




Languages
Pages
Legal


8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 1/150
Rational Use ofAntibiotics
Dr Ruzilawati Abu BakarJabatan Farmakologi
ext 6128
4th Year Medical Posting
2011/2012

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 2/150
Outline of the lecture
1)Indications for antibacterial therapy – definitive, empiric & prophylaxis
2) Selection of antibacterial agents
3) Methods of administration of antibacterialagents
4) Antibiotics Resistance5) Classification of antibacterial agents

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 3/150
Indications for antibacterial therapy:
1. Definitive therapy•This is for proven bacterial infections
•Attempts should be made to confirm the bacterialinfection by means of staining ofsecretions/fluids/exudates, culture & sensitivity,serological tests & other tests
•Based on the reports, a narrow spectrum, least toxic,easy to administer & cheap drug should be prescribed.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 4/150
2. Empirical therapy
• Empirical antibacterial therapy should be restrictedto critical cases, when time is inadequate foridentification & isolation of the bacteria & reasonablystrong doubt of bacterial infection exists:
- septicemic shock/sepsis syndrome- immunocompromised patients with severe systemic infection
- hectic temperature
- neutropenic patient (reduction in neutrophils)
In such situations, drugs that cover the most probable infective agent/s should be used.
Empiric antibiotic is antibiotic therapy that is begunbefore a specific pathogen is identified

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 5/150
3. Prophylactic therapy
• Certain clinical situations require the use of antibiotics
for the prevention rather than the treatment ofinfections.
• In all these situations, only narrow spectrum & specificdrugs are used
• The duration of prophylaxis is dictated by theduration of the risk of infection.
• eg.
1. Prevention for persons from non-malarious areas whovisit areas endemic for malaria.
2. Treatment prior to certain surgical procedures toprevent infections

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 6/150
Bacteria vs Host
Bacteria Host
Pathogen Vs non pathogen
Virulence
Host defence
antibiotic
Disease

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 7/150
Selection of
antibacterial agents

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 8/150
Factors should be considered beforeprescribing antibacterial agent
1. Site of infection
2.Type of infection
3.Severity of infection
4.Isolate & its sensitivity
5.Source of infection6.Patient factors
7.Drug-related factors

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 9/150
Koda-Kimble M.A.et al, AppliedTherapeutics , TheClinical Use ofDrugs (LippincottWilliams & Wilkin,9th ed.), 2009
1. Site of infection

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 10/150
1. Site of infectionInfection above the diaphragm:
•URTI eg pharyngitis, tonsilitis, sinusitis, otitis,epiglottitis etc.
- commonly caused by organism like Strep. pyogenes ,S. pneumoniae , Fusobacteria , Peptostreptococci (rarely Mycoplasma , H. influenzae )
- Can be treated with drugs like penicillinsmacrolides
cephalosporins

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 11/150
1. Site of infection…con’t
Lower respiratory tract infections:
Eg. Bronchitis, pneumonitis, pneumonia, lung abscessetc
-generally caused by the organisms Strep. pyogenes,S. pneumoniae , Fusobacteria , Peptostreptococci,Staph aureus (rarely Mycoplasma , H. influenzae ,Moraxella, Klebsiella) etc.
- can be treated penicillins, cephalosporins,macrolides & tetracylines

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 12/150
1. Site of infection …. con’t
Infection below the diaphragm:
•Eg UTI, intra-abdominal sepsis, pelvic infections etc ---these are caused by the organisms like E. coli, Klebsiella,Proteus, Pseudomonas, Bacteroides etc.
• Quinolones, aminoglycosides, 3rd generationcephalosporins & metronidazole alone or in combination are useful in these infections.
Rule of the thumbInfections above the diaphragm Cocci & Gram +ve organisms
Infections below the diaphragm Bacilli & Gram -ve organisms

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 13/150
1. Site of infection …. con’t
• There are certain sites where the infection tends to be difficult fortreatment :
- meningitis (impenetrable BBB),
- chronic prostatitis (non-fenestrated capillaris),
- intra-ocular infections (non-fenestrated capillaries),
- abscesses (thick wall, acidic pH, hydrolizing enzymes etc.),- cardiac & intravascular vegetations (poor reach & penetration),
- osteomyelitis (avascular sequestrum) etc
In such cases:-Higher & more frequent doseLonger duration of therapyCombinationsLipophilic drugs
may have to be used

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 14/150
2. Type of infection
Infections can be localised/extensive; mild/severe;
superficial/deep-seated; acute/sub acute/chronic &extracellular/intracellular.
For extensive, severe, deep-seated, chronic &intracellular infections –
• Higher & more frequent dose
• Longer duration of therapy
• Combinations
• Lipophilic drugs
may have to be used

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 15/150
3. Severity of infections• Bacteremia / sepsis syndrome / septic shock;
• abscess in lung / brain/ liver/ pelvis/ intra-abdominal;
• meningitis/ endocarditis/ pneumonias / pyelonephritis / puerperalsepsis;
• Severe soft tissue infections / gangrene & hospital acquired infections
For severe infectionsonly IV route- to ensure adequate blood levels.
only bactericidal drugs- to ensure faster clearance of the infection.
dose should be higher & more frequent.- If the site is unknown, attempt should be made to cover all possibleorganisms, including drug resistant Staphylococcus, Pseudomonas, &anaerobes.
- A combinations of Penicillins / 3rd generation cephalosporins,aminoglycosides & metronidazole may be used.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 16/150
4. Isolate & sensitivity
• Ideal management of any significant bacterial
infection requires culture & sensitivity (C&S) study ofthe specimen.
• If the situation permits, antibacterials can bestarted only after the sensitivity report is available.
• Narrow spectrum, least toxic, easy to administer &
cheapest of the effective drugs should be chosen.
If the patient is responding to the drug that hasalready been started, it should not be changed even if
the in vitro report says otherwise

