channels are activated by depolarization.
VSM RMP = - 40 to - 55 Mv
RMP is a mostly a K+ diffusion potential.
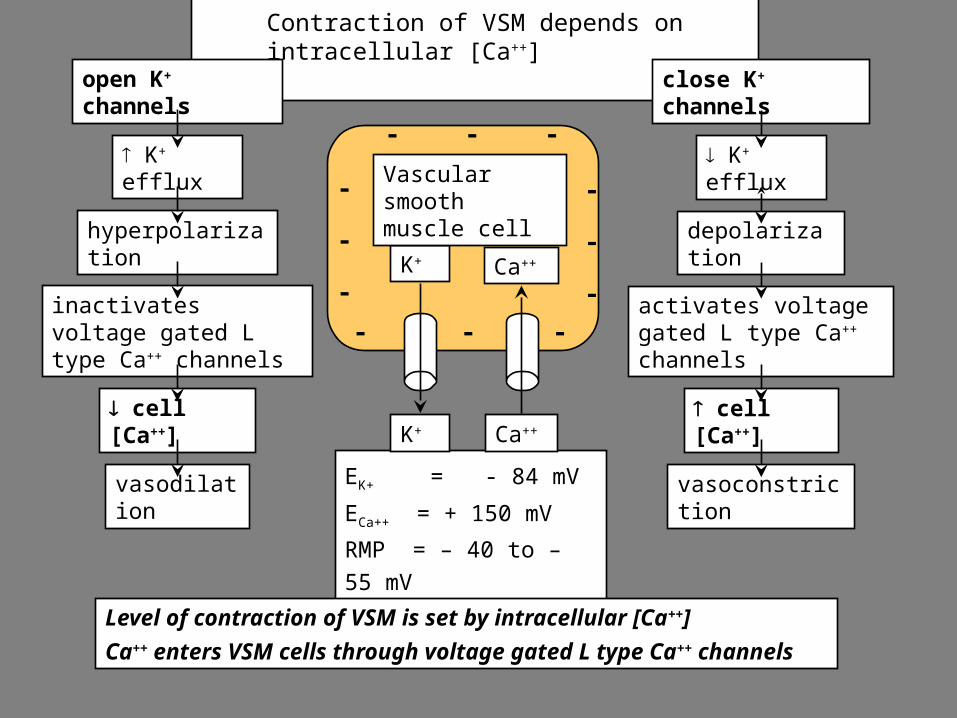
Contraction of VSM depends on intracellular [Ca++]
open K+ channels
K+ efflux
hyperpolarization
inactivates voltage gated L type Ca++ channels
cell [Ca++]
vasodilation
close K+ channels
K+ efflux
depolarization
activates voltage gated L type Ca++ channels
cell [Ca++]
vasoconstrictionEK+ = - 84 mV
ECa++ = + 150 mV
RMP = – 40 to – 55 mV
Level of contraction of VSM is set by intracellular [Ca++]
Ca++ enters VSM cells through voltage gated L type Ca++ channels
K+
-
-- -
- -
Ca++
Vascular smooth muscle cell
-
-
-
-
-
-
Ca++K+
Vasoactive hormones & voltage gated L type Ca++ channels
Vasoconstrictors either
Open Ca++ channels directly or
Depolarize the cell membrane which opens Ca++ channels.
Vasodilators either
close Ca++ channels directly or
hyperpolarize the cell membrane which closes Ca++ channels.
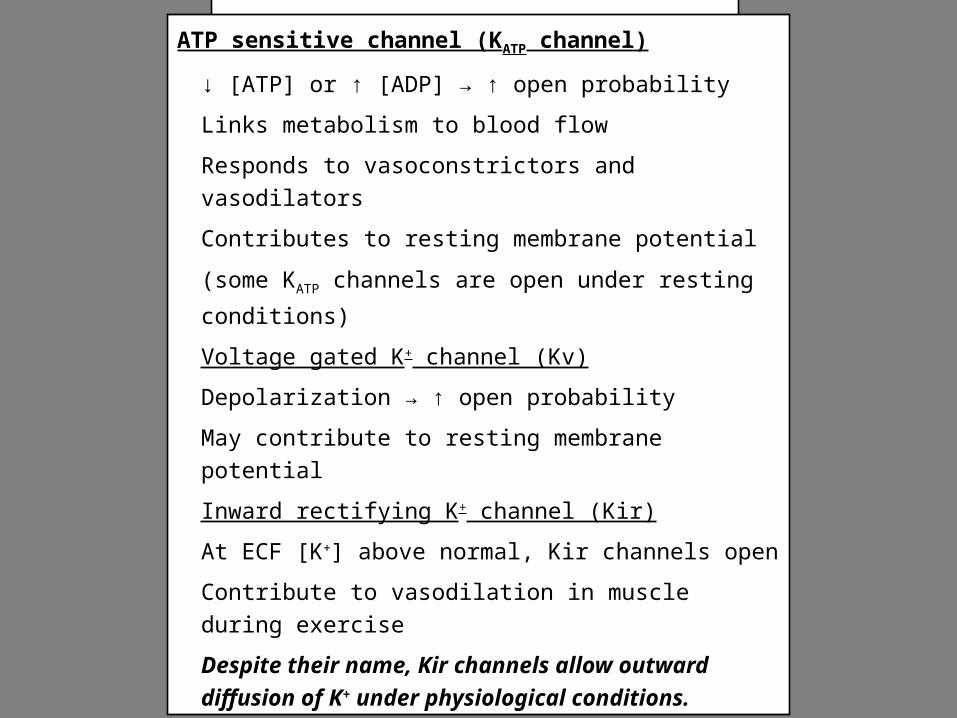
K+ channels in vascular smooth muscle (VSM)
ATP sensitive channel (KATP channel)
↓ [ATP] or ↑ [ADP] → ↑ open probability
Links metabolism to blood flow
Responds to vasoconstrictors and vasodilators
Contributes to resting membrane potential
(some KATP channels are open under resting conditions)
Voltage gated K+ channel (Kv)
Depolarization → ↑ open probability
May contribute to resting membrane potential
Inward rectifying K+ channel (Kir)
At ECF [K+] above normal, Kir channels open
Contribute to vasodilation in muscle during exercise
Despite their name, Kir channels allow outward
diffusion of K+ under physiological conditions.
