






Languages
Pages
Legal


Red herring?
Susan Limb, MD
June 16, 2006
Allergy Grand Rounds

History of the red herring
• Curing process turns fish a red color and gives the fish a distinctive, pungent odor
• Dried fish tied to a string and trailed through the woods to train hunting dogs to follow a scent
• Later used by fugitives to confuse bloodhounds in pursuit
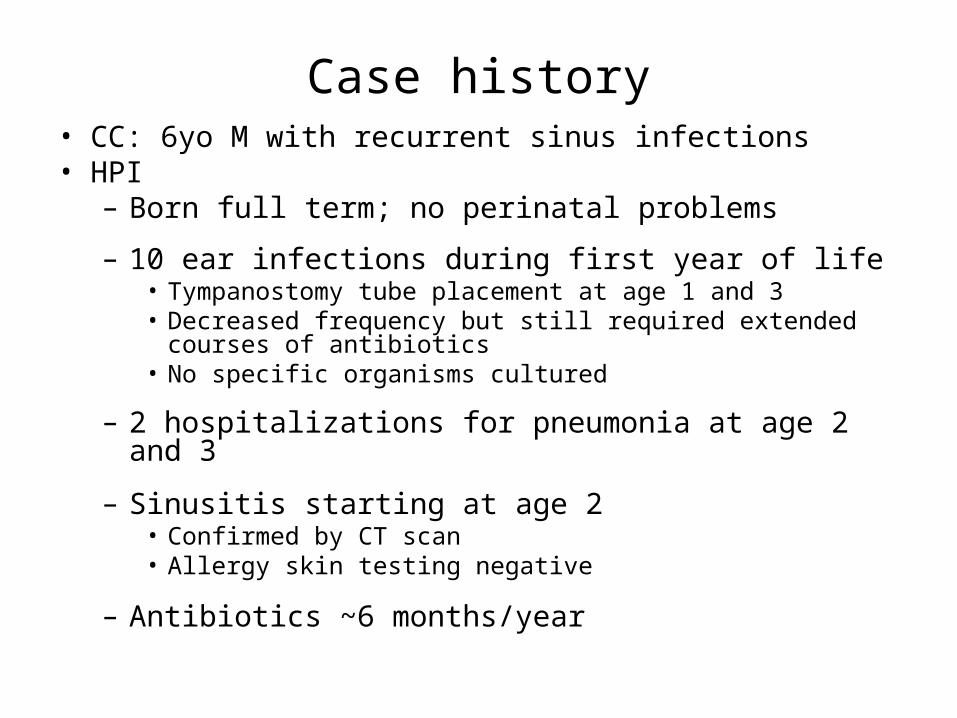
Case history• CC: 6yo M with recurrent sinus infections• HPI
– Born full term; no perinatal problems
– 10 ear infections during first year of life• Tympanostomy tube placement at age 1 and 3• Decreased frequency but still required extended courses of
antibiotics• No specific organisms cultured
– 2 hospitalizations for pneumonia at age 2 and 3
– Sinusitis starting at age 2• Confirmed by CT scan• Allergy skin testing negative
– Antibiotics ~6 months/year

Case history (cont.)• Past medical history
– Asthma diagnosed in infancy– 3 courses of prednisone– Occasional nocturnal and exertional cough
• No sputum production
• Medications– Flovent 110mcg 2 puffs BID– Albuterol PRN– Singulair 5mg QD– Rhinocort 2 sprays QD
• Immunizations– All age-appropriate vaccinations– Prevnar– Pneumovax– No antibody titers available

Family history
9yo6yo
• Recurrent sinusitis• Multiple sclerosis
No family history• autoimmune disease• fertility problems• situs inversus

Physical exam
• General: well-appearing 6 yo M• Vitals: T 372 BP 84/50 HR 92 17kg 115cm• HEENT:
– Nose –boggy turbinates, scant thick white mucus in nose, no polyps visualized
– Oropharynx –intact palate, 1-2+ tonsillar hypertrophy– Ears –TM scarring, PE tubes– No cervical LAD
• Cardiovascular –nl• Lungs –nl• Abd –nl, no hepatosplenomegaly• No skin or nail abnormalities

