







Languages
Pages
Legal

management
Medulloblastoma
: Dr Puneet Kumar Bagri
SURGER
Y
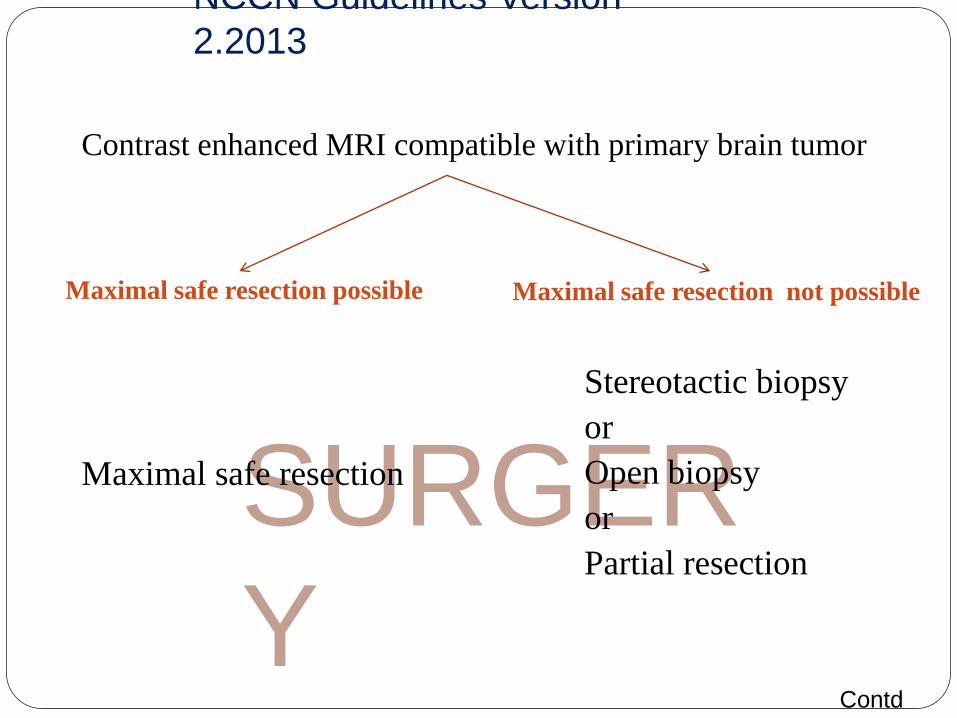
NCCN Guidelines Version
2.2013
Maximal safe resection possible Maximal safe resection not possible
Maximal safe resection
Stereotactic biopsy
or
Open biopsy
or
Partial resection
Contrast enhanced MRI compatible with primary brain tumor
Contd
…
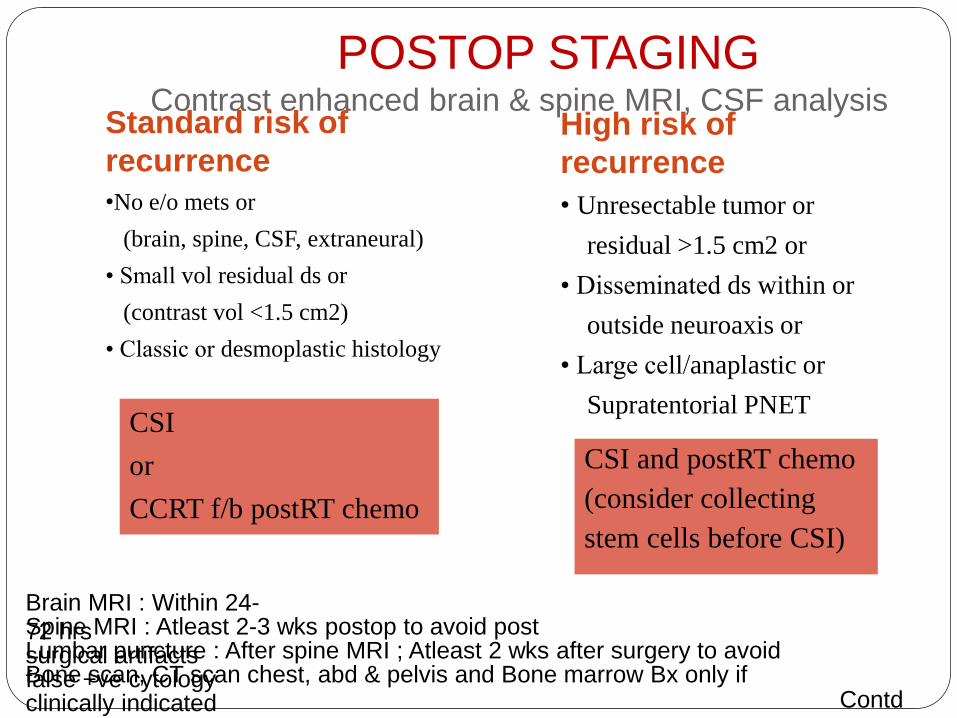
POSTOP STAGINGContrast enhanced brain & spine MRI, CSF analysis
Standard risk of
recurrence
•No e/o mets or
(brain, spine, CSF, extraneural)
• Small vol residual ds or
(contrast vol <1.5 cm2)
• Classic or desmoplastic histology
High risk of
recurrence
• Unresectable tumor or
residual >1.5 cm2 or
• Disseminated ds within or
outside neuroaxis or
• Large cell/anaplastic or
Supratentorial PNETCSI
or
CCRT f/b postRT chemo
CSI and postRT chemo
(consider collecting
stem cells before CSI)
Brain MRI : Within 24-
72 hrsSpine MRI : Atleast 2-3 wks postop to avoid post
surgical artifactsLumbar puncture : After spine MRI ; Atleast 2 wks after surgery to avoid
false +ve cytologyBone scan, CT scan chest, abd & pelvis and Bone marrow Bx only if
clinically indicated Contd
…
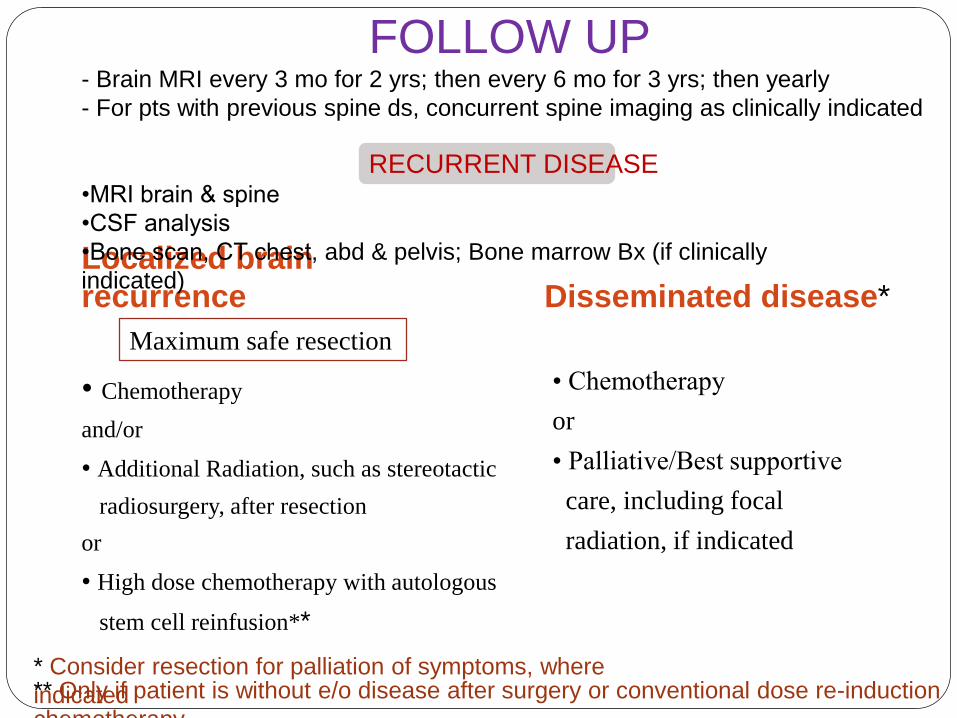
FOLLOW UP- Brain MRI every 3 mo for 2 yrs; then every 6 mo for 3 yrs; then yearly
- For pts with previous spine ds, concurrent spine imaging as clinically indicated
Localized brain
recurrence Disseminated disease*
• Chemotherapy
and/or
• Additional Radiation, such as stereotactic
radiosurgery, after resection
or
• High dose chemotherapy with autologous
stem cell reinfusion**
• Chemotherapy
or
• Palliative/Best supportive
care, including focal
radiation, if indicated
RECURRENT DISEASE•MRI brain & spine
•CSF analysis
•Bone scan, CT chest, abd & pelvis; Bone marrow Bx (if clinically
indicated)
Maximum safe resection
* Consider resection for palliation of symptoms, where