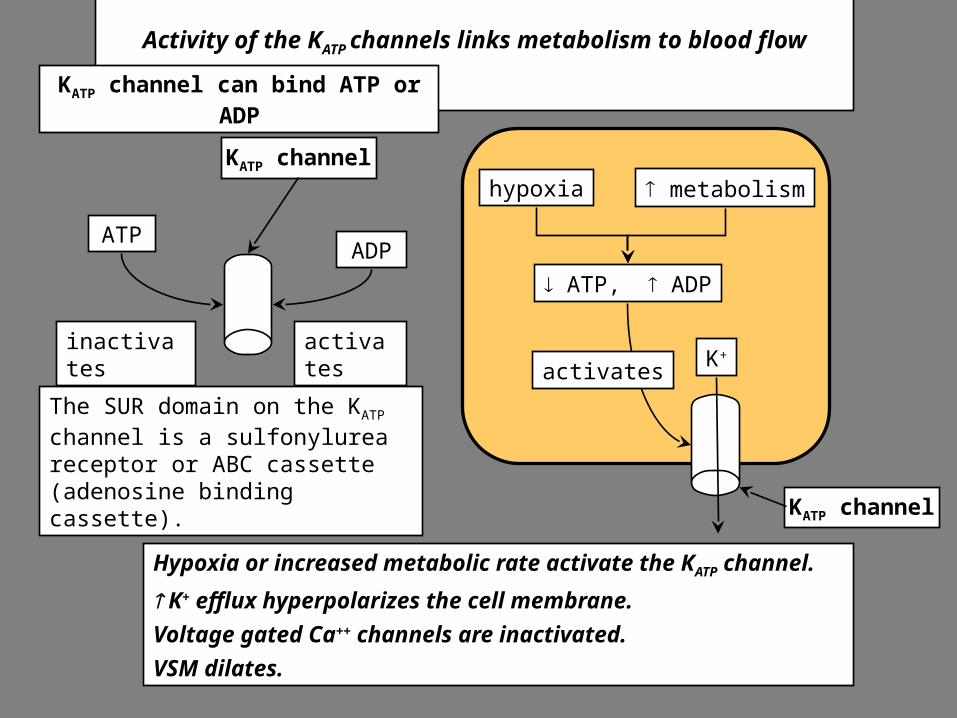
KATP channel
metabolismhypoxia
K+
ATP, ADP
activates
Activity of the KATP channels links metabolism to blood flow
Hypoxia or increased metabolic rate activate the KATP channel.
K+ efflux hyperpolarizes the cell membrane.
Voltage gated Ca++ channels are inactivated.
VSM dilates.
The SUR domain on the KATP channel is a sulfonylurea receptor or ABC cassette (adenosine binding cassette).
KATP channel can bind ATP or ADP
ATP
KATP channel
ADP
inactivates activates
Definition of metabolic control
Local blood flow is regulated by the local metabolic level of the tissue.
Increased metabolism produces vasodilators that cause an increase in flow.
The increased flow increases delivery of O2 & nutrients and the removal of CO2 &
waste products to match the new level of metabolism.
Possible vasoactive metabolites include: carbon dioxide, H+, nitric oxide, adenosine, inorganic phosphate ions, interstitial osmolality.
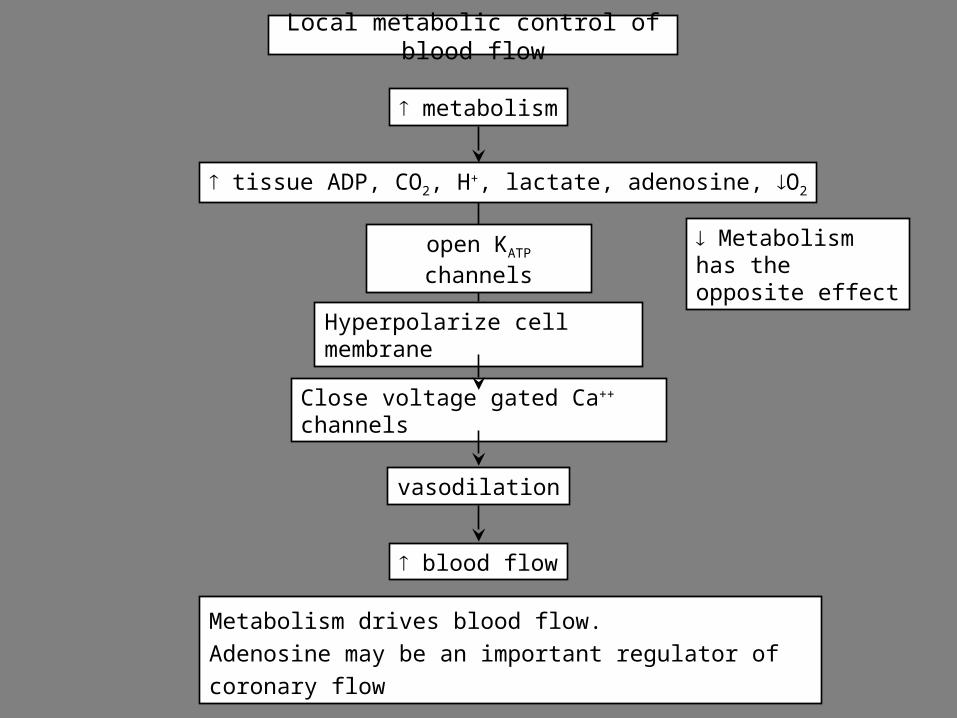
Local metabolic control of blood flow
Metabolism has the opposite effect
Metabolism drives blood flow.