Laboratory evaluation
• Normal CBC with differential • Normal serum immunglobulin levels• Normal sweat chloride testing• Pneumococcal and H. influenzae antibody titers
pending• Mannan-binding lectin <50ng/ml (normal range
>100)
In a 6-year-old boy with intact humoral immune responses, is mannan-binding lectin (MBL) deficiency an explanation for recurrent sinusitis and otitis media?
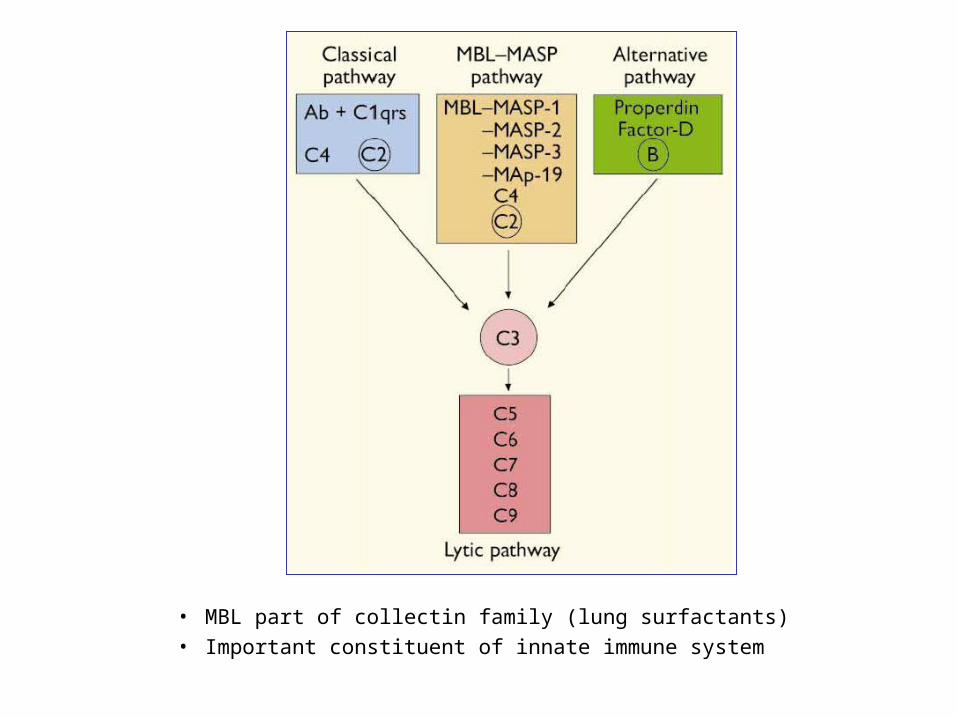
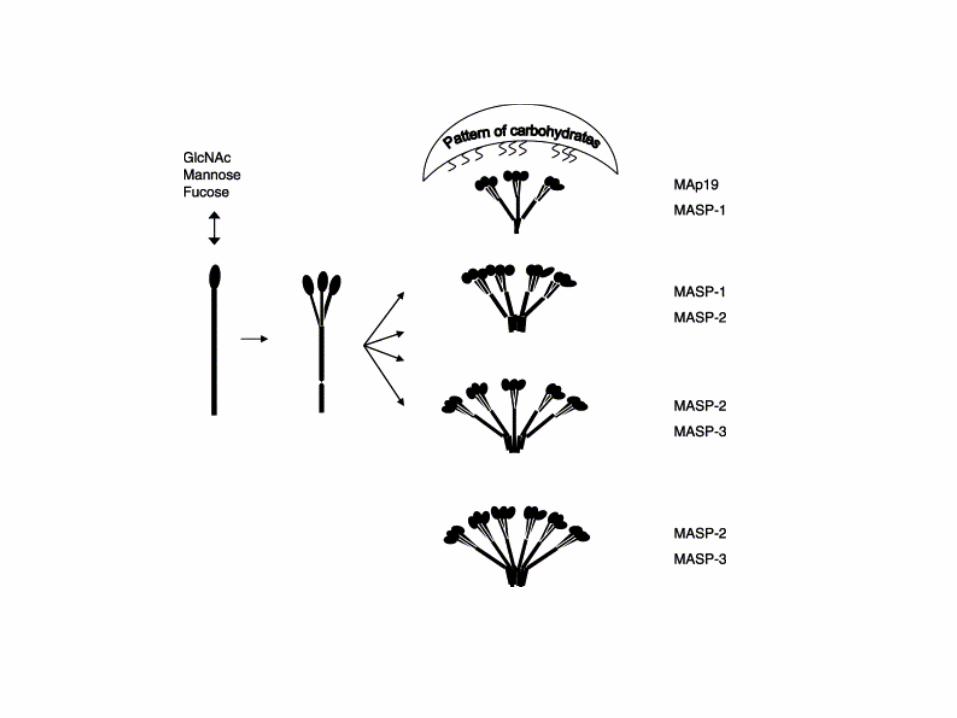
• MBL part of collectin family (lung surfactants)• Important constituent of innate immune system