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 17/150
5. Source of infection
Community-acquired infections areless likely to be resistant
whereas
Hospital-acquired infections arelikely to be resistant & more difficultto treat (eg. Pseudomonas, MRSAetc)

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 18/150

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 19/150
• In the elderly, achlorhydria may affect absorption ofanticbacterial agents; drug elimination is slower, requiringdose adjustments & ototoxicity of aminoglycosides may be
increased.
Patient factors…….con’t
Children
Elderly
- Tetracycline are contraindicated < 8 years because they discolour the teeth- < 18 years ALL fluoroquinolones arecontraindicated because they cause
arthropathy by damaging the growingcartilage.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 20/150
• In patients with likelihood ofcompromised immune status, likeextremes of age, HIV infection,diabetes mellitus, neutropenia,splenectomy, using corticosteroidsor immunosuppresants, patients
with cancers/blood dyscrasias,ONLY bactericidal drugs should beused.
Patient factors…….con’t
Patients with compromised immune status

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 21/150
Patient factors…….in pregnancyContraindicated in all trimesters Contraindicated in the last trimesters
Safe in pregnancy Contraindicated in lactatingmothers
• tetracylines
• quinolones
• streptomycin
• clarithromycin
• sulpha drug• nitrofurantoin
• chloramphenicol
•penicillins
•cephalosporins
•erythromycin
•isoniazid
•ethambutol
• sulpha drug
• tetracylines
•nitrofurantoin
• quinolones
•metronidazole
Drugs with limited data on safety like aminoglycoside, azithromycin,clindamycin, vancomycin, metronidazole, trimethoprim, rifampicin &pyrazinamide should be used with caution when benefits overweigh the risks

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 22/150
Patient factors…….in patientswith renal failure
Absolutely contraindicatedRelatively contraindicated
Relatively safe
It is better to avoid combinationsof cephalosporins & aminoglycosides in these patients because bothclasses can cause nephrotoxicity
• tetracycline
•Penicillins
•Macrolides
•Vancomycin
•Metronidazole
•Isoniazid
•Ethambutol
•Rifampicin
•Aminoglycoside
•Cephalosporins
•Fluoroquinolones
•Sulpha drug

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 23/150
Patient factors…….in patientswith hepatic failure
No drugs are absolutely contraindicated.
Relatively contraindicated Safe
•Chloramphenicol•Erythromycin estolate
•Fluoroquinolones
•Pyrazinamide
•Rifampicin
•Isoniazid
•Metronidazole
•Penicillins
•Cephalosporins
•Ethambutol
•Aminoglycosides

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 24/150
7. Drug factors
1. Hypersensitivity:If the patient has prior history of hypersensitivity theantibacterial agent should be avoided. It is thereforeimportant to elicit this history in all patients (common
with penicillin)
2. Adverse reactions:Certain ADRs warrant discontinuation of therapy & thedoctor should adequately educate the patients on theseadverse effects.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 25/150
7. Drug factors
3. Cost:
It should always be remembered that just because as
particular drug is expensive, it need not be superiorthan the cheaper ones.
Eg. Cheaper drug like doxycycline or co-trimoxazoleare as effective as the costlier clarithromycin or
cephalosporins in the management of lower RTI.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 26/150
7. Drug factors…….con’t
4. Interactions:Interactions with food & other concomitant drugs should beconsidered before instituting antibacterial therapy so as tomaximize efficacy & minimize toxicity.
a) Interactions include enhanced nephrotoxicity or ototoxicity
when aminoglycosides are given with loop diuretics, vancomycin orcisplatin.
b) Rifampicin, a strong inducer of hepatic drug-metabolizingenzymes, decreases the effects of digoxin, ketoconazole, oralcontraceptives, propranolol, quinidine & warfarin.
c) Erythromycin inhibits the hepatic metabolism of a number ofdrugs, including phenytoin, terfenadine, theophylline & warfarin.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 27/150
Methods of
administration ofantibacterial agents

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 28/150
Methods of administration of antimicrobials
Route of administration
The route of administration depends on the site, type &severity of the infection & the availability of a suitabledrug
- Oral route is the most preferred, easy & cheap,but may not be reliable in all circumstances, esp. inpatients with severe infections, non-compliant patients,in the presence of vomiting etc.
Certain drugs like the aminoglycosides & most 3rd generations cephalosporins are not available for oral
administration.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 29/150
Methods of administration of antimicrobials
- IM route should generally be restrictedfor the administration of procaine & benzathine
penicillin.
The absorption is not very reliable & it is
painful & dislike by the patients.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 30/150
Route of administration…….con’t
- IV route is the best for the management ofsevere & deep-seated infections since it ensures
adequate serum drug levels.
Procaine penicillin & benzathine penicillin should
never be given IV.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 31/150
Route of administration…….con’t
•However, some drugs are not availablefor parental use (eg. Most macrolides,sulpha drugs, tetracyclines)
• Antibacterials are also used topically