Adenosine may be an important regulator of coronary flow
metabolism
tissue ADP, CO2, H+, lactate, adenosine, O2
vasodilation
blood flow
open KATP channels
Hyperpolarize cell membrane
Close voltage gated Ca++ channels
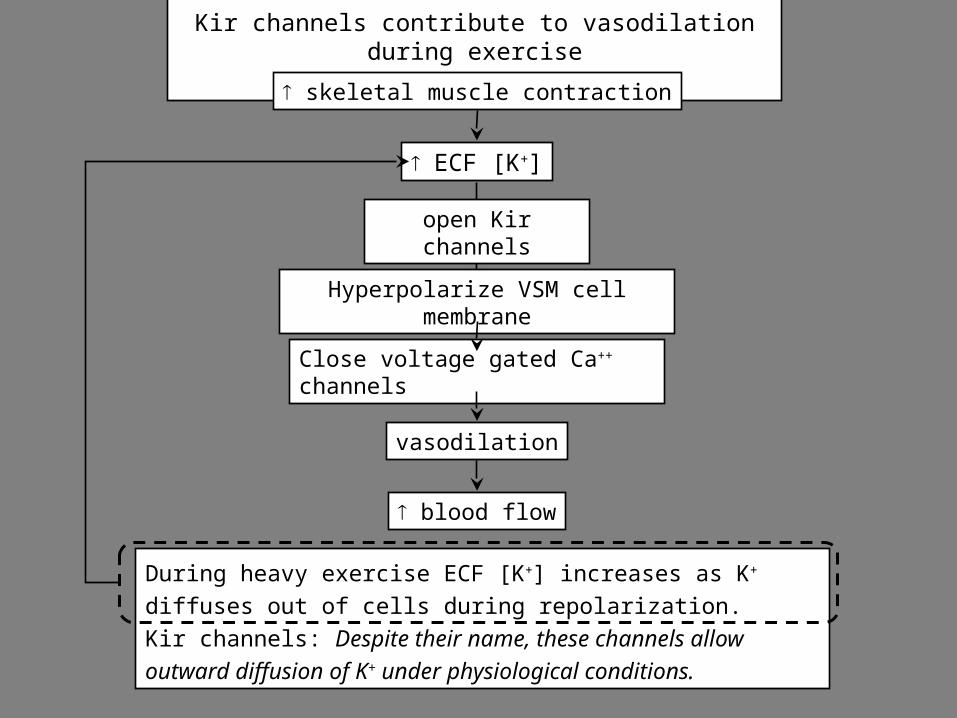
Kir channels contribute to vasodilation during exercise
During heavy exercise ECF [K+] increases as K+ diffuses out of
cells during repolarization.
Kir channels: Despite their name, these channels allow outward
diffusion of K+ under physiological conditions.
skeletal muscle contraction
ECF [K+]
vasodilation
blood flow
open Kir channels
Hyperpolarize VSM cell membrane
Close voltage gated Ca++ channels
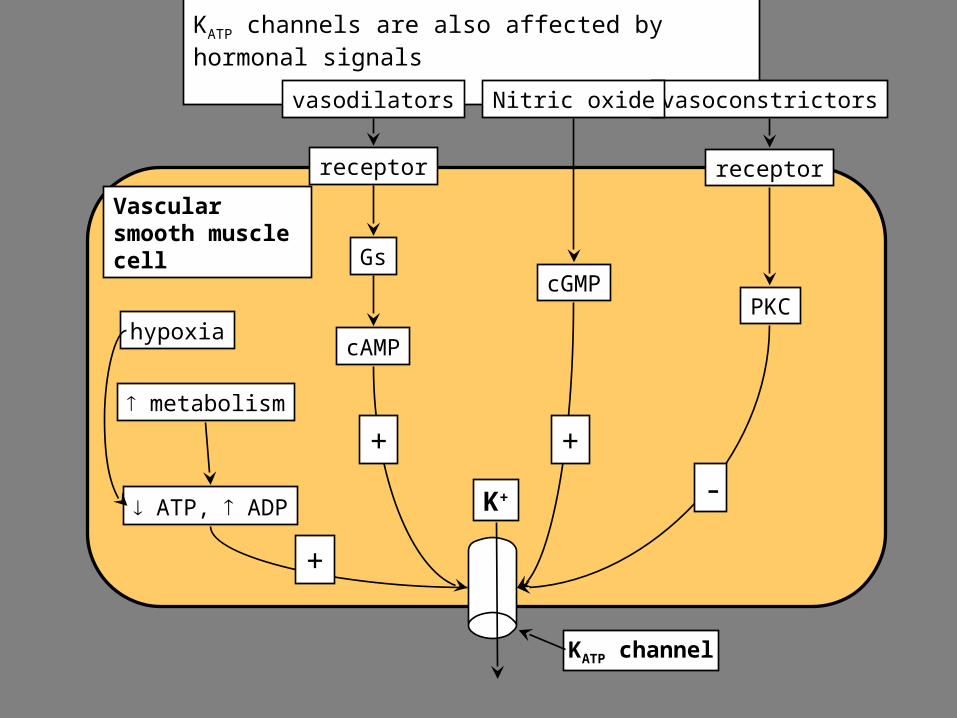
KATP channels are also affected by hormonal signals
KATP channel
Vascular smooth muscle cell
metabolism
hypoxia
vasodilators
receptor
K+ ATP, ADP
cAMP
Gs
vasoconstrictors
receptor
PKC
-
+
Nitric oxide
cGMP
++
Hormones that act via KATP channels
VasodilatorsAdenosine (coronary & renal circulation)EpinephrineNitric oxideANP (atrial natriuretic peptide)VasoconstrictorsAngiotensin IIVasopressinEndothelin
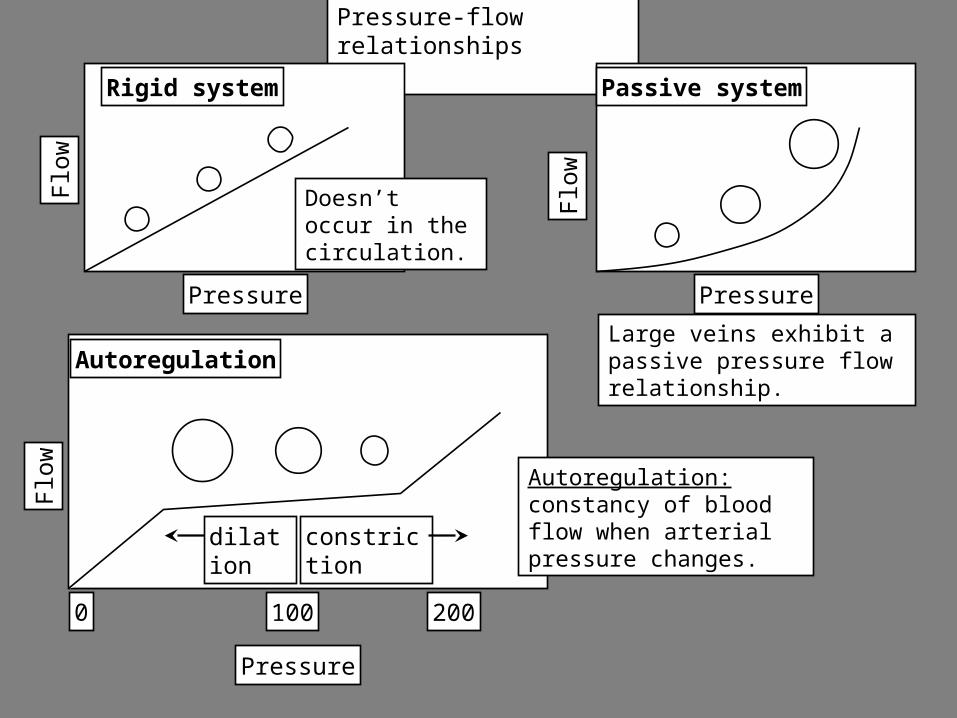
Pressure-flow relationshipsF
low
Pressure
Autoregulation
0 100 200
dilation constriction
Autoregulation: constancy of blood flow when arterial pressure changes.