indicated** Only if patient is without e/o disease after surgery or conventional dose re-induction
chemotherapy
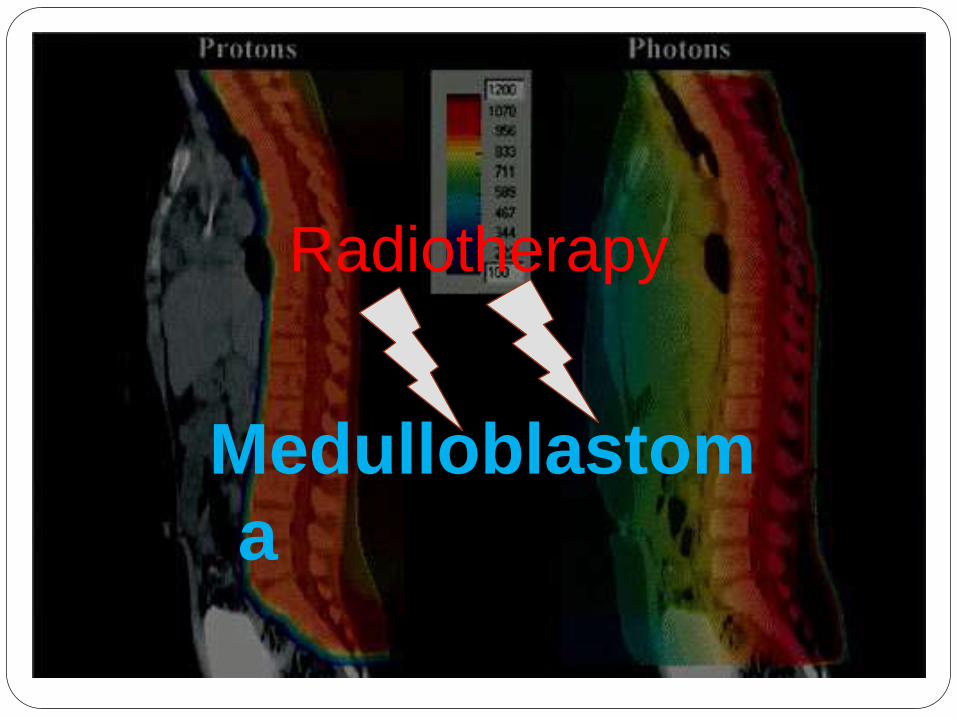
Radiotherapy
Medulloblastom
a
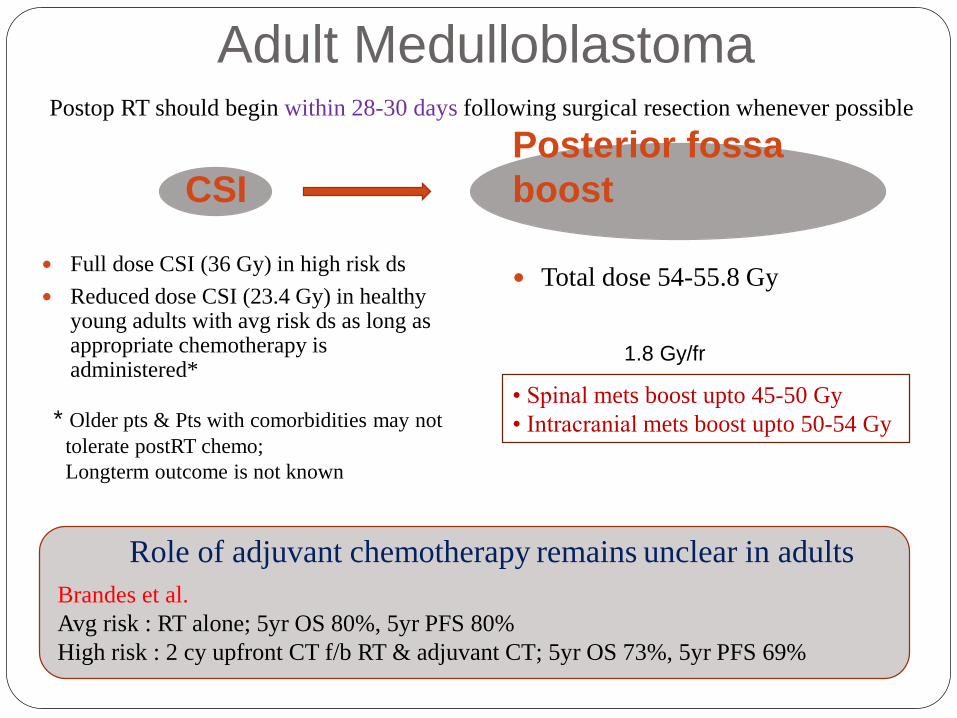
Adult Medulloblastoma
CSI
Posterior fossa
boost
Full dose CSI (36 Gy) in high risk ds
Reduced dose CSI (23.4 Gy) in healthy young adults with avg risk ds as long as appropriate chemotherapy is administered*
Total dose 54-55.8 Gy
Postop RT should begin within 28-30 days following surgical resection whenever possible
* Older pts & Pts with comorbidities may not
tolerate postRT chemo;
Longterm outcome is not known
• Spinal mets boost upto 45-50 Gy
• Intracranial mets boost upto 50-54 Gy
Role of adjuvant chemotherapy remains unclear in adults
Brandes et al.
Avg risk : RT alone; 5yr OS 80%, 5yr PFS 80%
High risk : 2 cy upfront CT f/b RT & adjuvant CT; 5yr OS 73%, 5yr PFS 69%
1.8 Gy/fr
Adult Medulloblastoma
Evidence-Based Treatment Summary
There are no prospective, randomized trials evaluating
major therapeutic issues in this disease in adults
Maximal surgical resection should be performed,
where feasible
Standard treatment consists of postop radiotherapy to
the craniospinal axis followed by a boost to the
posterior cranial fossa
The use of chemotherapy generally follows the
pediatric indications and guidelines
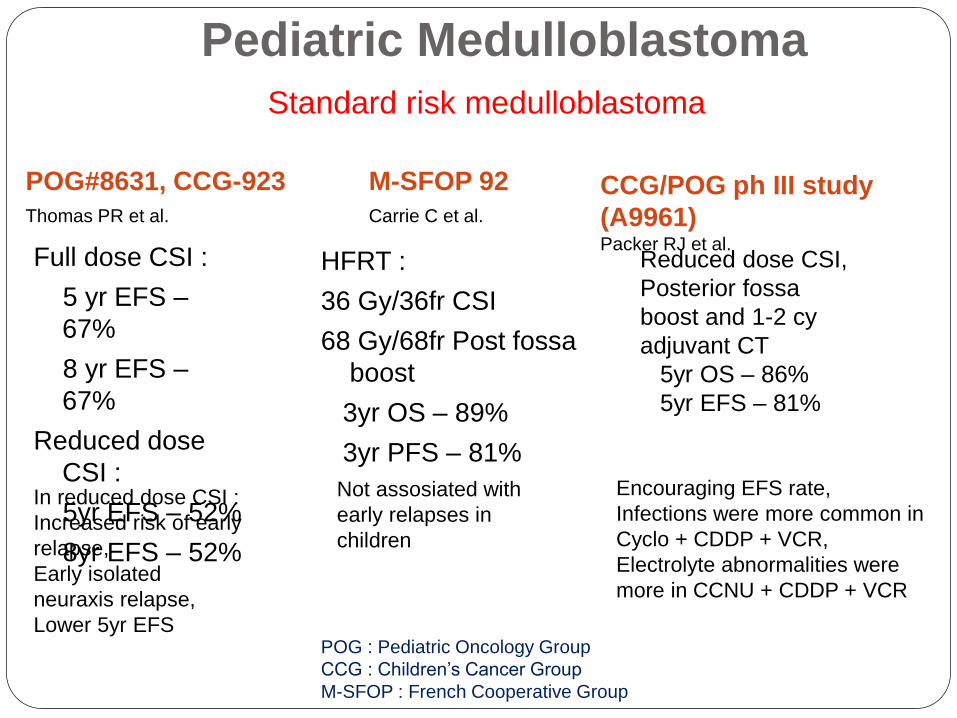
Pediatric Medulloblastoma
Standard risk medulloblastoma
POG#8631, CCG-923
Thomas PR et al.
M-SFOP 92
Carrie C et al.
Full dose CSI :
5 yr EFS –
67%
8 yr EFS –
67%
Reduced dose
CSI :
5yr EFS – 52%
8yr EFS – 52%
HFRT :
36 Gy/36fr CSI
68 Gy/68fr Post fossa
boost
3yr OS – 89%
3yr PFS – 81%
In reduced dose CSI :
Increased risk of early
relapse,
Early isolated
neuraxis relapse,
Lower 5yr EFS
Not assosiated with
early relapses in
children
CCG/POG ph III study
(A9961)Packer RJ et al.
