






Languages
Pages
Legal


Proactive Rounding – Actively Caring
Trudy Reid & Mary BurkeSouthern HSC Trust
WSCNTL 2014, Kings HallLeading Care, Leading Teams - Innovating and Supporting Person-Centred Care

Southern Health and Social Care Trust
Trudy Reid & Mary Burke
Southern Health and Social Care Trust
Trudy Reid & Mary Burke
Actively CaringActively Caring

Organisation of Care Organisation of Care
The aim of this project is to review and address how nursing / midwifery care is organised and delivered in acute wards /
departments, identify areas of best practice and to recognise opportunities to deliver patient safety and improve the patient
experience.

Phased approachPhased approach
Two acute Hospital sites Base Line 12 hour Observations of practice
Phase 1 – 11 pilot wards
Phase 2 - 19 wards across both sites
Evaluation included repeat Observations of practice

Safe Administration of MedicinesSafe Administration of Medicines
Aim– To support individual nurses and midwives achieve safe administration of
medicines and reduce inappropriate omitted and delayed medicines
Methodology/Implementation – Observation of medicines assessment tool– Self-assessment– Reflective learning– Work shop for band 6-7 (39 sisters attended)
Evaluation – Observation of practice– Audit – Reduction in all medication incidents (although incidents may increase initially
as awareness heightened)– 53% completed self evaluation programme
This work was shared with Nurse Consultant, Clinical Education Centre, who will integrate the elements of this work stream

Medicines Self Assessment Medicines Self Assessment 1.0 What is a critical medicine?
Critical medicines are those where the omission or delay is likely to cause the most harm.
2.0 Name groups of critical medicines Anti infectives (all IV Antibiotics, oral & suspensions) Insulin Medicines to treat Parkinson’s Resuscitation medicines (held in Resuscitation trolley) Steroids Stat doses
3.0 How many hours do you have before a medicine dose is recorded as an (a) omitted dose (b) delayed dose? (a) before the next dose is due (b) 2 hours
4.0 What would you do if a critical medicine was not available at 10.pm if a critical medicine was not available? Contact emergency duty pharmacist
5.0 What would you do if you noticed that a critical medicine had not been given? What should happen next? Escalation. Short RCA carried out by ward sister, ward pharmacist and patient’s consultant.
5.0 If a patient is nil by mouth and taking critical medicines what would you do? Refer to Trust Guidance
6.0 Knowledge of medicines: Therapeutic effect ,Side effects , Usual Dose and Route Demonstrates an understanding of the uses and side effects associated with the medicines for administration (take three examples from medicine round)
7.0 As a nurse, what guides your practice in relation to management of medicines? NMC Standard for Medicines Management (2010) Medicines Management Code (March 2009)
8.0 Have you completed the IV cannulation course? Do you use it to keep your skills up? 9.0 Have you attended Administration of Medicines in the last 3 years? 10.0 Any other questions arising from the observation of practice



Shift HandoverShift HandoverAim
– To review how shift handover currently takes place– To review the literature on shift handover– To provide a standardised approach to shift handover
Methodology/Implementation – Use SBAR guidance and template or adapt current templates
Evaluation – Observation of practice– Audit of handover process
Outcome– The principles of the SBAR model of communication for handover are
now implemented in all wards, most areas now generated electronically– Shift handover observed to be effective – reduction in time of handover -
45 mins – 25mins in MAU and 30mins-15 mins in Surgical admission ward, with only applicable and relevant information communicated

Hand Over Template Hand Over Template Situation Background Assessment Recommendations
No of days in patient
NameAge
Reason for Admission/Diagnosis / Investigations
Relevant
Medical History
Allergy statusInfection Control
DNAR
MEWS, nutritional, hygiene, elimination, change in condition etc
Planned investigations,On-going plan of care
EDD
Bay 1
1
2
3
4

Customer CareCustomer CareAims
– To ensure all staff are aware of their responsibility to inspire public confidence in all aspects of delivery of care
Methodology /Implementation – Delivery of PowerPoint presentation – Nursing supervision– Engaging with staff
Evaluation – Evaluation from participants – Observation of practice– Improve patient/client experience– Reduction in complaints
Outcome – Overall total- 764 staff attended (58%)– Extended to other areas and disciplines – outpatients/community
midwives/AHPs/medical staff (approx. 100)

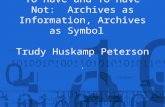
Proactive Rounding Proactive Rounding Aim To ensure that all patients have face to face contact with
nursing staff minimum of two hourly
Methodology Use of proactive rounding tool
Evaluation Observation of practice Patient rounding audit too
Outcomes
Falls reduction by 25% *
‘At first I thought intentional rounding was nothing more than a paper exercise, now I feel it is really beneficial to patient care as now I hardly ever hear a buzzer and all patients are able to tell exactly who their nurse is..’
Patient Name: _____________________ HSC Number: __________________________
Guidance notes Introduce yourself
May be completed by any member of Nursing staff, to be carried out on ALL patients, (using discretion if patient is independent re some areas eg toilet/position)
Tick boxes indicate you have had contact regarding these issues- Actions taken are recorded in nursing evaluation/appropriate charts
To be completed during night and record PA – Patient appears to be asleep
(if patient at high risk of falls carry out hourly – min 2 hourly) Rounding to be carried out ________hourly
Date Time Pain Position Toilet
Needs Check
Environment is clean and tidy/bed in
lowest position
Check ‘is there anything else you need’
Staff initals
Addressograph

Proactive Rounding Audit ToolProactive Rounding Audit ToolPatient Rounding Audit Tool
Date:________ Time:_________ Ward:_____________ Please tick for Yes and cross for No
Patient 1 Location on ward____________
Patient 2 Location on ward____________
Patient 3 Location on ward____________
Patient 4 Location on ward____________
1. Patient can correctly identify name of nurse (and HSW) caring for them that: Morning/Afternoon/Night duty. (Delete as appropriate)
2. Patient can indicate that someone has spoken to them within the past two hours with regards to comfort, pain and toilet needs.
3. Patient can indicate that nursing staff reassured them when they would return
4. Did the patient need to use Call Bell today?
5. Is bed table/call bell always within easy reach?
Name of person carrying out the audit: _________________________________

Other elements of organisation of care Other elements of organisation of care
Model of care Prevention of Health Care Associated
Infection Roles and Responsibilities

Rotational ProgrammeRotational Programme
Induction Programme Competency based Programme Named preceptors Rotational programme
– ED/MAU 6 months ED 6 months in MAU
– Trauma/orthopaedics Clinical supervision

Lunch & LearnLunch & Learn
MDT Learning together Sharing the learning New Initiatives Examples of good practice and areas for
development NIPEC Educational Audit

Patient Safety Briefings Patient Safety Briefings
Weekly meeting at ward level New guidance, policies, procedures and
best practice Audit feed back including NQI Sharing the learning from complements,
complaints, incidents, RCA and SAI Feed back from weekly sisters meetings Correspondence

Actively Care
Top Related