Flo
w
Pressure
Passive system
Large veins exhibit a passive pressure flow relationship.
Flo
w
Pressure
Rigid system
Doesn’t occur in the circulation.
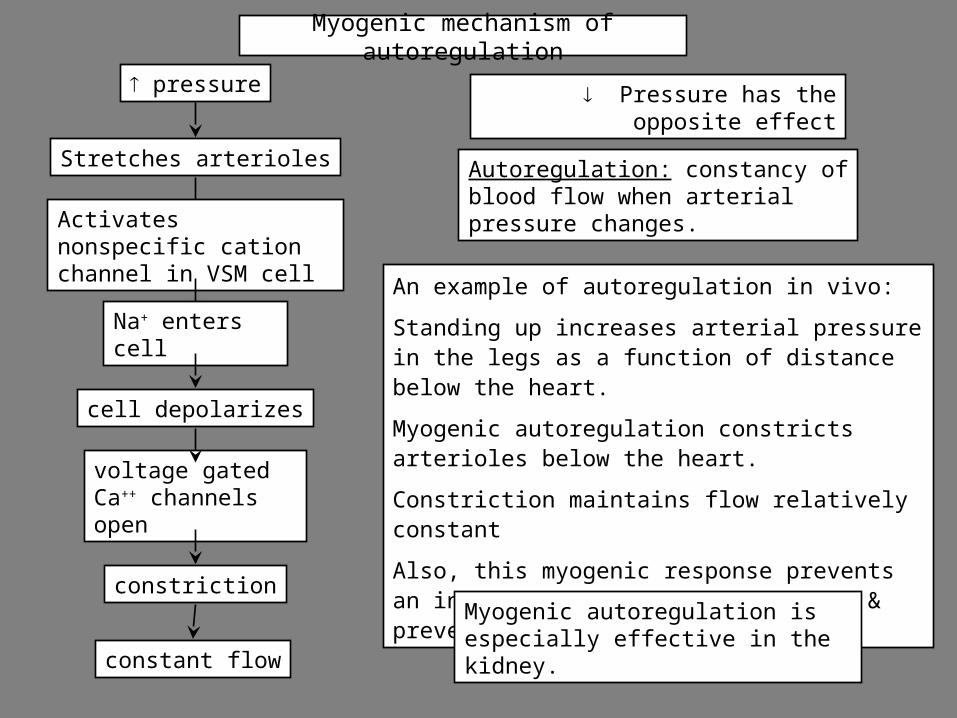
Myogenic mechanism of autoregulation
An example of autoregulation in vivo:
Standing up increases arterial pressure in the legs as a function of distance below the heart.
Myogenic autoregulation constricts arterioles below the heart.
Constriction maintains flow relatively constant
Also, this myogenic response prevents an increase in capillary pressure & prevents pedal edema.
Myogenic autoregulation is especially effective in the kidney.
pressure
Stretches arterioles
constriction
constant flow
voltage gated Ca++ channels open
cell depolarizes
Activates nonspecific cation channel in VSM cell
Na+ enters cell
Autoregulation: constancy of blood flow when arterial pressure changes.
Pressure has the opposite effect
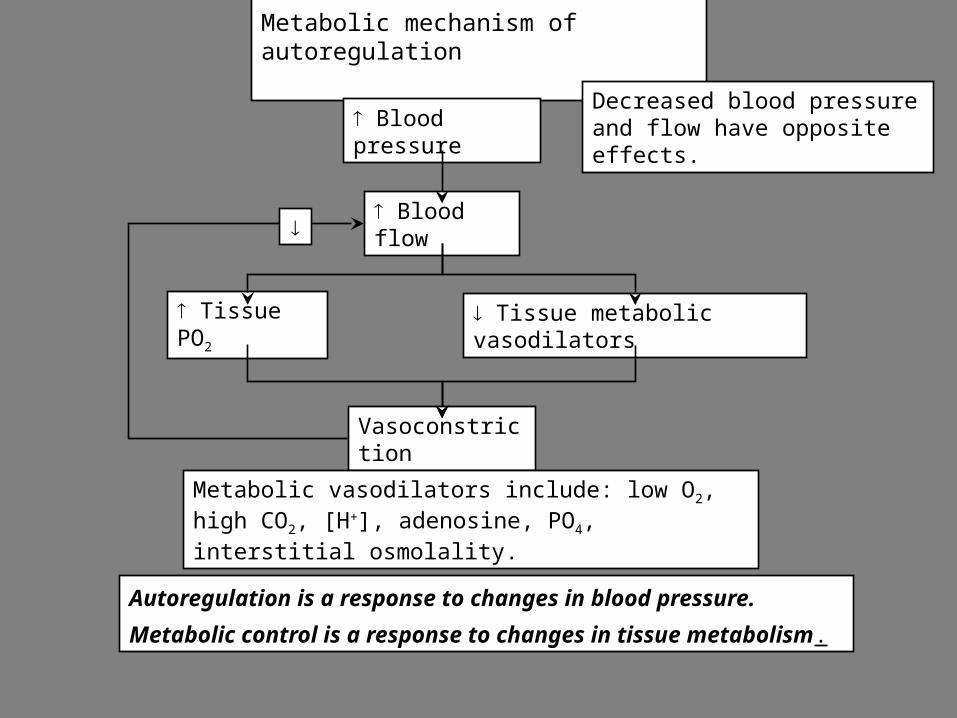
Metabolic mechanism of autoregulation
Decreased blood pressure and flow have opposite effects. Blood pressure
Blood flow
Tissue PO2 Tissue metabolic vasodilators
Vasoconstriction
Metabolic vasodilators include: low O2, high CO2, [H+], adenosine, PO4, interstitial osmolality.
Autoregulation is a response to changes in blood pressure.
Metabolic control is a response to changes in tissue metabolism.