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 32/150
Dosage
- Dosage depends on patient’s age, weight, associatedconditions like pregnancy, renal & hepatic failure &site, type & severity of infection.
- Generally the dose should be higher in cases ofsevere, deep-seated infections & lower in cases ofrenal-failure.
- Unnecessary overdosage only adds to the cost &adverse effects.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 33/150
Frequency of administration
• The drug should be administered 4-5x the plasmahalf-life to maintain adequate therapeuticconcentrations in the serum throughout the day.
• Frequency can be:-
- increased in cases of severe, deep seated &sequestrated infections
- reduced in cases of renal & hepatic failure.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 34/150
Duration
• Duration of therapy depends on the site
1) Tonsilitis – 10 days
2) Bronchitis – 5-7 days
3) UTI – single shot to 21 days4) Lung abscess- 2-4 weeks
5) Tuberculosis – 6-24 months
• Longer courses of therapy are usually required for infections dueto fungi or mycobacteria
• Endocarditis & osteomyelitis require longer duration of treatment
om nat ons

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 35/150
om nat ons1) For synergistic effect:
eg: combination of 2 bacteriostatic drugs such as
trimethoprim + sulfamethoxazole =
Co-Trimoxazole (bacterim®)
Therapeutic advantage of sulphonamide+ trimethoprim
1) Synergistic effects
2) Bactericidal activity
3) Decrease resistance4) Bigger spectrum of activity
5) Reduced toxicity

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 36/150
2) Treatment of infections with multipleorganisms:
Mixed infections in lung abcess, peritonitis, soiled
wounds etc naturally require multiple antibioticsfor complete clearance of the infection – penicillins (for Gram +ve & certain anaerobes) &aminoglycosides (for Gram –ve); metronidazole for
bacteroides.
penicillins + aminoglycosides + metronidazole
Combinations…….con’t
’

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 37/150
3) To prevent resistance: Use of combination is a well known method ofpreventing drug resistance. The classic example is theantiTB therapy,
Eg isoniazid + ethambutol + rifampicin
4) To overcome resistance: Combination of specific drugs can be useful inovercoming that resistant infections, egPenicillins + -lactamase inhibitors
(Co-amoxiclav/augmentin)
Combinations…….con’t

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 38/150
The following combinations are irrational, not usefulor even harmful:
1) Bactericidal with bacteriostatic
eg. Penicillins (bactericidal) with tetracyclines ( bacteriostatic)
Bactericidal a/b (kill bacteria) – tend to be used in combinationwith one another
Bateriostatic a/b (prevent bacteria’s reproduction) – tend tobe used on its own
2) Combinations of drugs with similar toxicity
eg. Chloramphenicol & sulpha drug
3) Combining drugs for non-existing ―mixed infections‖
eg. Tablets of ciprofloxacin + metronidazole/tinidazole

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 39/150
Which one of the following patients is least likely torequire antimicrobial treatment tailored to theindividual’s condition?
A. Patient undergoing cancer chemotherapy
B. Patient with kidney disease
C.Elderly patient
D.Patient with hypertension
E. Patient with liver disease
A. Patient undergoing cancer chemotherapy

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 40/150
A. Patient undergoing cancer chemotherapy
- Anticancer drugs often suppress immune function 7 these patients require additional
antibiotics to eradicate infections
B. Patient with kidney disease
- Impaired renal function may lead to accumulation of toxic levels of antimicrobial drugs
C. Elderly patient
- Renal & hepatic function are often decreased among the elderly
D. Patient with hypertension- Elevated BP would not be expected to markedly influence the type of antimicrobial
treatment employed.
E. Patient with liver disease
- Impaired liver function may lead to the accumulation of toxic levels of antimicrobial drugs

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 41/150
Clinical failure of
antimicrobialtherapy

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 42/150
Failure of an antibiotic regimen (1)
1) Drug factors• incorrect choice,
• poor tissue penetration
• inadequate dose• pH – low pH reduces effectiveness of
aminoglycosides, erythromycin, clindamycin
Inadequate clinical or microbiological response toantimicrobial therapy can result from multiplecauses, including;
l ( )

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 43/150
Failure of an antibiotic regimen (2)
2) Host factors
• poor host defense,
• age
• renal & liver function• pre-existing dysfunction
of other organs
3) Pathogen factors
resistance
superinfection
A tibi ti R sist

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 44/150
Antibiotic Resistance
―P i illi E ‖

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 45/150
―Penicillin Era‖
1942-1950 available without a prescriptionPublic demand followed by production of throatsprays, cough lozenges, mouthwashes, soaps and otherproducts containing penicillin
Alexander Fleming Warned that excessive use could result in
antimicrobial resistance ―the microbes are educated to resist penicillin and
a host of penicillin-fast organisms is bred out
which can be passed to other individuals and from them to others until they reach someone who gets a pneumonia or septicemia which penicillin cannot save .‖ The New York Times 1945
Fleming’s words proved to be correct....
Th P bl f A tibi ti

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 46/150
The Problem of AntibioticResistance
Penicillin resistance first identified in 1940’s
Since then, antibiotic resistance hasdeveloped faster than new drugs
Estimated cost of infections: $4-5 million per year
Antibiotic resistance previously concentratedin hospitals, especially ICUs
MRSA recently estimated to kill 18,000Americans yearly

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 47/150
History
APPEARANCE
DRUG INTRODUCTION OF RESISTANCE
Penicillin 1943 1946
Streptomycin 1945 1959
Tetracycline 1948 1953
Erythromycin 1952 1988
Vancomycin 1956 1988
Methicillin 1960 1961
Ampicillin 1961 1973
Cephalosporins 1964 late 1960’s

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 48/150
Antibiotic Resistance
Relative or complete lack ofeffect of antimicrobial againsta previously susceptiblemicrobe
• Bacteria are said to beresistant to an antibiotic if themaximal level of that antibiotic
that can be tolerated by thehost does not stop theirgrowth.
What Factors Promote Antimicrobial

