





Languages
Pages
Legal

Slide 1
Pulmonary Stereotactic Ablative Radiotherapy:
Current Implementation and Future Directions
CTOP Conference 2014Philip Schaner M.D., Ph.D
I have no conflicts of interest to report
Definition of Stereotactic Body Radiotherapy Method of delivering external beam radiotherapy (EBRT) Particles (proton) or photonDose per Fraction: at least equivalent to radical doses in conventional fractionation: 5 34 gray (Gy) [Conventional Fractionation: 1.8 2 Gy]Accurately delivers EBRT with a high degree of conformalitySpatial and Temporal resolution of target and organs at riskMaintenance of high spatial targeting accuracy throughout the entire treatmentImmobilizationHigh frequency position monitoring through integrated image guidance Respiratory Motion ManagementFew fractions: 1 - 10Nomenclature:Stereotactic ablative radiotherapy (SABR)Stereotactic body radiotherapy (SBRT)
SBRT LUNG
Subset of NSCLC appropriate for SBRT Stage I subset: typically < 5 cm in maximal dimension Not invading outside the chest (can be touching pleura) Not invading into lobar bronchus Minimal associated lung collapse Mass well delineated
Subset of NSCLC appropriate for SBRT Mass too large, invading into nearby structures
Primary acceptable but nodal disease present
Treatment Planning Highly conformal dose distribution with rapid dose fall off Maximally spare adjacent organs Low dose spill High dose spill
Accurate Delivery Target localization Lung cancer is a moving target.
4D Treatment DeliveryPatient Breaths Normally Control when XRT is on
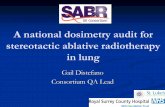
Multi-institutional Phase II Data: RTOG 0236 Inclusion: NSCLC T1 or T2, N0,M0 Peripheral: > 2 cm from proximal bronchial tree Medically inoperable: FEV1 40%, DCLO >40% Methodology: Dose escalation to 20 Gy x 3 fractions (60 Gy) Accrual: 38 pts => 63 lesions Rusthoven et al. JCO 2009ClinicalMulti-institutional phase I/II trial of stereotactic body radiation therapy for lung metastases
Results: Local control: 2 yr = 96%
Patient characteristicsClinical
Rusthoven et al. JCO 2009
Toxicity: Grade 3: 8% Grade 4-5: 0%
Areas of Investigation What is the appropriate SABR dose for peripheral lesions?
Areas of InvestigationRTOG 0915 interim outcomes: N=94
Median FU 20.6 months
No significant difference with respect to toxicity in both arms: 9.8% 34 Gy vs 13.3% 48 Gy > Gr 3 toxicities.
Local Control at 1 yr 97% both arms.
Winner? Need longer term follow up Local Failure increases over time in many series, one year is not enough follow up.
What is the appropriate SABR dose for centrally located lesions?
Areas of Investigation
Measuring SABR against Surgery Stage IA NSCLC
Peripheral lesionARM 1:Anatomical surgical resection with LN dsxnARM 2:SABR20 Gy x 3
12 Gy x 5FOLLOW
UPROSEL Trial (Netherlands)Terminated due to poor accrualAreas of Investigation
Measuring SABR against Surgery Stage I NSCLC < 4 cm Good surgical candidate FEV1 > 40% pred DLCO > 40% predPost-op predicted FEV1 > 30%ARM 1:Lobectomy or pneumonectomyARM 2:SABR using Cyberknife
Peripheral: 20 Gy x 4Central: 15 Gy x 4FOLLOW
UPLung Cancer STARS trial: phase III, endpoint 3 yr OSAreas of Investigation
Measuring SABR against Surgery Histological confirmation NSCLC and confirmation N2/N3 negative lymph nodesT < 3 cm Peripheral High risk for surgery MajorFEV1 50% predDLCO 50% predMinorAge 75 yearsFEV1 51-60% predDLCO 51-60% pred
ARM 1:Sublobar Resection Brachytherapy (SR)ARM 2:Stereotactic Body Radiation Therapy (SBRT) 18 Gy X 3 = 54 GyFOLLOW
UPACOSOG Z4099/RTOG 1021 Phase III TrialOpened June 2011Areas of Investigation
Combining radiofrequency ablation with SABRUNM: RFA combined with SABR for large lung tumorsT2-4N0 > 3 cm; N1-3 if M1 eligible40 Gy/5 fractions escalating to 50 Gy/5 fractions f/b RFA procedure
Areas of Investigation Using SBRT as a boost for Stage II/III NSCLC U Kentucky: Stage IIA selected III-B 59.4 Gy chemoradiotherapy => if residual disease: boost 10 Gy x 2 (peripheral) Proton vs Photon SBRT SBRT combined with chemotherapy Maintenance chemotherapy vs consolidative SBRT for Stage IV NSCLC UTSW: 1st line chemo (no biologics) => up to six discrete extracranial lesionsU Kentucky: T1-T3N0 NSLC => SBRT then adjuvant cisplatin + docetaxel or pemetrexed
Questions.
Top Related