Flo
w, m
l/min
Pre
ssur
e, m
m H
g
occlusion occlusion occlusion
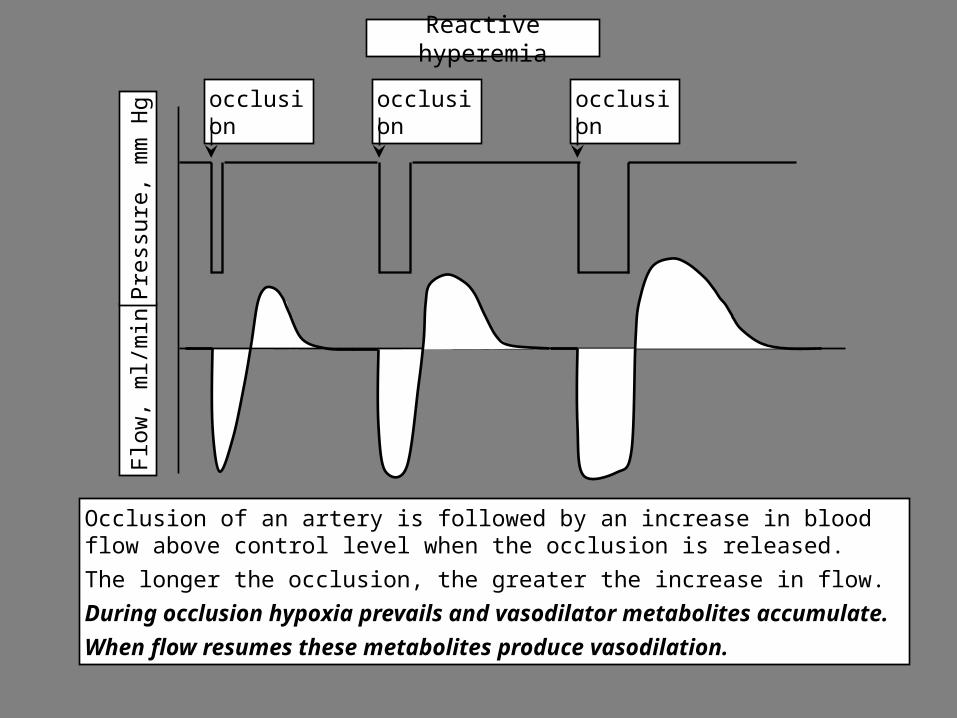
Reactive hyperemia
Occlusion of an artery is followed by an increase in blood flow above control level when the occlusion is released.
The longer the occlusion, the greater the increase in flow.
During occlusion hypoxia prevails and vasodilator metabolites accumulate.
When flow resumes these metabolites produce vasodilation.
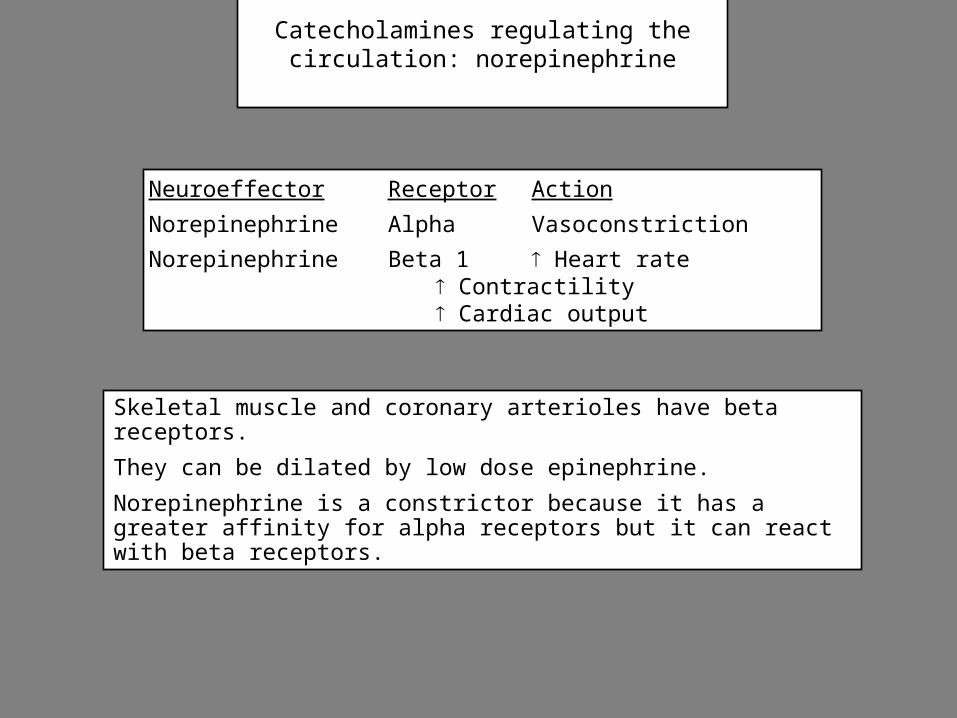
Catecholamines regulating the circulation: norepinephrine
Skeletal muscle and coronary arterioles have beta receptors.
They can be dilated by low dose epinephrine.
Norepinephrine is a constrictor because it has a greater affinity for alpha receptors but it can react with beta receptors.
Neuroeffector Receptor Action
Norepinephrine Alpha Vasoconstriction
Norepinephrine Beta 1 Heart rate Contractility Cardiac
output
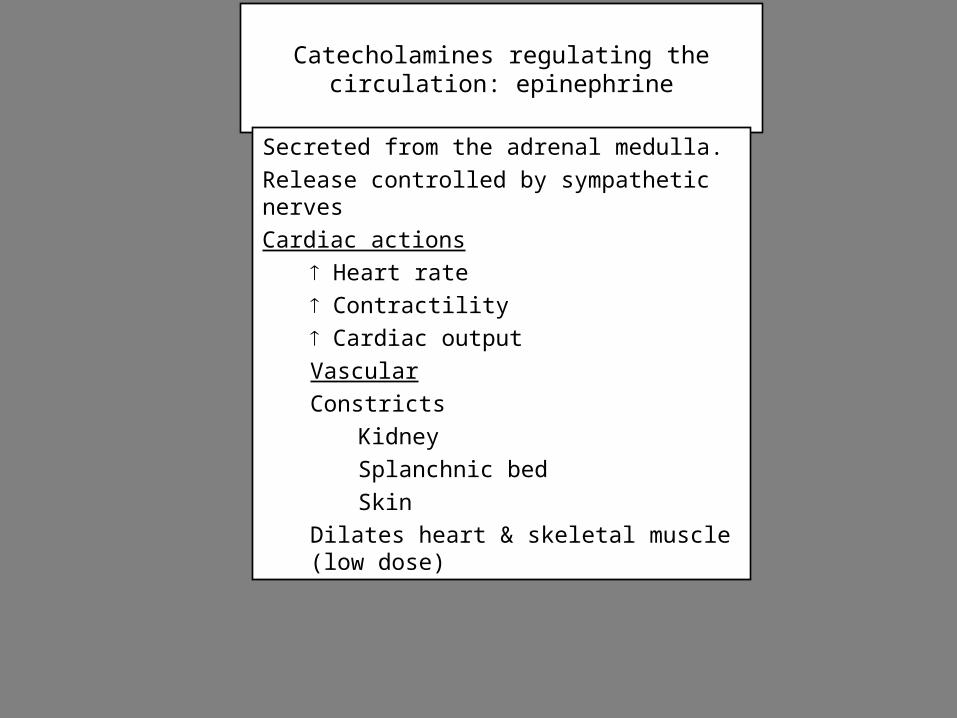
Catecholamines regulating the circulation: epinephrine
Secreted from the adrenal medulla.