Reduced dose CSI,
Posterior fossa
boost and 1-2 cy
adjuvant CT
5yr OS – 86%
5yr EFS – 81%
Encouraging EFS rate,
Infections were more common in
Cyclo + CDDP + VCR,
Electrolyte abnormalities were
more in CCNU + CDDP + VCR
POG : Pediatric Oncology Group
CCG : Children’s Cancer Group
M-SFOP : French Cooperative Group
Pediatric
Medulloblastoma
High risk medulloblastoma
CSI : 36 Gy
Posterior fossa boost upto 55.8 Gy
Additionally :
19.8 Gy to focal metastatic site
Spinal disease :
Additional boost upto total of 45 Gy if tumor is
located above the termination of spinal cord
Upto 50.4 Gy if tumor is located below the
termination of cord
Pediatric Medulloblastoma
Medulloblastoma in infants
Age <3yrs : The poorest risk group
Rate of complete resection is lower
Leptomeningeal seeding at diagnosis higher ( 50%)
Role of Radiotherapy is controversial
RT causes significant risks to neurocognitivefunctions
COG study : Chemotherapy alone
Without mets – 3yr PFS 29%
With mets – 3yr PFS 11%
POG study : Chemotherapy f/b delayed Radiation
2yr PFS 34%Contd…
Pediatric
Medulloblastoma
Medulloblastoma in infants
North American study :
» Tumor without leptomeningeal seeding RT
GTV : tumor bed
CTV : 1 cm margin to GTV
» With mets – Intensive Chemotherapy
Trials
High dose chemotherapy f/b autologous stem cell
rescue
showed good initial response; OS 30-40%
RADIOTHERAPY
Objective: To treat microscopic cancer cells / residual
tumor with the goal of reducing its size orstopping its progression.
Prevent or treat spread through CSF.
Covering the entire subarachnoid space is an
essential component in the management of
medulloblastoma. So We do Craniospinal
irradiation (CSI).
CSI is a very complex technique
Goal is to achieve uniform dosage throughout
the subarachnoid space, encompassing the
entire intracranial vault and spinal canal
Fundamental is
the use of opposed lateral fields including the
cranium and upper cervical spinal canal,
matching a posterior spinal field including the full
spinal subarachnoid space with cranial field
in larger children, the upper posterior spinal field
matching with a separate lower posterior spinal field
Target Volume:Entire brain and its meningeal coverings with the CSF
Spinal cord and the leptomeninges with CSF
Posterior fossa – boost
Energy4-6 MV linac or Co60