Worthley, D. L., Bardy, P. G. & Mullighan, C. G.Mannose-binding lectin: biology and clinical implications.Internal Medicine Journal 35 (9), 548-555.doi: 10.1111/j.1445-5994.2005.00908.x
Worthley, D. L., Bardy, P. G. & Mullighan, C. G.Mannose-binding lectin: biology and clinical implications.Internal Medicine Journal 35 (9), 548-555.doi: 10.1111/j.1445-5994.2005.00908.x
Some clinically relevant microorganisms recognized by MBLBacteria Viruses Fungi Protozoa
Staphylococcus aureus HIV-1 and -2 Aspergillus fumigatus Plasmodium falciparum
Streptococcus pneumoniae
Herpes simplex 2 Candida albicans Cryptosporidium parvum
Streptococcus pyogenes Influenza A Cryptococcus neoformans Trypanosoma cruzi
Enterococcus spp.
Listeria monocytogenes
Haemophilus influenzae
Neisseria meningitidis
Neisseria gonorrhoeae
Escherichia coli
Klebsiella spp.
Pseudomonas aeruginosa
Salmonella montevideo
Salmonella typhimurium
Chlamydia pneumonia
Chlamydia trachomatis
Proprionibacterium acnes
Mycobacterium avium

• Commonly inherited missense mutations
• Additional polymorphisms in promoter and 5’-untranslated regions affect expression levels in serum
• Ethnic/racial variability– Reduced levels in up to 40% Caucasians– Very low levels in up to 8% Caucasians– Very low levels in ~13% Africans– Very low levels in ~3% Eskimos
• Additional variability with age
MBL deficiency
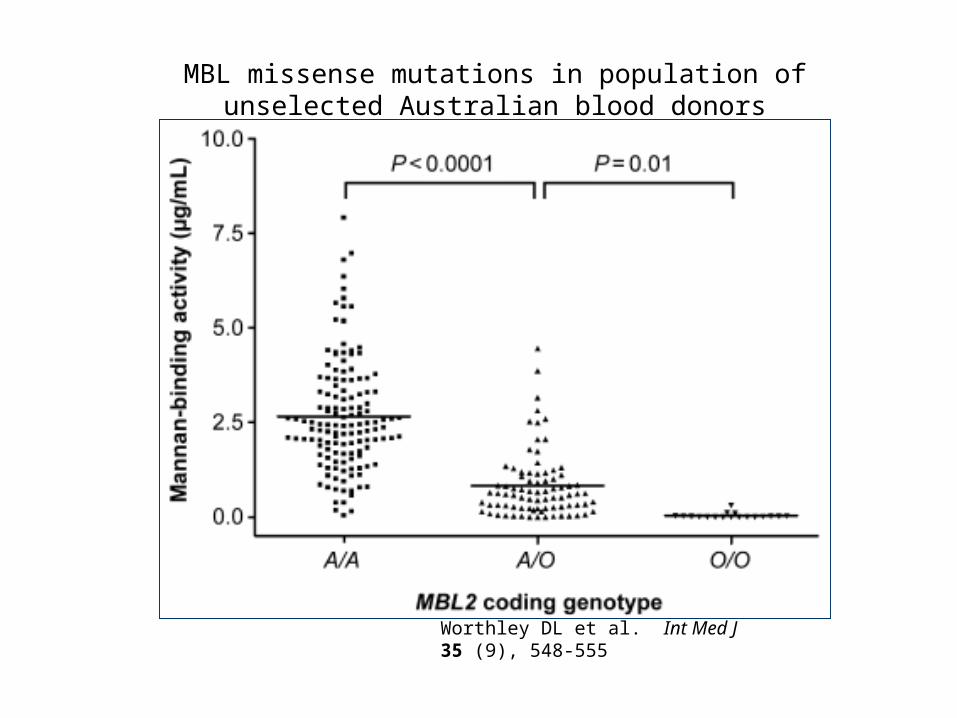
Worthley DL et al. Int Med J 35 (9), 548-555
MBL missense mutations in population of unselected Australian blood donors
Clinical manifestations
• Clinically silent in most otherwise healthy individuals
• Manifests in individuals with immature or compromised adaptive immune systems– Early infancy and childhood (range undefined)– Cystic fibrosis– Post chemotherapy– Post-stem cell transplant
• Associations with other conditions– Autoimmune disease– Other inflammatory disorders– Miscarriage
• Possibly beneficial in cases where increased opsonization and phagocytosis may promote intracellular pathogens such as mycobacteria

Summerfield JA et al. BMJ. 1997 Apr 26;314(7089):1229-32
Objective: To determine the extent to which mutations in the mannose binding protein gene predispose to childhood infection
Design: Clinical details and genotype of mannose binding protein determined in consecutive children attending a paediatric department
Subjects: 617 children presenting to London inner city hospital between October 1993 and August 1995
Results: – The prevalence of mutations in the mannose binding protein gene in
children with infection (146/345) was ~2x that in children without infection (64/272) (P<0.0001)
– Increased susceptibility to infection was found in both heterozygotic and homozygotic children
– 13 out of 17 children homozygotic for variant alleles presented with strikingly severe infections, including 6 with septicaemia