Release controlled by sympathetic nerves
Cardiac actions
Heart rate
Contractility
Cardiac output
Vascular
Constricts
Kidney
Splanchnic bed
Skin
Dilates heart & skeletal muscle (low dose)
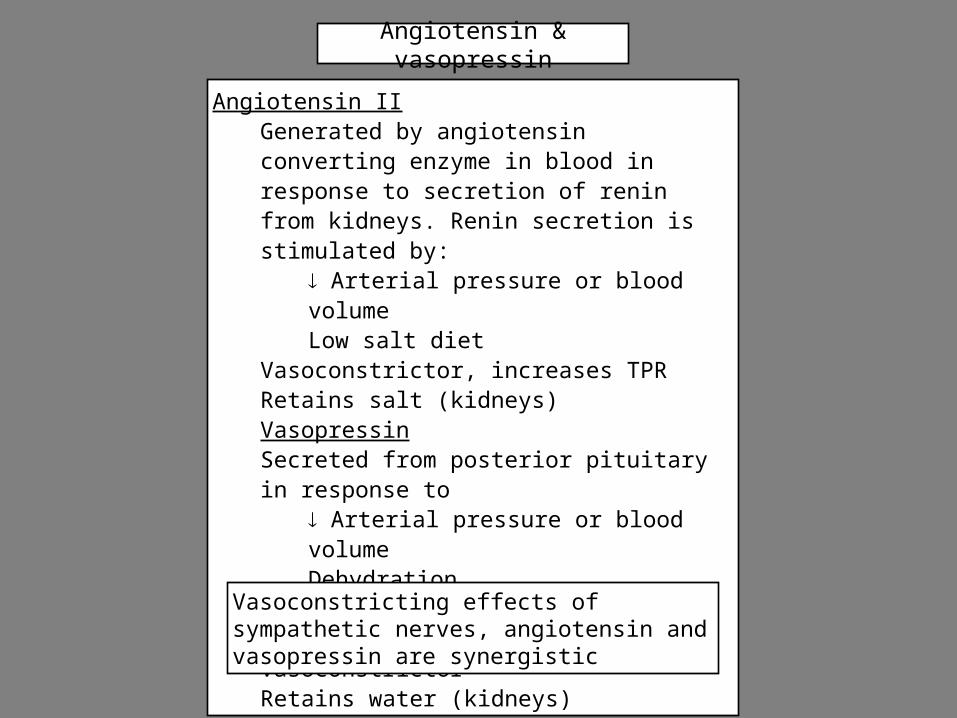
Angiotensin & vasopressin
Angiotensin IIGenerated by angiotensin converting enzyme in blood in response to secretion of renin from kidneys. Renin secretion is stimulated by:
Arterial pressure or blood volumeLow salt diet
Vasoconstrictor, increases TPRRetains salt (kidneys)VasopressinSecreted from posterior pituitary in response to
Arterial pressure or blood volumeDehydrationPainFear
VasoconstrictorRetains water (kidneys)
Vasoconstricting effects of sympathetic nerves, angiotensin and vasopressin are synergistic
Parasympathetic effects on blood flow
Neuroeffector Receptor Action
Acetylcholine Muscarinic Blood flow
Salivary glands
Gastrointestinal glands
Erectile tissue
Effects of acetylcholine on blood flow are indirect.
Ach acts on the endothelium to release nitric oxide.
NO diffuses to VSM & is a vasodilator.
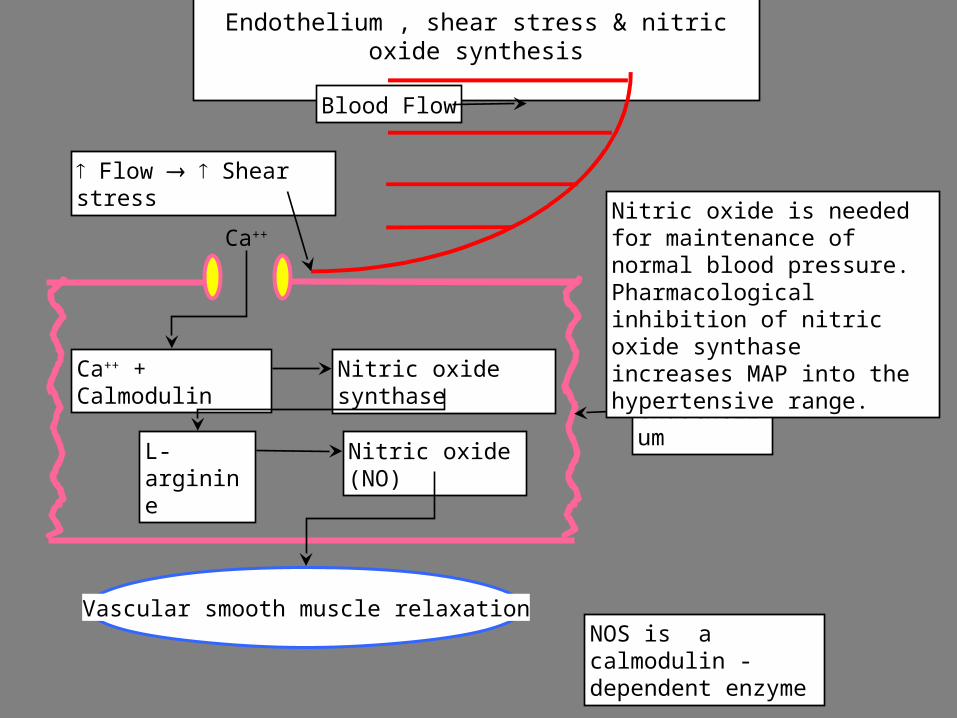
Endothelium , shear stress & nitric oxide synthesis
Vascular smooth muscle relaxation
Flow Shear stress
Ca++
L-arginine
Ca++ + Calmodulin Nitric oxide synthase
Nitric oxide (NO)
Blood Flow
NOS is a calmodulin -dependent enzyme
endothelium
Nitric oxide is needed for maintenance of normal blood pressure. Pharmacological inhibition of nitric oxide synthase increases MAP into the hypertensive range.