PortalsWhole Brain: Two parallel opposed lateral field.
Spine: Direct Posterior field
Scheduling of radiotherapy:Starting time : within 28 days following surgery
Duration of treatment : 45 to 47 days
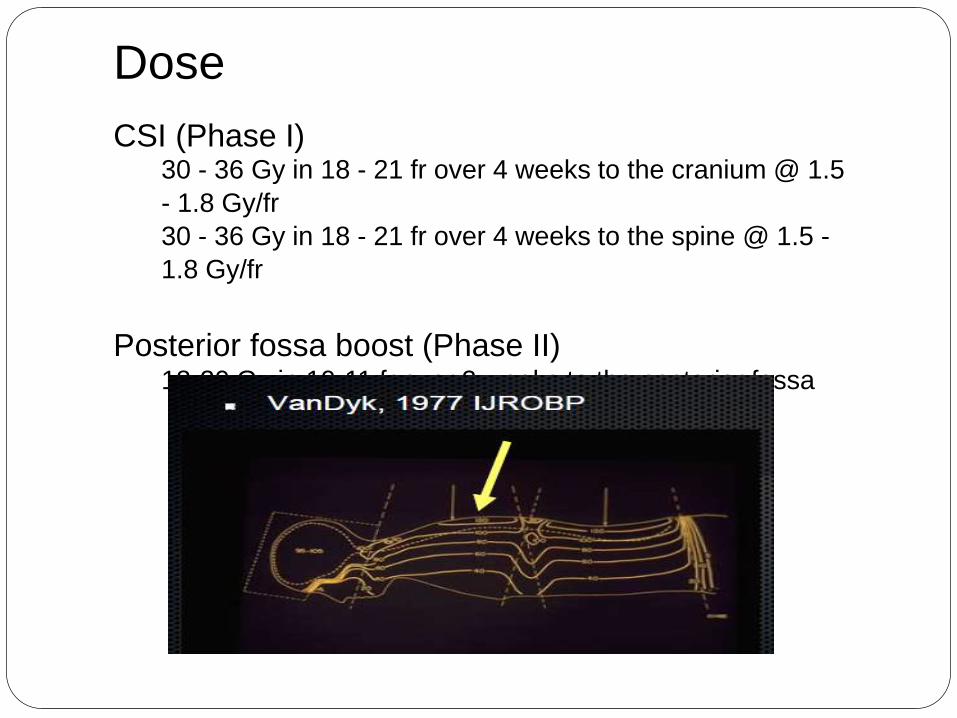
Dose
CSI (Phase I)30 - 36 Gy in 18 - 21 fr over 4 weeks to the cranium @ 1.5
- 1.8 Gy/fr
30 - 36 Gy in 18 - 21 fr over 4 weeks to the spine @ 1.5 -
1.8 Gy/fr
Posterior fossa boost (Phase II)18-20 Gy in 10-11 fr over 2 weeks to the posterior fossa
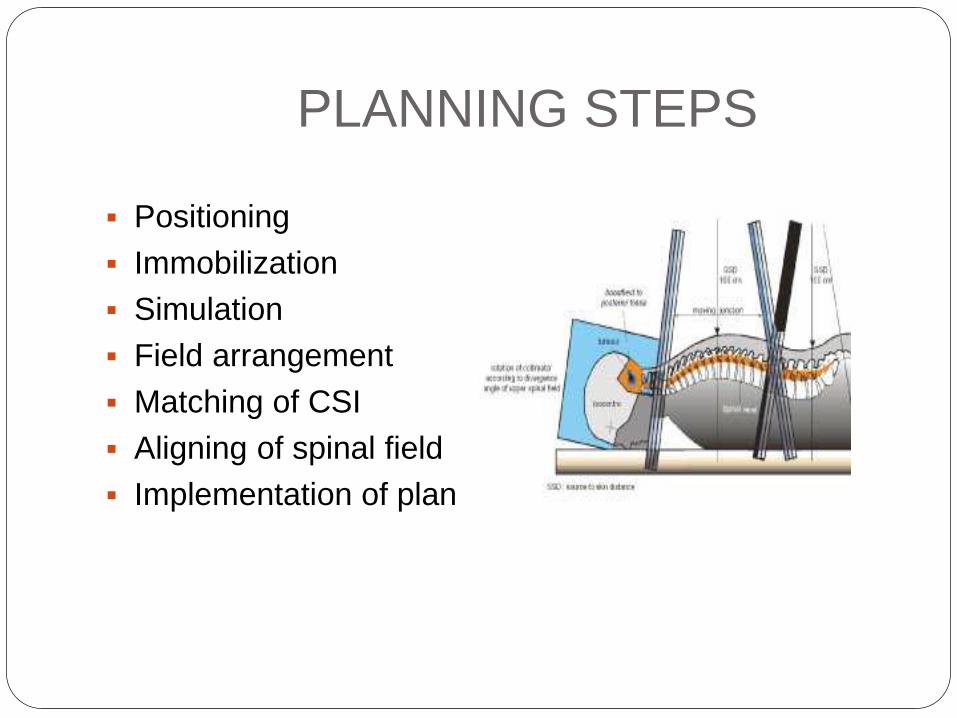
PLANNING STEPS
Positioning
Immobilization
Simulation
Field arrangement
Matching of CSI
Aligning of spinal field
Implementation of plan
Patient position
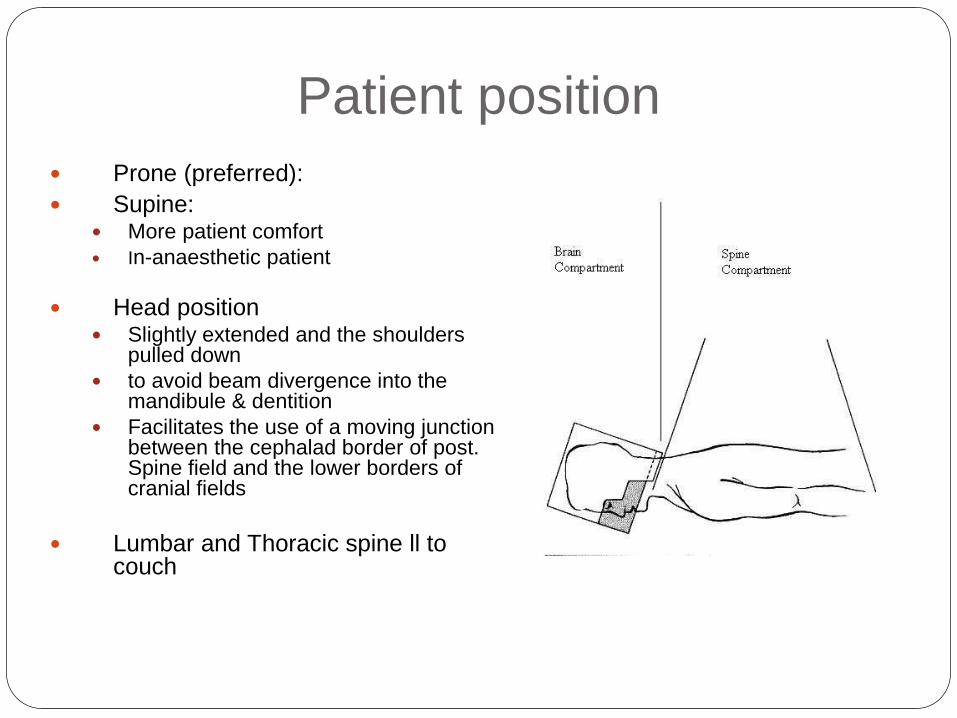
Prone (preferred):
Supine: More patient comfort
In-anaesthetic patient
Head position Slightly extended and the shoulders
pulled down
to avoid beam divergence into the mandibule & dentition
Facilitates the use of a moving junction between the cephalad border of post. Spine field and the lower borders of cranial fields
Lumbar and Thoracic spine ll to couch
Immobilization method
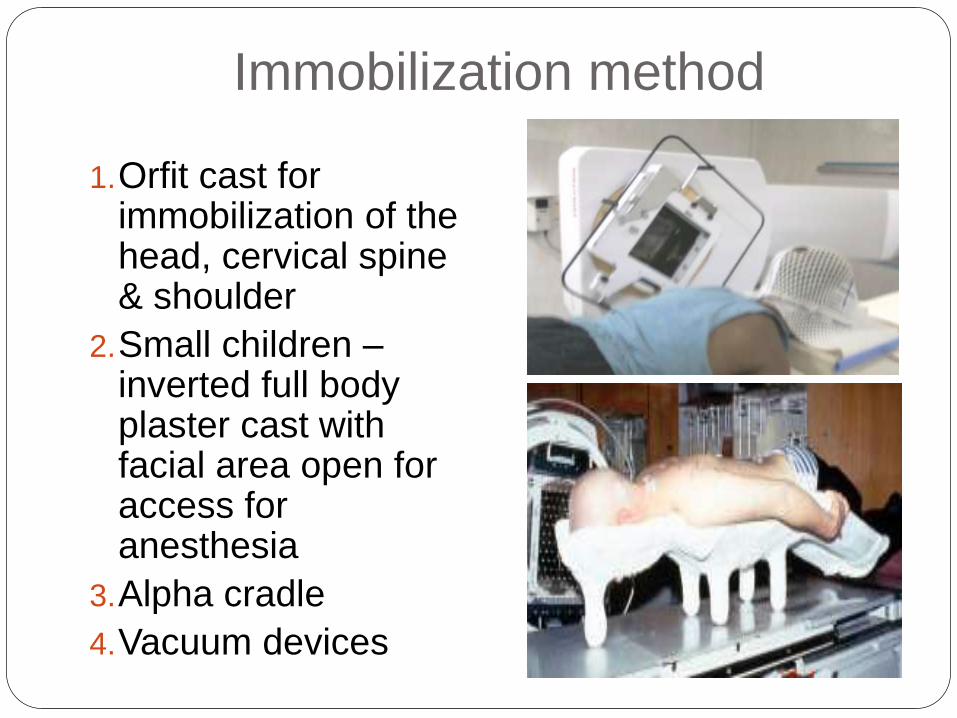
1.Orfit cast for immobilization of the head, cervical spine & shoulder
2.Small children –inverted full body plaster cast with facial area open for access for anesthesia
3.Alpha cradle
4.Vacuum devices
FIELD ARRANGEMENTS
Whole brain
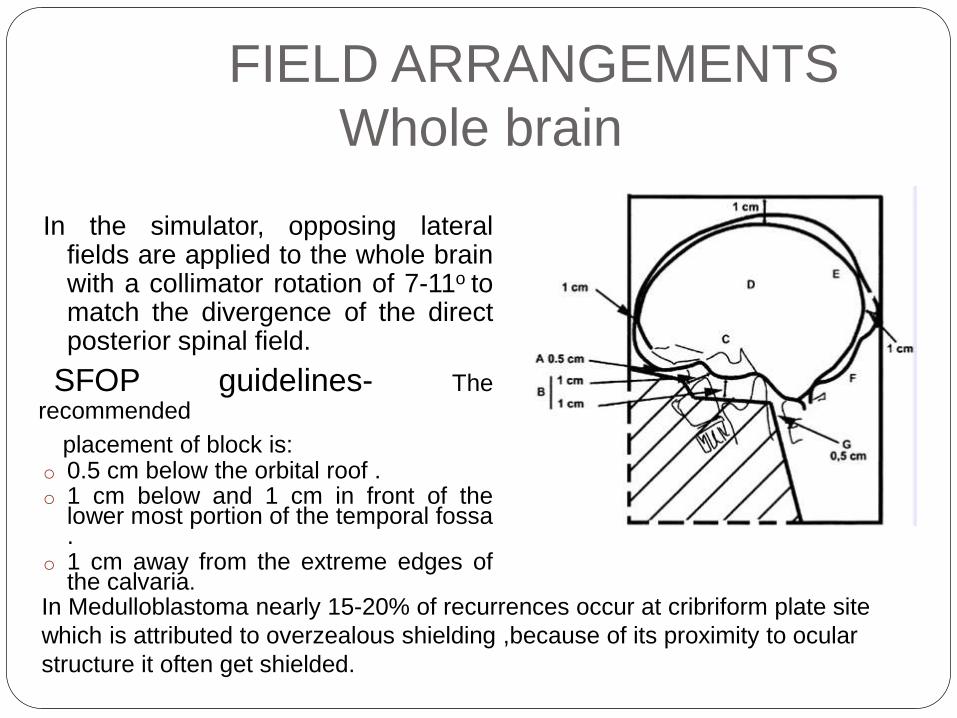
In the simulator, opposing lateralfields are applied to the whole brainwith a collimator rotation of 7-11o tomatch the divergence of the directposterior spinal field.
SFOP guidelines- Therecommended
placement of block is:o 0.5 cm below the orbital roof .o 1 cm below and 1 cm in front of the
lower most portion of the temporal fossa.
o 1 cm away from the extreme edges ofthe calvaria.
In Medulloblastoma nearly 15-20% of recurrences occur at cribriform plate site
which is attributed to overzealous shielding ,because of its proximity to ocular
structure it often get shielded.
Spinal field
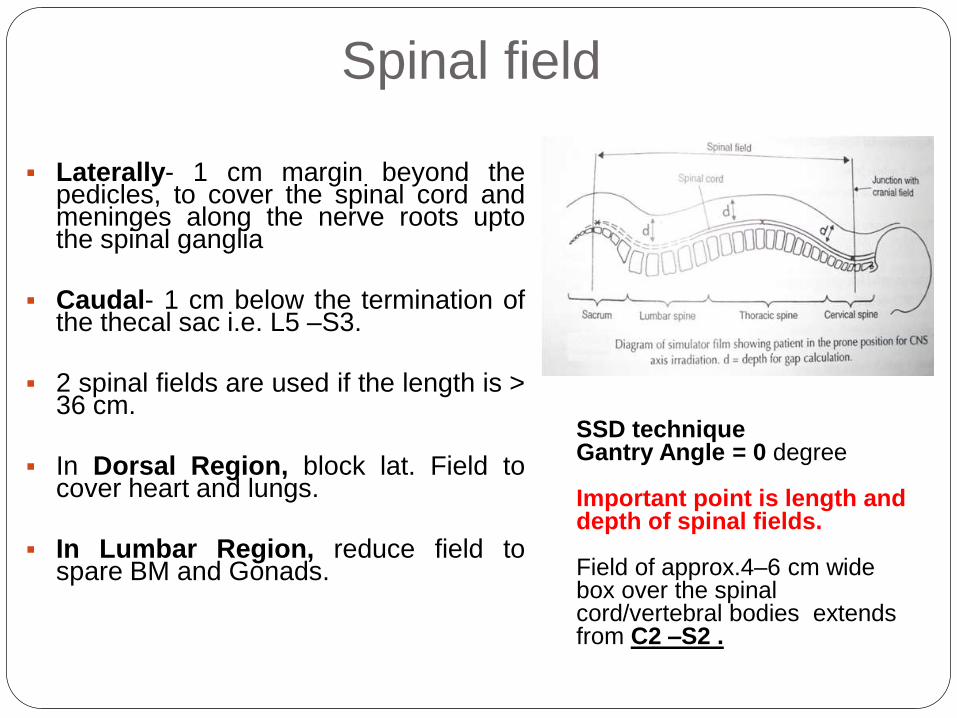
Laterally- 1 cm margin beyond thepedicles, to cover the spinal cord andmeninges along the nerve roots uptothe spinal ganglia
Caudal- 1 cm below the termination ofthe thecal sac i.e. L5 –S3.
2 spinal fields are used if the length is >36 cm.
