






Languages
Pages
Legal

Radial Tunnel Nerve Block is useful in the diagnosis of Radial Tunnel Syndrome C Egeler, GL Roberts, M Pritchard,
ABMU HB Swansea
Introduction: Radial Tunnel Syndrome (RTS) is a rare cause of forearm pain, difficult to diagnose clinically with no reliable diagnostic test available. Previously blind trigger point injections have been used to improve surgical outcome. We present a series of patients who underwent US guided radial tunnel nerve block to successfully diagnose radial tunnel syndrome.
Methods: Over 3 years 12 patients with suspected of RTS underwent diagnostic US guided block of the deep radial nerve (DRN) at the Supinator Muscle (SM) with 1 ml 0.5 % Levobupivacaine. Patients who had temporary improvement were offered surgery. Surgical outcome was audited.
Results All patients had correct placement of LA demonstrated by temporary extensor weakness and wrist drop . 1 patient did not improve and did not proceed to surgery. 2 Patients achieved sustained improvement of symptoms and did not require surgery. 9 patients had temporary complete resolution of symptoms and were offered surgery. Of those patients 8 had an immediate successful outcome, 1 patient developed CRPS which settled over 12 months.
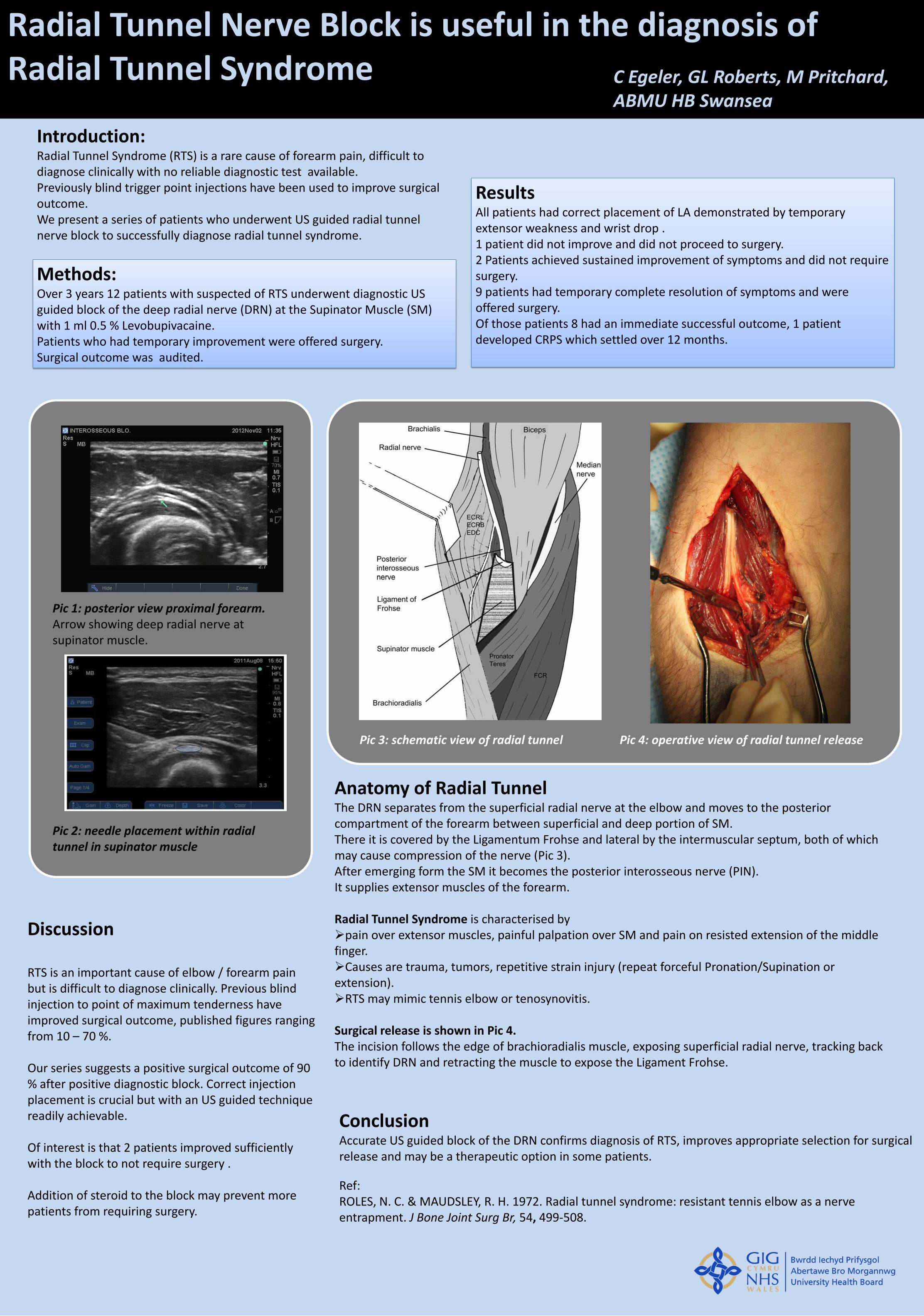
Anatomy of Radial Tunnel The DRN separates from the superficial radial nerve at the elbow and moves to the posterior compartment of the forearm between superficial and deep portion of SM. There it is covered by the Ligamentum Frohse and lateral by the intermuscular septum, both of which may cause compression of the nerve (Pic 3). After emerging form the SM it becomes the posterior interosseous nerve (PIN). It supplies extensor muscles of the forearm. Radial Tunnel Syndrome is characterised by pain over extensor muscles, painful palpation over SM and pain on resisted extension of the middle finger. Causes are trauma, tumors, repetitive strain injury (repeat forceful Pronation/Supination or extension). RTS may mimic tennis elbow or tenosynovitis.
Surgical release is shown in Pic 4. The incision follows the edge of brachioradialis muscle, exposing superficial radial nerve, tracking back to identify DRN and retracting the muscle to expose the Ligament Frohse.
Discussion RTS is an important cause of elbow / forearm pain but is difficult to diagnose clinically. Previous blind injection to point of maximum tenderness have improved surgical outcome, published figures ranging from 10 – 70 %. Our series suggests a positive surgical outcome of 90 % after positive diagnostic block. Correct injection placement is crucial but with an US guided technique readily achievable. Of interest is that 2 patients improved sufficiently with the block to not require surgery . Addition of steroid to the block may prevent more patients from requiring surgery.
Conclusion Accurate US guided block of the DRN confirms diagnosis of RTS, improves appropriate selection for surgical release and may be a therapeutic option in some patients.
Ref: ROLES, N. C. & MAUDSLEY, R. H. 1972. Radial tunnel syndrome: resistant tennis elbow as a nerve entrapment. J Bone Joint Surg Br, 54, 499-508.
Pic 2: needle placement within radial tunnel in supinator muscle
Pic 1: posterior view proximal forearm. Arrow showing deep radial nerve at supinator muscle.
Pic 3: schematic view of radial tunnel Pic 4: operative view of radial tunnel release
Top Related