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 49/150
What causes the rapid occurrence of widespreadresistance?
(1) Incomplete treatment:
- people fail to finish the full course of their medication
- 25% of previously-treated tuberculosis patientsrelapsed with drug resistant strains; most had failed tocomplete their initial course
What Factors Promote AntimicrobialResistance?
What Factors Promote Antimicrobial

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 50/150
(2) Mis-prescription:
- patients demand antibioticsfor cold
- widespread inappropriate use:up to 50% of prescriptions indeveloping countries are for viral
infections that cannot respond
What Factors Promote AntimicrobialResistance?
(3) Exposure to microbes carrying
resistance genes
I i t A tibi ti U

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 51/150
Inappropriate Antibiotic Use
Prescription not taken correctly Antibiotics for viral infections Antibiotics sold without medical supervision Spread of resistant microbes in hospitals due
to lack of hygiene Lack of quality control in manufacture or outdated
antimicrobial Use of broad-spectrum agents when a narrow-
spectrum drug would suffice (eg, use of third-generation cephalosporins for community-
acquired pneumonia)
Mechanisms of Antibiotic

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 52/150
• The four main mechanisms by which microorganismsexhibit resistance to antibiotics are:
(1) Drug inactivation or modification:
e.g. enzymatic deactivation of Penicillin G in somepenicillin-resistant bacteria through the productionof β-lactamases.
(2) Alteration of target site: e.g. alteration of PBP—the binding target site ofpenicillins—in MRSA and other penicillin-resistantbacteria – resulting in decreased binding of the
antibiotic to its target.
Mechanisms of AntibioticResistance (1)
Mechanisms of Antibiotic

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 53/150
(3) Alteration of metabolic pathway: e.g. some sulfonamide-resistant bacteria do notrequire para-aminobenzoic acid (PABA), an importantprecursor for the synthesis of folic acid and nucleic
acids in bacteria inhibited by sulfonamides. Instead,they turn to utilizing preformed folic acid.
(4) Reduced drug accumulation: by decreasing drug permeability
and/or
increasing active efflux (pumping out) of the drugsacross the cell surface.
Mechanisms of AntibioticResistance (2)
R i t l t E

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 54/150
Resistance: -lactamase Enzymes
•Bacteria produce-lactamase enzymes to hydrolyze the
-lactamring before drugs can reach inner membrane where PG synthesis
occurs
•A cell may produce 100,000 - lactamase enzymes, each of whichcan destroy 1,000 penicillins per second 100 million molecules of
drug destroyed per second
• β-Lactamantibiotics act byinhibiting thesynthesis of thepeptidoglycan
layer of bacterialcell walls.

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 55/150
-lactamases
Enzymes produced by bacteria whichdestroy -lactam antibiotics
Many different types Penicillinases, cephalosporinases,
carbapenemases
Most are plasmid mediated
Overcoming lactam Resistance

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 56/150
Overcoming -lactam Resistance
slow to
hydrolyze
As a response to bacterial resistance to -lactam drugs, there aredrugs, such as Augmentin, which are designed to disable the -lactamase enzyme.
Augmentin is made of amoxicillin, a -lactam antibiotic, andclavulanic acid, a -lactamase inhibitor.
The clavulanic acid is designed to overwhelm all -lactamaseenzymes, bind irreversibly to them, and effectively serve as an
antagonist so that the amoxicillin is not affected by the -lactamase enzymes.
Overcoming lactam Resistance

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 57/150
Amoxicillin (-lactam antibiotic)
+ clavulanic acid (a -lactamase inhibitor)
= Co-amoxiclav (Augmentin®)
Ampicillin (-lactam antibiotic)+ sulbactam (a -lactamase inhibitor)
= Unasyn®
Overcoming -lactam Resistance
Resistance in Simpler Terms

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 58/150
Resistance in Simpler Terms…
BA
By-pass Alteredtarget
Efflux
Impermeability
Inactivation
(alteration of metabolic pathway)
(reduced drug accumulation)
(reduced drug accumulation)
Genetic alterations in drug

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 59/150
Genetic alterations in drugresistance
Acquired antibiotic resistance requires thetemporary or permanent gain or alterationof bacterial genetic information.
Resistance develops due to the ability ofDNA:-
1. To undergo spontaneous mutation
2. To move from one organism to another(DNA/gene transfer)
Spontaneous mutation of DNA

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 60/150
Spontaneous mutation of DNA
Stable and heritable genetic change
Not induced by antimicrobial agents
Resistance variant will proliferate
Eg. The emergence of rifampicin-resistant M.tuberculosiswhen rifampicin is used as a single antibiotic
DNA/Gene transfer of drug

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 61/150
DNA/Gene transfer of drugresistant
transduction
conjugation
transformation
DNA Most resistance genes are plasmid mediated
Plasmid may enter cells by processes such as conjugation,transduction (phage mediated) & transformation
Measuring Antimicrobial

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 62/150
Measuring AntimicrobialSensitivity
Disk Diffusion
E- test(antimicrobialgradient method)
Serial dilution
Measuring Antimicrobial

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 63/150
MIC increase in
the case ofresistance
(Minimal inhibitory concentration)
- important in diagnosticlaboratories to confirm resistanceof microorganisms to anantimicrobial agent
Measuring AntimicrobialSensitivity
Consequences of Antimicrobial

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 64/150
Consequences of AntimicrobialResistance
Infectionsresistant to
availableantibiotics
Increased costof treatment