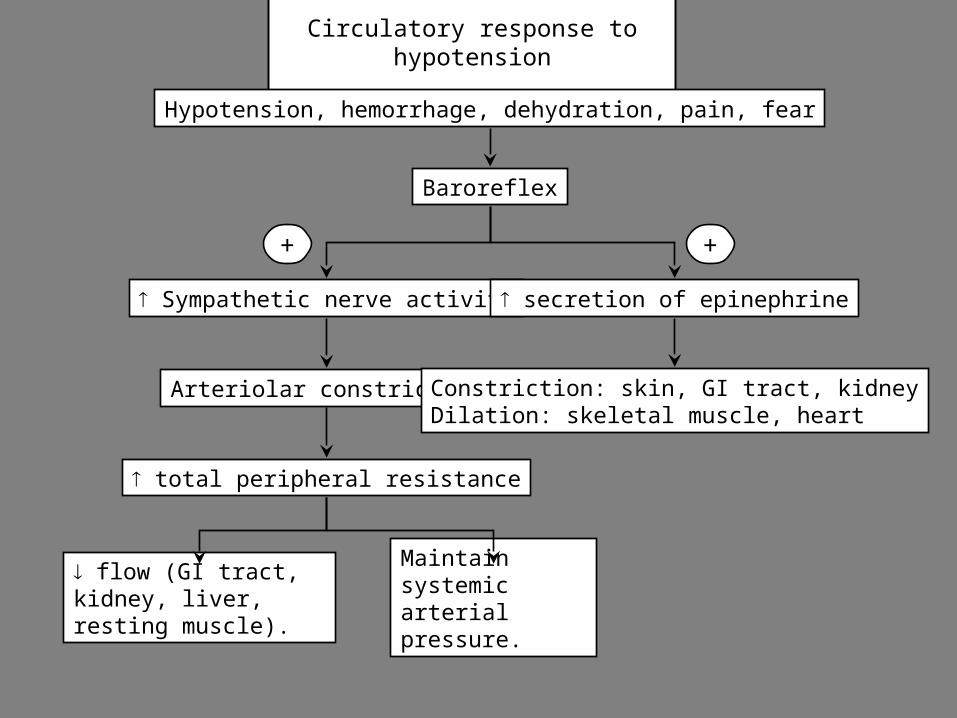
Circulatory response to hypotension
Sympathetic nerve activity
Arteriolar constriction
total peripheral resistance
flow (GI tract, kidney, liver, resting muscle).
Baroreflex
secretion of epinephrine
Constriction: skin, GI tract, kidneyDilation: skeletal muscle, heart
Hypotension, hemorrhage, dehydration, pain, fear
+
Maintain systemic arterial pressure.
+
Integration of sympathetic and metabolic control of circulation
In general:
At rest, blood flow is controlled primarily by a low level of sympathetic tone.
Increased work (muscle contraction, secretion, digestion, absorption etc) increases tissue metabolism.
Blood flow increases to match the new level of metabolism.
Blood flow decreases in inactive tissue due to increased sympathetic tone.
Effects of epinephrine on vascular smooth muscle are less important than sympathetic activity.
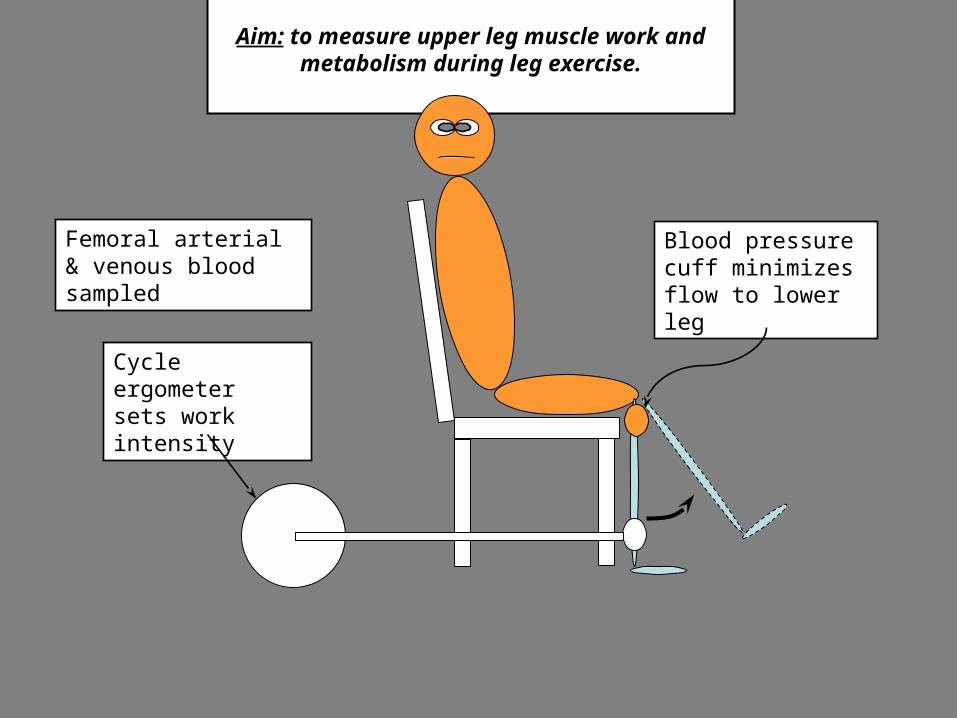
Aim: to measure upper leg muscle work and metabolism during leg exercise.