Infections in 133 children heterozygotic for mutations in mannose binding protein gene
Diagnosis NOsteomyelitis 3
Otitis media 4
Streptococcal infection 4
UTI 4
Gastroenteritis 5
Cellulitis and abscess 8
HIV 8
FUO 14
Tonsillitis 14
Meningococcemia 17
Chest infection 23
Miscellaneous 29

Sex Age Clinical detail
M 8yo Recurrent cellulitis and boils, surgical drainage; father and maternal uncle had boils
M 6yo 54M74Recurrent, serious chest infections, persistent cough, low IgG3
F 8yo 54F94Tetralogy of Fallot, cleft palate and lip, congenital ptosis
F 11mos Transfusion associated HIV infection, pneumocystis, herpes zoster, recurrent chest infections
M 6yo Meningococcal sepsis
F 26mos Meningococcal sepsis
M 5yo Severe meningococcal sepsis
M 27mos Severe meningococcal sepsis, skin grafting, avascular necrosis of hip
M 0 Prematurity (25wks)
M 0 Prematurity, respiratory distress
F 4yo H. Influenzae septicemia, recurrent tonsillitis
M 15mos Sickle trait, pneumococcal sepsis
M 12mos Streptococcal infection, otitis media, hx prematurity
F 28mos Recurrent tonsillitis, bilateral chronic otitis media
M 6yo Recurrent tonsillitis, bilateral otitis media
F 12yo Recurrent tonsillitis
Clinical details of children homozygotic for mutations in MBL gene

Prevalence of mutations was significantly greater in infected children under 6 months (P=0.05), between 6 and 18 months (P=0.03), and over 18 months (P=0.0001)

Koch A et al. JAMA 2001; 285: 1316–1321
• Objective To investigate the effect of MBL insufficiency on risk for acute respiratory tract infection (ARI) in unselected children younger than 2 years
• Design and Setting Population-based, prospective, cohort study conducted in Sisimiut, Greenland
• Subjects 250 children (age <2yrs) followed weekly between August 1996 and August 1998 for morbidity surveillance
• Results – A 2.08-fold (95% CI, 1.41-3.06) increased relative risk (RR) in MBL-
insufficient children (n = 13) compared with normals (n = 239; P<.001) – Risk is stratified by age
• Age 6 to 17 months (RR, 2.92; 95% CI, 1.78-4.79)• 0 to 5 months (RR, 1.47; 95% CI, 0.45-4.82) and • No effect in 18 to 23 months (RR, 1.00; 95% CI, 0.42-2.37)

Association between MBL genotypes and risk of acute respiratory tract infections (ARI) in 252 children from Sisimiut, Greenland

Interaction between age and MBL genotypes and risk of ARIs in 252 children from Sisimiut, Greenland
Dahl M et al. J Exp Med 2004; 199: 1391–9
• Objective: Investigate associations between MBL-deficiency and infection, other common diseases, and death in an unselected adult population
• Study design: longitudinal cohort study (part of Copenhagen City Heart Study), evaluated at baseline and at 8 and 24-year-followup by questionnaire, interview, and chart review
• Subjects: 9245 adults age>20
• Results:– No differences in infection or hospitalization rates between
heterozygote/homozygote subjects and normals– Increased risk associated with homozygosity in cardiac-related
hospitalization – Not confirmed by 2 subsequent case-control studies

Morbidity leading to hospitalization according to MBL deficiency genotype during 24 yr follow-up

Mortality according to MBL deficiency genotype during 8 yr follow-up

Treatment options
• Human and recombinant MBL therapy under development
• Anecdotal reports of successful replacement therapy
• Phase I trial (Valdimarsson H et al. Scand J Immunol 2004; 59: 97–102) – 20 healthy, adult MBL-deficient subjects– 6mg human MBL IV administered weekly x 3wks– Infusions well tolerated– Serum half-life 70h; twice to thrice weekly infusions may be
needed to maintain stable, protective levels– No antibodies to MBL detected up to 24 weeks after treatment
• Phase II trials underway

In a 6-year-old boy with intact humoral immune responses, is mannan-binding lectin (MBL) deficiency an explanation for recurrent sinusitis and otitis media?
Yes and No– May be explanation for early infections, setting up
chronic inflammation and hypertrophy of mucosal tissues
– Follow-up post-vaccination antibody titers– ENT evaluation
• Saline washes for sinuses• Tonsillectomy/adenoidectomy scheduled• Endotracheal aspirate for gram stain and culture

Steve and Les holding their prize giant herring
Sometimes it’s good to catch a herring!
Top Related