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 65/150

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 66/150
Speed development of new antibiotics Track resistance data nationwide Restrict antimicrobial use
Narrow spectrum Combination in longterm use (TB) Direct observed dosing (TB) Appropriate dose and duration Use more narrow spectrum antibiotics Use antimicrobial cocktails
Prevention of resistance

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 67/150
• A pregnant woman was hospitalized andchatheterized with a catheter. She developed aurinary tract infection caused by Pseudomonasaeruginosa and was treated with gentamicin. Whichof the following adverse effects was arisk to the fetuswhen the woman was on gentamicin?
• A. Skeletal deformity• B. Hearing loss
• C. Teratogenesis
• D. Blindness
• E. Mental retardation

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 68/150
Classification of
antibacterial agents

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 69/150
Chemical structure
Mechanism of action
Spectrum of activity
Broad, extended, narrow
Types of actions i i i i
Classification of antibacterial agents
Chemical structure

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 70/150
Chemical structure
Sulfonamides sulfadiazines
Diaminopyrimidines Trimethoprim
Quinolones Nalidixic acid, ciprofloxacin
b-lactam antibiotics Penicillins, cephalosporins,
carbapenems, monobactams
Tetracyclines Tetracycline, doxycycline
Nitrobenzene derivatives Chloramphenicol
Aminoglycosides Gentamicin
Macrolides Erythromycin
Nitrofuran derivatives Nitrofurantoin
Glycopeptide
Vancomycin Nitroimidazoles
Metronidazoles
Spectrum of activity

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 71/150
Terms Definitions
Narrow-spectrumantibiotics
Antibiotics acting only on a single or alimited group of microorganisms
Eg.- isoniazid active only againstmycobacteria
Extended-spectrumantibioticsAntibiotics that are effective against gram+ve organisms & also against a significantno. of gram -ve organisms.
Eg.- ampicillin – acts against gram +veorganisms (Listeria monocytogenes) & somegram -ve organisms (E. coli ).
Broad-spectrumantibiotics
Antibiotics affect a wide variety ofmicrobial species
Eg.- tetracycline active against chlamydia,mycoplasma, actinomyces, anaerobicorganisms, gram –ve rods (E. coli )
Spectrum of activity

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 72/150
Spectrum of activity
Summary of antibiotic’s spectrum

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 73/150
y p
Narrow Spectrum
• Aztreonam
• Benzylpenicillin
• Cloxacillin• Phenoxymethyl-penicillin
• Cephalexin
Broad Spectrum•Amoxycillin
•Aminoglycoside
•Ciprofloxacin
•Chloramphenicol
•Imipenam
•Tetracycline
•Vancomycin
•Carbenicillin
•3rd generation cephalosporins
B d l b

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 74/150
Bactericidal vs. bacteriostatic
Bactericidalagents
outright kill
bacteria.
Bacteriostatic agentsinhibit growth but
don’t kill. They rely onbody defenses toclear the infection.
Penicillins
Cephalosporins Macrolides
Tetracyclines
M h f

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 75/150
Mechanism of action
Inhibit cell wall synthesis Penicillins, cephalosporins, vancomycin
Inhibit protein synthesis Macrolides, tetracyclines, CMC
Inhibit DNA gyrase Quinolones
Interfere with DNA function
Rifampicin, metronidazole Antimetabolites
Sulfonamides, Trimethoprim
Cell Wall Inhibitors

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 76/150
1. Beta-lactam antibiotics1) Penicillin derivatives
2)Cephalosporins
3)Monobactams
4)Carbapenems
1) Penicillin 2) Cephalosporins
-lactam ring in red
Cell Wall Inhibitors
2. Glycopeptides1) Vancomycin
3. Beta-lactamase inhibitors1) Clavulanic acid
2) Sulbactam
C ll ll i hibi

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 77/150
Cell wall inhibitors
1. -lactam antibiotics Penicillins
Cephalosporins
Carbapenems Monobactams
2. Glycopeptide Vancomycin
Teicoplanin
Penicillin core structure."R" is variable group.
B i l ll ll-lactam
antibiotics

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 78/150
Bacterial cell wall antibioticsinhibit
transpeptidasesenzymes that
form thesecrosslinkages
Glycopeptidesbind D-alanineand preventcrosslinkage
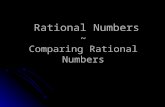
A schematic of peptidoglycan’s structure The NAM and NAG

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 79/150
A schematic of peptidoglycan s structure. The NAM and NAGsugars are shown as green and blue spheres respectively. Thetetrapeptides linked to NAM are cross-linked by a pentaglycinepeptide, shown as red lines linking the D-glutamine (L) to the D-alanine (A).
-lactamantibiotics
inhibittranspeptidasesenzymes thatform these
crosslinkages
Glycopeptidesbind D-alanineand preventcrosslinkage
Penicillins - structure

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 80/150
Penicillins - classifications

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 81/150
Penicillin G like drugs Penicillin G (Benzylpenicillin) Penicillin V Procaine penicillin G Benzathine penicillin G
Penicillinase- resistant penicillins (anti staph)
Cloxacillin Flucloxacillin Methicillin
Extended spectrum penicillin Ampicillin-like drugs
Ampicillin Amoxicillin Broad-spectrum (antipseudomonal) penicillins
Carbenicillin Piperacillin
P i illi h ki ti

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 82/150
Penicillins - pharmacokinetics
Given parenterally – well distributed
Crosses inflamed biological barrier
Mainly excreted via kidney Inhibited by probenecid
Penicillins - indication