In Dorsal Region, block lat. Field tocover heart and lungs.
In Lumbar Region, reduce field tospare BM and Gonads.
SSD techniqueGantry Angle = 0 degree
Important point is length and depth of spinal fields.
Field of approx.4–6 cm wide box over the spinal cord/vertebral bodies extends from C2 –S2 .
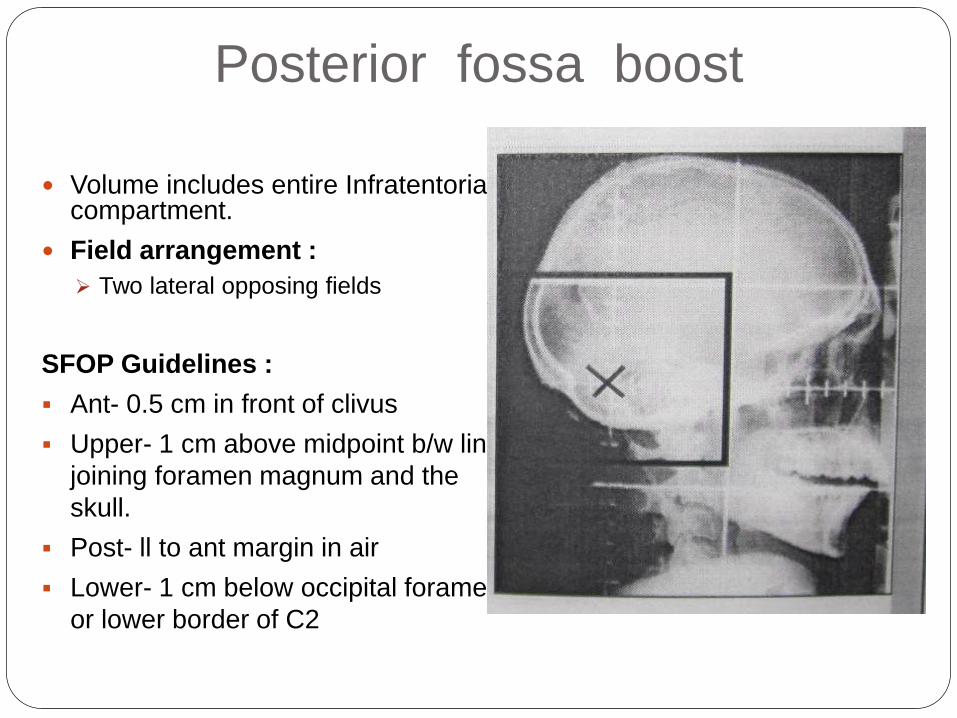
Posterior fossa boost
Volume includes entire Infratentorialcompartment.
Field arrangement :
Two lateral opposing fields
SFOP Guidelines :
Ant- 0.5 cm in front of clivus
Upper- 1 cm above midpoint b/w line
joining foramen magnum and the
skull.
Post- ll to ant margin in air
Lower- 1 cm below occipital foramen
or lower border of C2
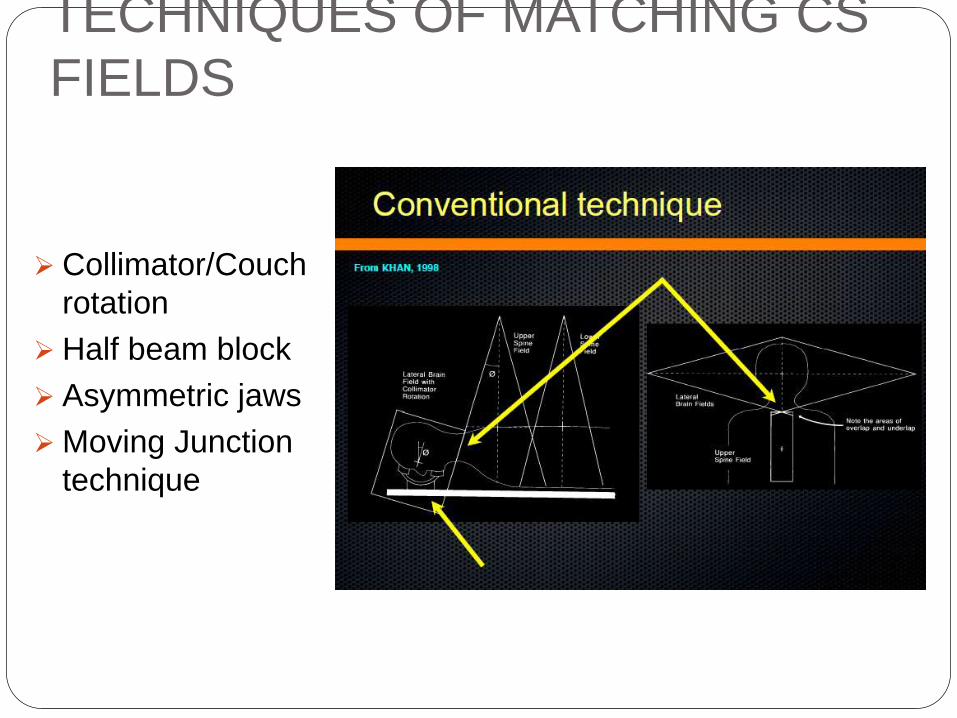
TECHNIQUES OF MATCHING CS
FIELDS
Collimator/Couch
rotation
Half beam block
Asymmetric jaws
Moving Junction
technique
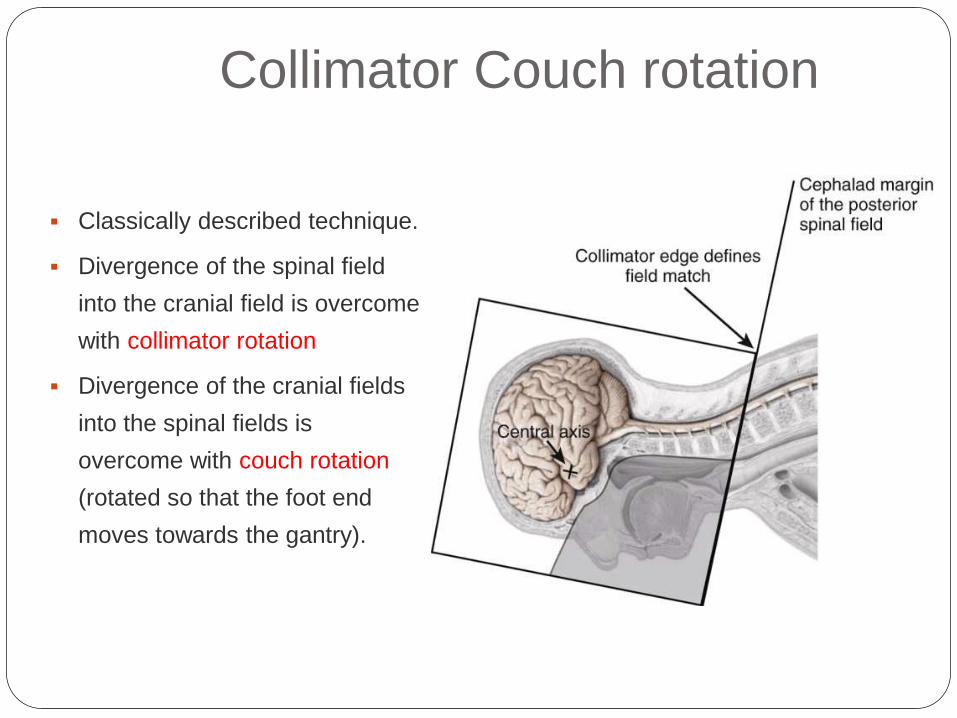
Collimator Couch rotation
Classically described technique.
Divergence of the spinal field
into the cranial field is overcome
with collimator rotation
Divergence of the cranial fields
into the spinal fields is
overcome with couch rotation
(rotated so that the foot end
moves towards the gantry).