Cycle ergometer sets work intensity
Blood pressure cuff minimizes flow to lower leg
Femoral arterial & venous blood sampled
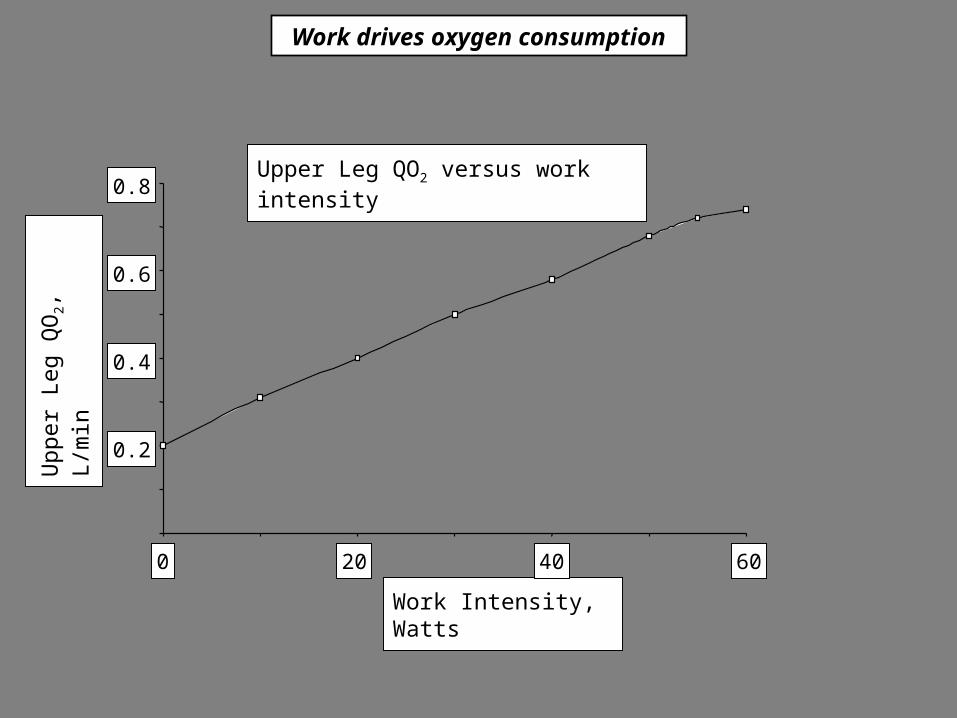
Upper Leg QO2 versus work intensity
Work Intensity, Watts
Upp
er L
eg Q
O2, L
/min
0
0.2
0.4
0.6
0.8
20 40 60
Work drives oxygen consumption

Graph shows leg blood flow as a function of work intensity
Maximal cardiac output is the limiting factor in aerobic exercise.U
pper
Leg
Blo
od F
low
, L/m
in
Work Intensity, Watts
20 40 600
2
4
6VO2 = (F)(O2A- O2V)
VO2 may be increased by
increasing flow &
increasing oxygen extraction
Maximum flow = 2L/min per kilogram of muscle.
If projected to the whole body, this flow would be equivalent to CO = 50 - 60 L/min. The capacity of skeletal muscle to receive blood is greater than the maximal cardiac output.
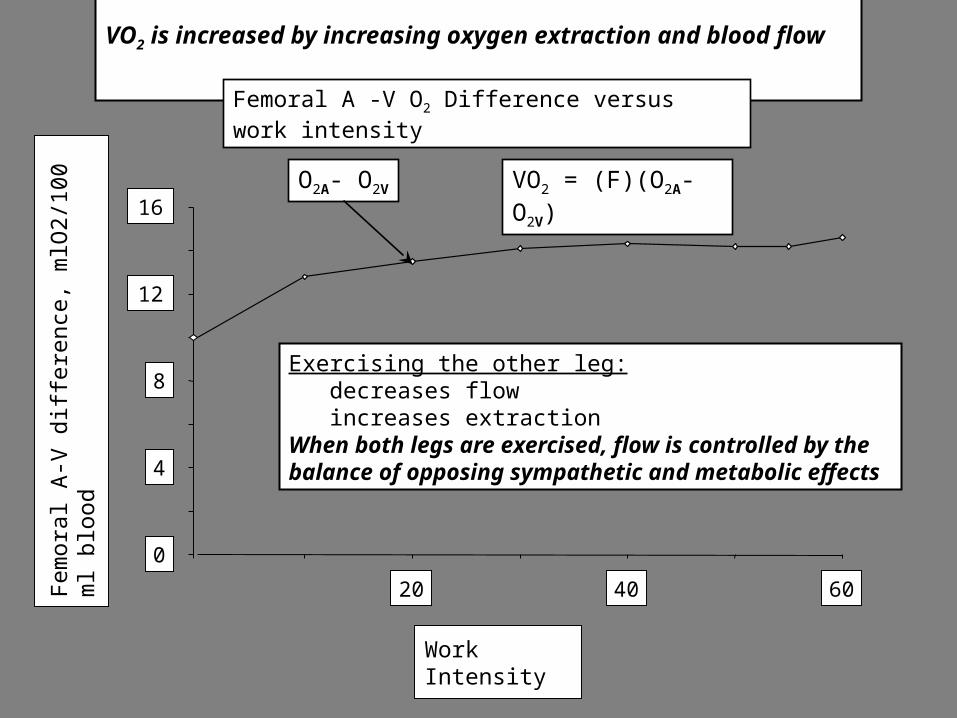
VO2 is increased by increasing oxygen extraction and blood flow
Femoral A -V O2 Difference versus work intensity
Work Intensity
Fe
mo
ral A
-V d
iffe
renc
e, m
lO2
/10
0 m
l blo
od
0
4
8
12
16
20 40 60
Exercising the other leg: decreases flow increases extractionWhen both legs are exercised, flow is controlled by the balance of opposing sympathetic and metabolic effects
VO2 = (F)(O2A- O2V)O2A- O2V

Summary
Arteriolar resistance determines distribution of flow between organs.
Vascular smooth muscle (VSM) has basal tone independent of nerves & hormones.
Tone of VSM is regulated by gradual changes in RMP & cell [Ca++].
Stretch depolarizes VSM & increases tone (myogenic response).
Increased local metabolism dilates VSM (metabolic regulation).
Autoregulation maintains constant flow when pressure changes (brain, heart, kidney,
skeletal muscle).
Local metabolic control predominates in heart & brain.
Muscle blood flow in active tissue is a balance between sympathetic (constrictor) &
metabolic (dilator) effects.
Neural control predominates in the splanchnic region and skin.
Sympathetic nerves, angiotensin II and vasopressin potentiate each other’s effects.
Top Related