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 83/150
Penicillins - indication Penicillin G
Gram +ve infectionStreptococciMeningococci Pneumococci Clostridium
Syphilis
Penicillinase-resistant penicillins Staph infection
ImpetigoAbcess
Extended spectrum penicillin Gram +ve & Gram –ve
Pneumonia, otitis media
P i illi d ti

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 84/150
Penicillins – adverse reaction
Relatively non-toxicAllergic reaction
Anaphylaxis- will occur in approximately in
0.01% patients
A rash on the back of aperson with anaphylaxis
C h l i

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 85/150
Cephalosporins
1. 1st generation cephalosporins

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 86/150
g p p
2. 2nd generation cephalosporins-best for Gram +ve & -ve-Extended Gram –ve coverage- eg. Cefuroxime, Cefaclor
- best for Gram +ve- eg. Cephalexin, Cephazoline
3. 3rd generation cephalosporins -best for Gram –ve-antipseudomonas- eg. Ceftazidime, Ceftriaxone, Cefotaxime,
Cefoperazone
4. 4th generation cephalosporins -Good coverage for both Gram +ve & -ve
- antipseudomonal activity
-Eg. Cefipime
C h l i d ti

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 87/150
Cephalosporins – adverse reactions
Fairly safeAllergic reaction
Cross reaction with penicillinSuperinfection
(an infection following a previous infection, esp. when caused bymicroorganisms that have become resistant to the antibiotics
used earlier)
Carbapenem

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 88/150
Carbapenem Examples
Imipenem
Meropenem
Wide spectrum
Resistant against -lactamase Good activity against both Gram +ve & -ve
Active against pseudomonas
Use in resistant organisms Hospital acquired infection
M n b t m

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 89/150
Monobactam
ExampleAztreonam
Resistant against -lactamase
Antipseudomonal activity Inactive against Gram +ve
GIT side effects – diarrhea, nausea &
vomiting IV – poorly absorbed when given via oral
route.
l t m s inhibit s

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 90/150
- lactamase inhibitors
Resemble -lactam molecules No antibacterial activity Inhibits bacterial -lactamase Use in combination with penicillins
Ampicillin–sulbactam Piperacillin-tazobactam
Amoxycillin-clavulanate (clavulanic acid)
Glycopeptides

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 91/150
Glycopeptides
Vancomycin, teicoplanin Active against Gm +ve esp staph
Not active against Gm –ve
Use in MRSA infection
Nephrotoxicity, red man syndrome
PROTEIN SYNTHESIS INHIBITOR

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 92/150
1) Aminoglycosides
2) Tetracyclines
3) Chloramphenicol
4) Macrolides5) Fusidic Acid

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 93/150
Aminoglycosides

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 94/150
Aminoglycosides
Bactericidal From various Streptomyces species
Streptomycin
Neomycin Amikacin
Gentamicin
Tobramycin Netilmicin
Aminoglycosides – physical

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 95/150
g y p yproperties
Water soluble (polar)Poorly absorbed from gut
Given parenterallyLess able to cross biological
barrier
More active at alkaline pH
Aminoglycosides MOA

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 96/150
Aminoglycosides - MOA
Irreversible inhibitor ofprotein synthesis
Passive diffusion via porinchannels of outer
membrane
Actively transport intocytoplasm
Bind to 30S subunitribosome
Interfere with synthesis
of protein
Aminoglycoside: clinical use

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 97/150
Use against Gram –ve infection Usually combined with -lactam
antibiotic Better coverage Synergistic effect
No activity against anaerobe
Aminoglycoside: clinical use
Aminoglycosides -

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 98/150
pharmacokinetic
Polar substance Given i.m. or i.v.
Poorly penetrate CSF or eye 20% blood level in inflamed meninges
May be given intrathecal
t1/2 = 2-3 hours
Excreted unchanged by the kidneys
Adjust dosage with renal impairment Can be calculated based on creatinine clearance
Aminoglycosides: PK PD

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 99/150
Aminoglycosides: PK-PD
Concentration dependent killing Rate of killing depend on concentration
Post antibiotic effect
Antibacterial activity persist after thelevel reduce to below MIC
Can be given single daily dose Same efficacy Reduce risk of toxicity convenience
Aminoglycosides: toxicity

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 100/150
g y y Ototoxic
Auditory damage Vestibular damage
Nephrotoxic Potentiated by other
nephrotoxic drugs
Need to measurelevel (TDM)
Peak and trough High dose
Block neuromuscular junction
Streptomycin

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 101/150
Mainly use in the treatment of TB Combine with other anti TB
Resistance easily developed withoutcombination
Side effect Fever, rashes Impair vestibular function
Contraindicated in pregnancy
Deafness in newborn
Gentamicin

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 102/150
Gentamicin
Active both in Gram +ve & -ve Staphylococci
Resistance rapidly developed
Pseudomonas, klebsiella No activity against streptococci and
enterococci
But can enhance the effect of -lactam orvancomycin
Gentamicin – clinical uses

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 103/150
Gentamicin – clinical uses
Combine with cell wall inhibitor in severeinfection
With penicillin G in Strep viridans
endocarditis Should not be used alone for pneumonia
Poor penetration
Requires TDM If use more than 5 days Renal impairment
Amikacin

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 104/150
Amikacin
Semi synthetic aminoglycoside More resistant than genta towards
inactivating enzymes
Active against MDR M. tuberculosis Usually use as second line antibiotic
Spectinomycin