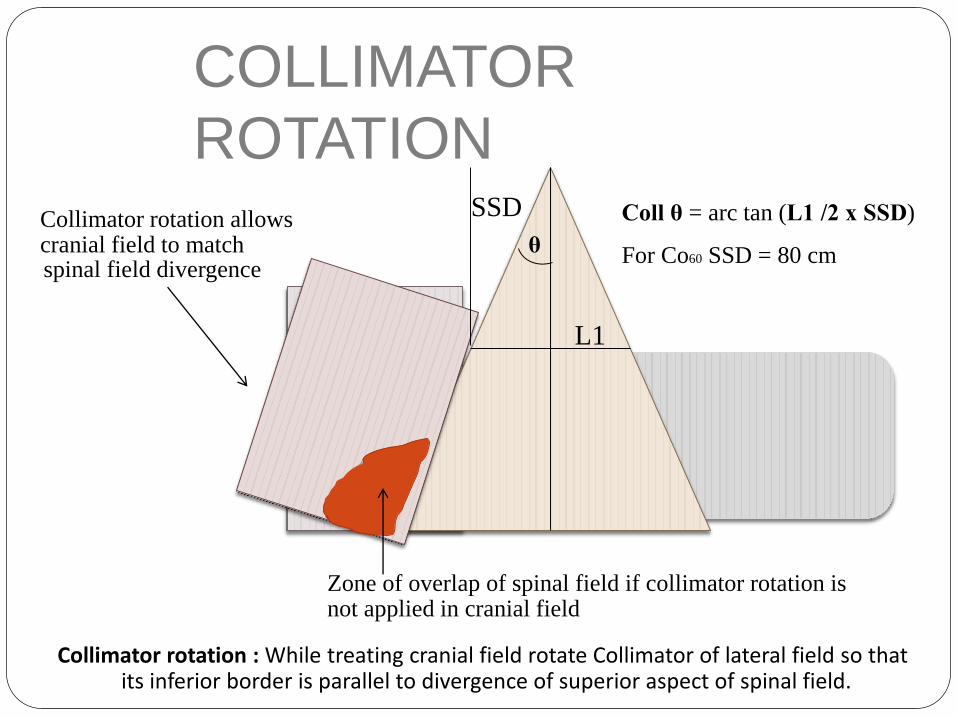
Collimator rotation allowscranial field to matchspinal field divergence
Coll θ = arc tan (L1 /2 x SSD)
For Co60 SSD = 80 cm
Zone of overlap of spinal field if collimator rotation isnot applied in cranial field
SSD
L1
Collimator rotation :While treating cranial field rotate Collimator of lateral field so thatits inferior border is parallel to divergence of superior aspect of spinal field.
θ
COLLIMATOR
ROTATION
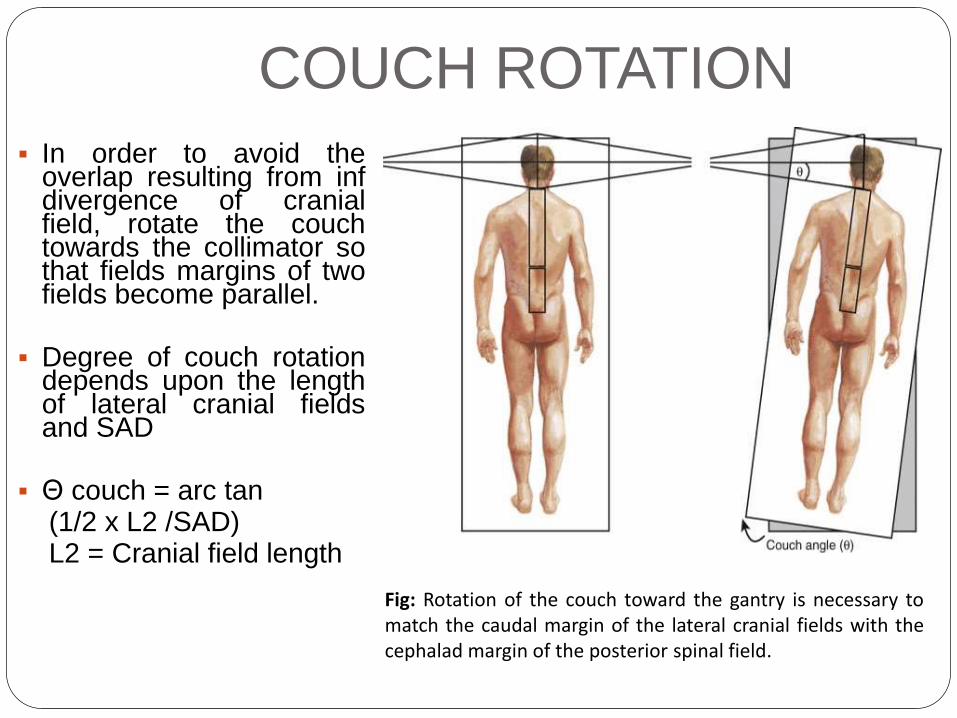
In order to avoid theoverlap resulting from infdivergence of cranialfield, rotate the couchtowards the collimator sothat fields margins of twofields become parallel.
Degree of couch rotationdepends upon the lengthof lateral cranial fieldsand SAD
Θ couch = arc tan(1/2 x L2 /SAD)L2 = Cranial field length
COUCH ROTATION
Fig: Rotation of the couch toward the gantry is necessary tomatch the caudal margin of the lateral cranial fields with thecephalad margin of the posterior spinal field.
COUCH ROTATION
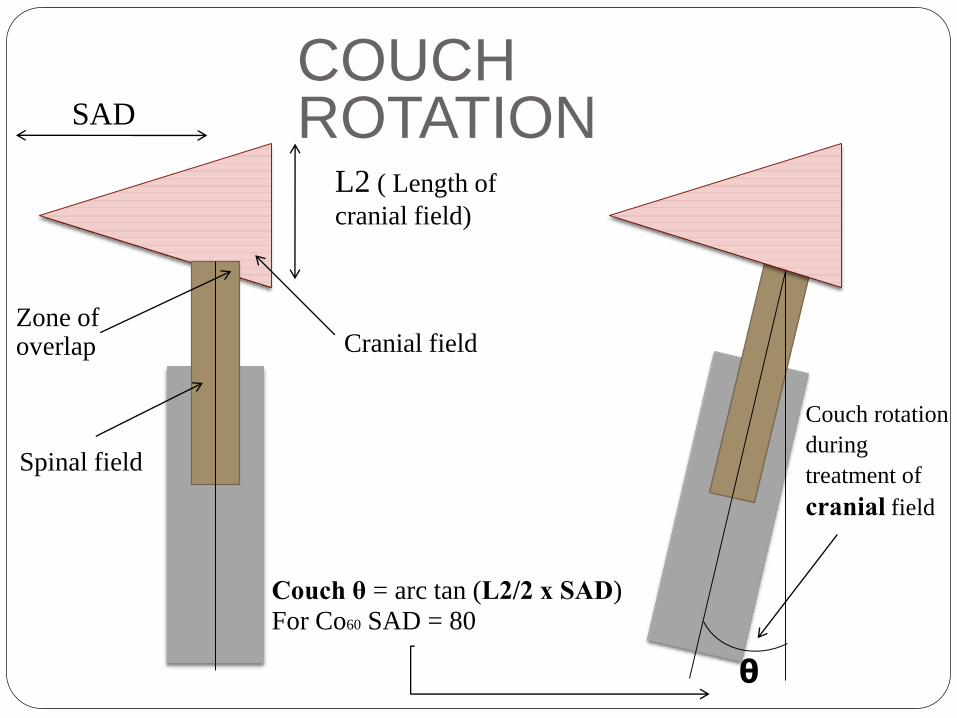
Couch θ = arc tan (L2/2 x SAD)
For Co60 SAD = 80
L2 ( Length of
cranial field)
Cranial field
SAD
Zone ofoverlap
Spinal field
Couch rotation
during
treatment of
cranial field
θ
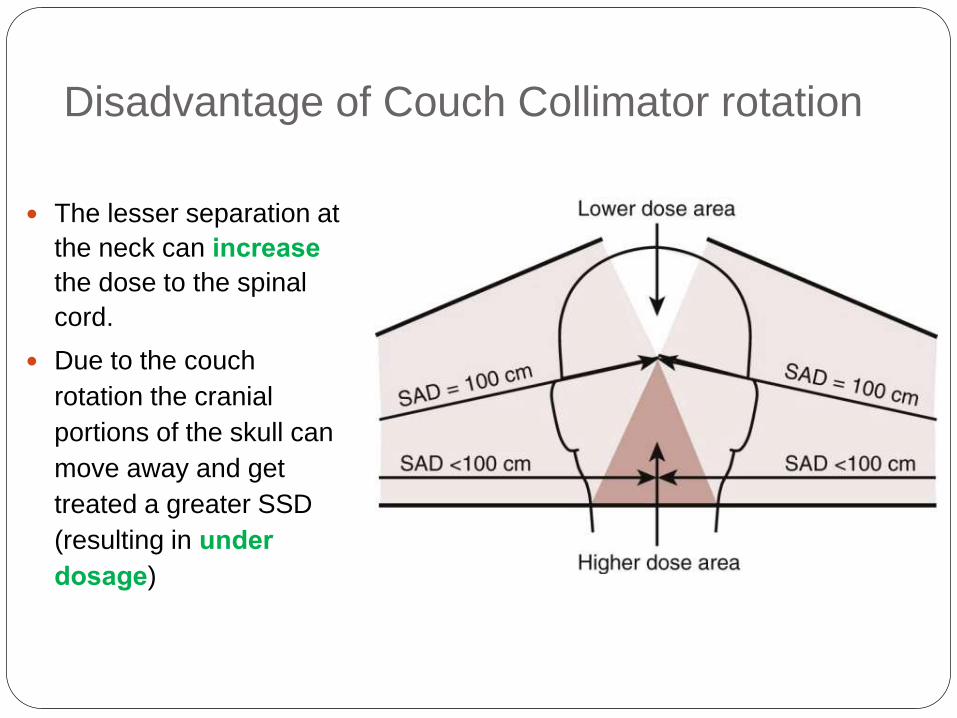
Disadvantage of Couch Collimator rotation
The lesser separation at
the neck can increase
the dose to the spinal
cord.