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 105/150
Spectinomycin
Structure related to aminoglycoside butlack of amino sugars
Given i.m.
Only use as an alternative to penicillin ingonorrhoea therapy Penicillin sensitivity
Resistant gonococcal Rarely nephrotoxic

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 106/150
Macrolides

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 107/150
Macrolides
azithromycin erythromycin clarithromycin
Macrolides

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 108/150
Macrolides
MOA
Bind reversibly to
the 50S subunit Inhibit elongation
of the protein
• Streptomycin obtained from Streptomyces erythreus
• Clarithromycin & azithromycin are semisynthetic
Erythromycin- spectrum

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 109/150
Erythromycin spectrum
Gram +ve Pneumococci, streptococci, staph
Atypical organism
Mycoplasma, clamydia Mycobacteria
M. kansasii
Gram –ve Neiserria sp, B pertussis,
Corynebacteria
Treponema pallidum (syphilis)
Erythromycin - pharmacokinetics

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 110/150
Erythromycin pharmacokinetics
Destroyed by stomach acid Enteric coated tablet
Food interferes absorption
t1/2 = 1.5 hours Well distributed except CSF
Excreted in biles
Erythromycin- uses

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 111/150
Erythromycin uses
Corynebacterialinfection Diphteria
Clamydial infection Community acquired
pneumonia
Pertussis
Syphilis Penicillin allergy
Erythromycin- ADR

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 112/150
Erythromycin ADR
GIT Nausea, vomiting,diarrhoea
Liver toxicity Cholestatic jaundice
Drug interaction Inhibit cytochrome P450
Clarithromycin

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 113/150
Clarithromycin
Improved acid stability Better absorption
Longer t1/2 BD dosing
Metabolised by liver
More active against Mycobacterium avian complex
More expensive
Azithromycin

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 114/150
Azithromycin
More active against M avian complex
Toxoplasma gondii
Penetrates well into tissues Concentration > 10 – 100 times serum
Tissue t1/2 = 2-4 days Single daily dose Short courses

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 115/150
Tetracyclines

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 116/150
Tetracyclines
Tetracyclines - MOA

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 117/150
Tetracyclines MOA
Bind reversibly tothe 30S subunit
Misalignment of
anticodons of thecharged tRNAs withthe codons of themRNA.
Failure of proteinsynthesis
Tetracyclines

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 118/150
Tetracyclines
Introduced in 1948 (chlortetracycline) Bacteriostatic
Coverage
Gram +ve & -ve Atypical bacteria
Rickettsiae
Chlamydia
mycoplasma Protozoa
Amoebas
Tetracyclines – P’kinetics

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 119/150
GI absorption
tetracycline (60-80%), doxycycline (95%), minocycline (100%)
Impaired by food (esp with Mg2+,Ca2+)
Ditributed widely except intoCSF
Crosses placenta Excreted both thru bile and
urine T 1/2
Short acting (6 hrs) Tetracycline
Intermediate (12 hrs) demeclocycline
Long (18 hrs)
doxycycline, minocycline
Tetracyclines - uses

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 120/150
Tetracyclines uses
Drug of choice in atypical bacteria infection Ricketsiae
Used in combination to treat gastric or
duodenal ulcer To eradicate H. Pylori
Cholera
Acne
Lyme disease (Borelia burgdorferi )
Tetracyclines - ADR

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 121/150
Tetracyclines ADR
GIT Nausea, vomiting,
diarrhoea
Damage growingbone & teeth Due to Ca2+ chelating
property
Yellow discolouration Contraindicated in
children < 8 years old
Hepatic injury Increased during
pregnancy
Nephrotoxicity
Photosensitization Severe sunburn ;
doxy/demeclocycline

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 122/150
Chloramphenicol

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 123/150
Chloramphenicol
Binds to 50 S ribosomalsubunit
Mainly bacteriostatic
Bactericidal H. influenza
N. meningitidis
Broad spectrum (includingrickettsiae)
Chloramphenicol – P’kinetics

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 124/150
hloramphen col k net cs
IV (prodrug) or orally Complete oral absorption
Excretion depends on conversion in liver
to glucuronide, then secretion in kidney Slow excretion in liver impairment
Chloramphenicol - uses

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 125/150
r mp n u
Staph brain abscess Typhus
As an alternative in meningitis
Conjunctivitis – eye preparation
Chloramphenicol - ADR

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 126/150
mp D
Blood dyscrasias Idiosyncratic aplastic anemia
Gray baby syndrome Neonates if doses not adjusted
ANTIMETABOLITES

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 127/150
1) Trimethoprim
2) Sulfonamides
Sulphonamide - MOA

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 128/150
p
Bacteria cannottransport folate intocells
Tetrahydrofolate is aDNA precursor
p-aminobenzoic acid(PABA) is a precursorfor folate synthesis
Sulfonamides arestructurally similar to
PABA Inhibits synthesis ofdihydropteroatesythase (DHPS)
DHPS & DHFR absent inmammalian cells
Sulfonamides - effect

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 129/150
Bacteriostatic Active against
Both Gram +ve & -ve
E. coli, Klebsiella, Salmonella Clamydia
Some protozoa –
Pneumocystis carinii Not active against rickettsiae
Sulfonamides -Pharmacokinetics

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 130/150
Pharmacokinetics
Preparation available Topical
Oral
Well absorbed from gut Distributed widely including CSF
Metabolized in liver
Excreted via kidney
Sulfonamides - uses

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 131/150
Topical Sulfacetamide ophthalmic solution
Conjunctivitis
Trachoma Silver sulfadiazine (SSD)
burns
Systemic Use in combination
Sulfonamides - ADR

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 132/150
Fever Skin rash
Exfoliative
dermatitis Steven Johnson
syndrome
Crystalluria
Sulfonamides - combination

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 133/150
Sulfadiazine + pyrimethamine Pyrimethamine inhibit protozoan
DHFR Synergistic
Penetrates CSF 1st line for acute toxoplasmosis
Sulfadoxin + pyrimethamine (Fansidar)
Long acting Prophylaxis & treatment for
malaria

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 134/150
Trimethoprim + sulfamethoxazole(TMP + SFX = co-trimoxazole)

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 135/150
(TMP + SFX = co-trimoxazole)
TMP Inhibit DHFR
Synergistic whencombined with SFX
Combination isbactericidal
co-trimoxazole – p’kinetics

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 136/150
p
TMP:SFX = 1:5 Available in IV and oral
Oral Well absorbed T1/2 = 10 hrs (both)
Penetrates well into CSF, prostate
Excreted in urine Usually given BD dose
co-trimoxazole - uses

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 137/150
Infection caused by Shigella Salmonela
UTI Treatment prophylaxis
Community acquired pneumonia PCP pneumonia (P. jiroveci )
Treatment prophylaxis
Co-trimoxazole - ADR

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 138/150
Sulfonamides ADR Megaloblastic anaemia
Leukopenia
Granulocytopenia
Inhibit DNA gyrase

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 139/150
Quinolones
Essential structure of all quinoloneantibiotics
Metronidazole
- Fluoroquinolones
Interfere with DNA function
Fluoroquinolones

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 140/150
q
Synthetic fluorinated analogs ofnalidixic acid
Inhibit bacterial DNA synthesis
Inhibit DNA gyrase & topoisomerase Examples
Ciprofloxacin
Norfloxacin Perfloxacin

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 141/150
Required fornormal
transcriptionand
replication
Inhibition of topoisomerase IV
prevents separationof replicated DNA
Fluoroquinolones

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 142/150
Spectrum depend on drugs Earlier fluoroquinolones (ciprofloxacin)
Mainly cover Gram –ve
Later drug (gatifloxacin) Better coverage for Gram +ve
Also useful in
Atypical pneumonia TB, M. avian
Fluoroquinolones - uses

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 143/150
Usually used in multidrug resistantinfection
UTI
Bacterial AGE Gonorrhea
Eradication of meningococci from
carriers
Fluoroquinolones - ADR

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 144/150
Usually well tolerated GIT upset
Allergic reaction
May damage growing cartilage (rat)

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 145/150
Metronidazole - anaerobes- It is used mainly in the treatment of infections caused

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 146/150
yby susceptible organisms, particularly anaerobic bacteria
and protozoa.
- It is used to treat ameobic dysentry, giardiasis,gangrene, pseudomonas coitis & various abdominalinfections, lung abscess & dental sepsis.
Mechanism of actions- The nitro group of metronidazole is able to serve as anelectron acceptor, forming reduced cytotoxic compoundsthat bind to proteins and DNA, resulting in cell death.
Metronidazole - anaerobes

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 147/150
Side Effects
PK
It is well absorbed after oral or rectaladministration
•Nausea & vomiting
•Peripheral neuropathy
•Convulsions, headaches•Hepatitis
Pathogen Drug (s) of first choice Alternative Drug (s)
Gram +ve cocciPneumococcus Penicillin G, Ampicillin Erythromycin, Cephalosporin

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 148/150
Streptococcus (common) Penicillin G Erythromycin, Cephalosporin
Staphylococcus
(penicillase-producing)
Augmentin ® , Unasyn ® , Cloxacillin,Methicillin, Nafcillin, Timentin ®
Cephalosporin
Staphylococcus
(methicillin resistance)
Vancomycin TMZ-SMZ
Enterococcus Penicillin G plus gentamicin Vancomycin plus gentamicin
Gram -ve cocciGonococcus Cetrriaxone Penicillin G, Ampicillin, Spectinomycin
Meningococcus Penicillin G, Ampicillin Cefotaxime, Cefuroxime,Chloramphenicol
Gram -ve rodsE.coli , Proteus, Klebsiella Aminoglycosides, 3rd generation
cephalosporinTMZ-SMZ, Fluoroquinolone,extended spectrum penicillin
Shigella Fluoroquinolone TMZ-SMZ, Ampicillin
Enterobacter, Citrobacter,
Serratia
Imipenam, Fluoroquinolone TMZ-SMZ, extended spectrum
penicillin
Hemophilus spp Cefuroxime or 3rd generationcephalosporin
TMZ-SMZ, Ampicillin,
Chloramphenicol
Pseudomonas aeruginosa Aminoglycosides plus extendedspectrum penicillin
Ceftazidime, Aztreonam, Imipenam
Bacteroides fragillis Metronidazole, Clindamycin Imipenam, Chloramphenicol,Ampicillin/sulbactam
A patient with degenerative joint disease is toundergo insertion of a hip prosthesis. To avoidcomplication due to postoperative infection the

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 149/150
complication due to postoperative infection, thesurgeon will pretreat this patient with anantibiotic. This hospital has a significant problemwith MRSA. Which of the following antibioticsshould the surgeon select?
• A. Ampicillin
• B. Imipenem/cilastatin
• C. Gentamicin/piperacillin
• D. Vancomycin• E. Cefazolin

8/2/2019 Rational Use AB - 2011
http://slidepdf.com/reader/full/rational-use-ab-2011 150/150
THANK YOU
Top Related