Due to the couch
rotation the cranial
portions of the skull can
move away and get
treated a greater SSD
(resulting in under
dosage)
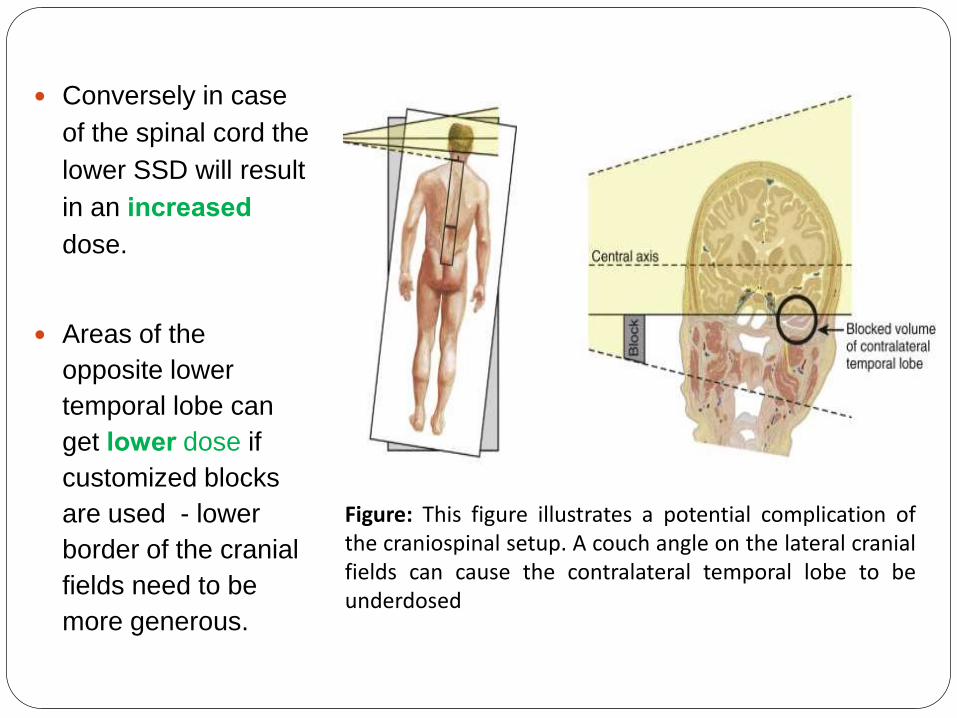
Conversely in case
of the spinal cord the
lower SSD will result
in an increased
dose.
Areas of the
opposite lower
temporal lobe can
get lower dose if
customized blocks
are used - lower
border of the cranial
fields need to be
more generous.
Figure: This figure illustrates a potential complication ofthe craniospinal setup. A couch angle on the lateral cranialfields can cause the contralateral temporal lobe to beunderdosed
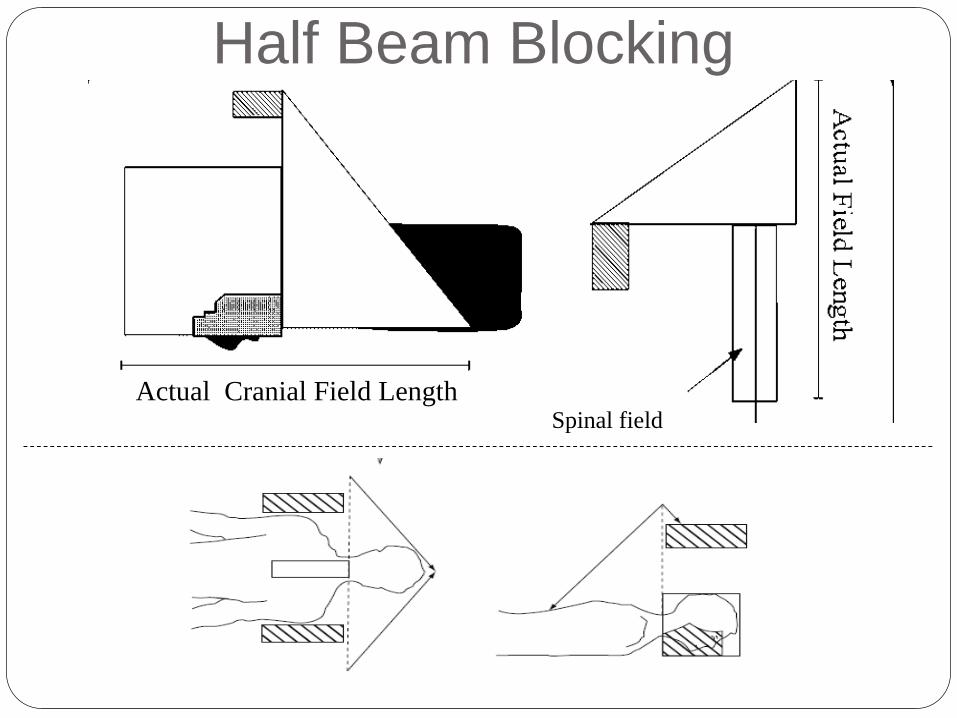
Half Beam Blocking
Actual Cranial Field LengthSpinal field
Disadvantage of the half beam
technique
Requires asymmetrical jaws
In event of misaligned jaws or improper
movement unintended dose inhomogenecities
Spinal field size reduced – two fields needed in
most children
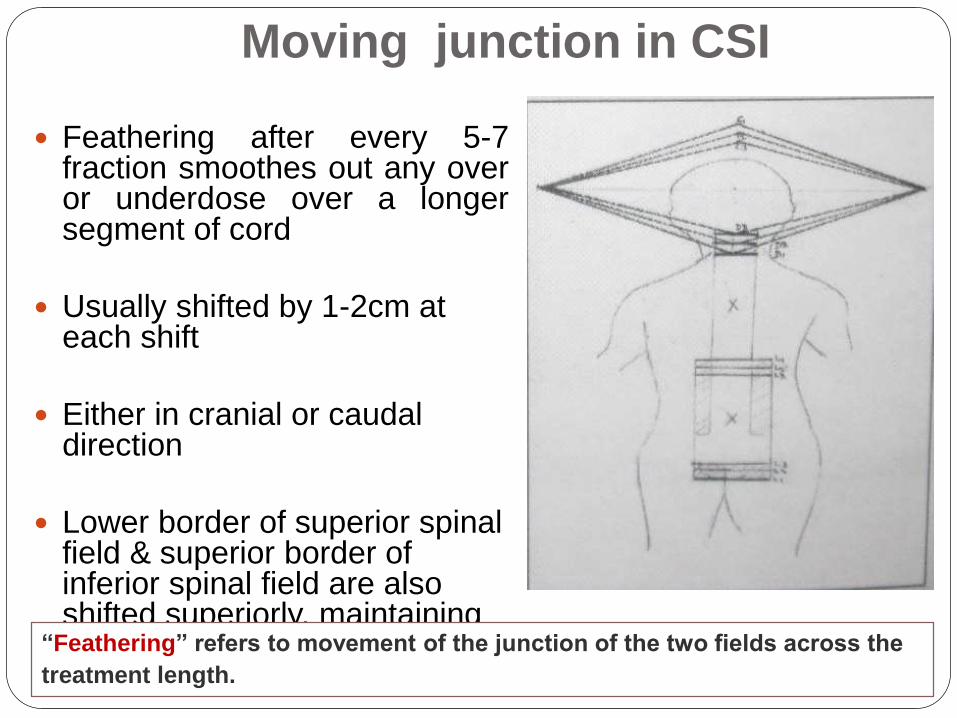
Moving junction in CSI
Feathering after every 5-7fraction smoothes out any overor underdose over a longersegment of cord
Usually shifted by 1-2cm at each shift
Either in cranial or caudal direction
Lower border of superior spinal field & superior border of inferior spinal field are also shifted superiorly, maintaining the calculated gap b/w them“Feathering” refers to movement of the junction of the two fields across the
treatment length.
Aligning Spinal field
Abutting fields will result in heterogenous
dose to the spinal cord
To overcome this various techniques are
available
o Gap technique
o Double junction technique
o Moving junction technique
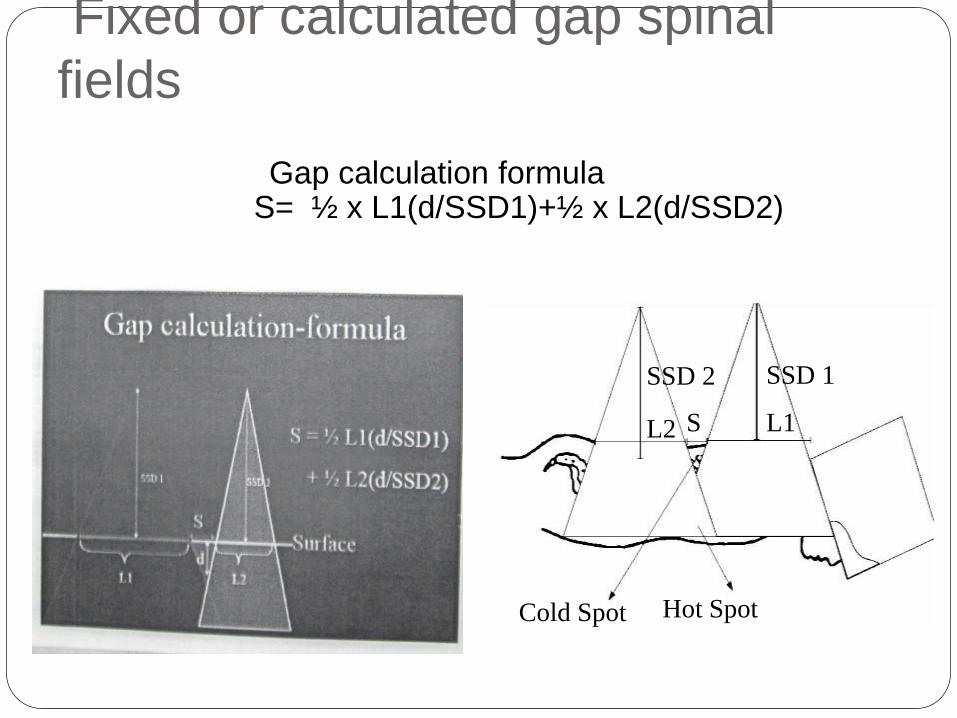
Fixed or calculated gap spinal
fields
Gap calculation formulaS= ½ x L1(d/SSD1)+½ x L2(d/SSD2)
Cold Spot Hot Spot
SSD 2 SSD 1
L2 S L1
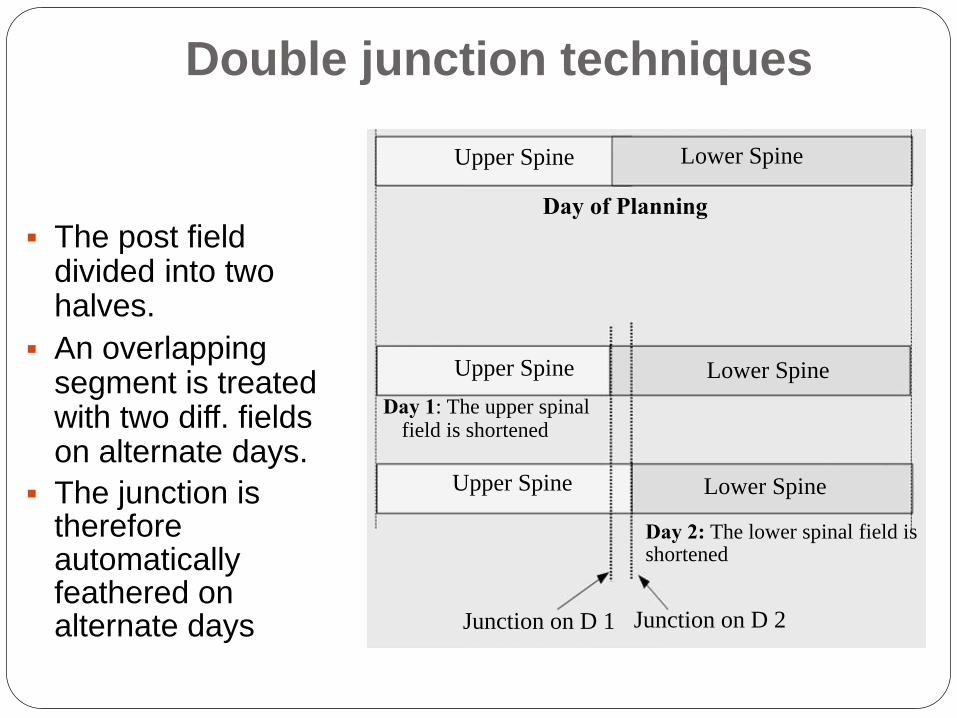
Double junction techniques
The post field divided into two halves.
An overlapping segment is treated with two diff. fields on alternate days.
The junction is therefore automatically feathered on alternate days
Upper Spine Lower Spine
Day of Planning
Upper Spine Lower Spine
Day 1: The upper spinalfield is shortened
Upper Spine Lower Spine
Day 2: The lower spinal field isshortened
Junction on D 1 Junction on D 2
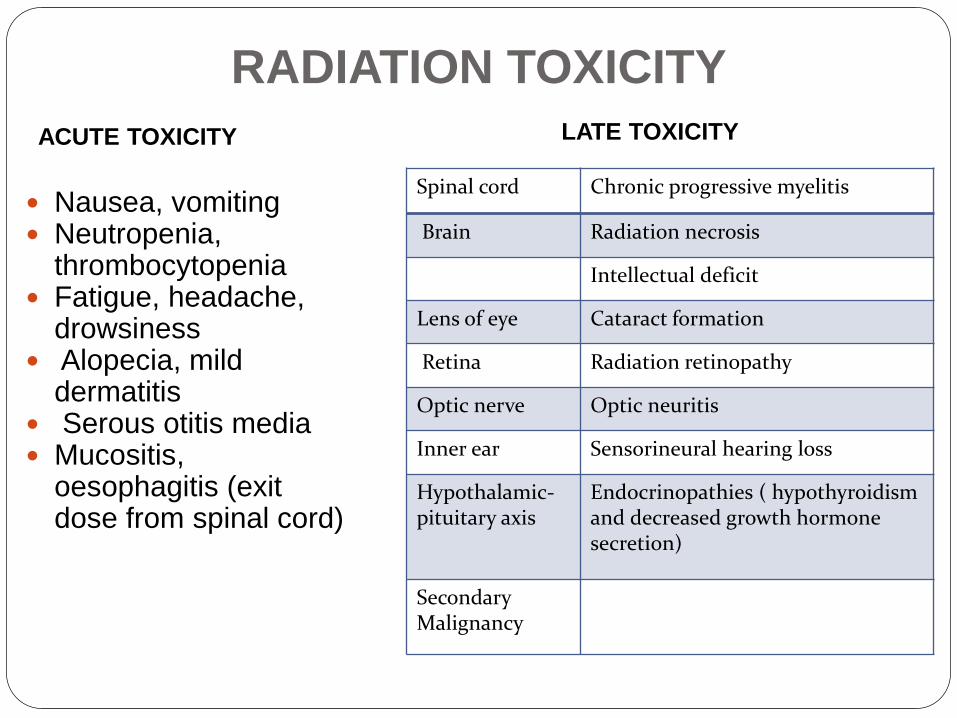
RADIATION TOXICITY
ACUTE TOXICITY
Nausea, vomiting Neutropenia,
thrombocytopenia Fatigue, headache,
drowsiness Alopecia, mild
dermatitis Serous otitis media Mucositis,
oesophagitis (exit dose from spinal cord)
Spinal cord Chronic progressive myelitis
Brain Radiation necrosis
Intellectual deficit
Lens of eye Cataract formation
Retina Radiation retinopathy
Optic nerve Optic neuritis
Inner ear Sensorineural hearing loss
Hypothalamic-pituitary axis
Endocrinopathies ( hypothyroidism and decreased growth hormone secretion)
Secondary Malignancy
LATE TOXICITY
Monitoring during CSI
CSI results in predictable, if quantitatively variable, acutechanges in the peripheral blood counts.
Neutropenia or thrombocytopenia are most often notedduring or after the third week of CSI.
Traditionally, CSI is interrupted if:
The TLC falls below 3000/cumm
The neutrophil count falls below 1,000 cells/ml
Platelet count falls below 80,000/cumm
Any neutropenia with fever or thrombocytopenia withbleeding manifestations
If blood counts necessitate interrupting CSI for more than2 consecutive days, initiation of posterior fossa irradiationcan be done
A biweekly hemogram should be done – one on Mondayand the next on Thursday.
Pediatric
Medulloblastoma
Prognosis :5yr survival rate
Standard risk ds – 78%
High risk ds – 30-55%
Infants – 30%
Summary
Medulloblastoma is pediatric age group tumor
Raised ICT is the most common presentation
CT, MRI have important role in diagnosis and treatment
Surgery is the primary modality of treatment
RT has central role in treatment
Standard risk:
Surgery CSI or
CCRT followed by post radiation chemotherapy
High risk: CSI and post RT chemotherapy
Infants treated with intent to avoid or delay the RT
Long term neurological sequalae seen in CSI
Medulloblastom
a
Prediction 2019
Imaging diagnosis of tumor
Stereotactic biopsy for molecular profiling and
subclassification
Chemotherapy alone ( conventional and novel
pharmacotherapeutics )
Aggressive surgical therapy and radiation therapy
will be relegated to past
THANKS
Top Related