






Languages
Pages
Legal


Primary CarePrimary CareValue PropositionValue Proposition
Robert Phillips, MD MSPHRobert Phillips, MD MSPH
The Robert Graham CenterThe Robert Graham Center
AcademyHealth 2007AcademyHealth 2007

Value, Problems, PropositionsValue, Problems, Propositions
►ValueValue Health, Costs, EquityHealth, Costs, Equity
►ProblemsProblems Undervalued, underinvested, underpaidUndervalued, underinvested, underpaid
►PropositionsPropositions Patient-centered Medical HomePatient-centered Medical Home Change MedicareChange Medicare New Social Contract with Primary CareNew Social Contract with Primary Care

ProblemsProblems
““Primary Care in the United States is on death Primary Care in the United States is on death row”row”
--David Reuben, MD--David Reuben, MD
American Journal of Medicine January, 2007American Journal of Medicine January, 2007
““Unless there are changes in the broader health Unless there are changes in the broader health care system and within the specialty, the care system and within the specialty, the position of family medicine in the United States position of family medicine in the United States may be may be untenableuntenable in a 10-20 year time frame” in a 10-20 year time frame”
----Future of Family Medicine Project, 2002Future of Family Medicine Project, 2002

ValueValue

ValueValue
►Evidence for Effectiveness:Evidence for Effectiveness: People live longer and fewer die due to People live longer and fewer die due to
heart and lung diseaseheart and lung disease Less ER and hospital useLess ER and hospital use Better preventive careBetter preventive care Reduced health disparitiesReduced health disparities
Macinko J. Starfield B. Shi L. HSR. 2003;38(3):831-65.

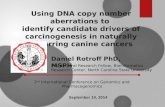
Primary-care score vs Primary-care score vs health outcomeshealth outcomes
UnitedStates
AUS
BELGER
CANFIN
SP SWE
UK
0
1
2
3
4
5
6
7
8
9
10
0 1 2 3 4 5 6 7 8 9 10 11 12
better------Primary care score ranking-------worse
Hea
lth
care
Ou
tco
mes
R
ank* NTH/DK
*Rank based on patient satisfaction, expenditures per person, 14 health indicators, and medications per person in Australia, Belgium, Canada, Denmark, Finland, Germany, Netherlands, Spain, Sweden, United Kingdom, United States



Of 21 OECD countries, the Of 21 OECD countries, the United States is, by far, the United States is, by far, the most socially inequitable most socially inequitable (poor versus non-poor) in (poor versus non-poor) in terms of the annual terms of the annual probability of visiting a probability of visiting a physician. physician.
Starfield 03/06IC 384Source: van Doorslaer et al, CMAJ 2006; 174:177-83.

ValueValue
►Evidence for Efficiency:Evidence for Efficiency: Less ER and hospitals useLess ER and hospitals use Fewer testsFewer tests Higher patient satisfactionHigher patient satisfaction Lower medication useLower medication use Less care-related costsLess care-related costs
Greenfield S, et al JAMA 1992;267:1624-30.Forrest CB. Starfield B. JFP:. 1996;43(1):40-8. Macinko J. Starfield B. Shi L. HSR. 2003;38(3):831-65.

Expenditures vs Primary Expenditures vs Primary Care ScoreCare Score
Barbara Starfield, 1994 and 2001
UNITED STATES
AUS BEL
GERCAN
DKFIN
NTH
SPASWEUK
$0
$1,000
$2,000
$3,000
$4,000
0 2 4 6 8 10 12
better Primary Care Score Rank worse
Per
Cap
ita
Hea
lth
Car
e E
xpen
dit
ure
s

ValueValueBetter OutcomesBetter Outcomes
Landmark 2005 study shows U.S. counties Landmark 2005 study shows U.S. counties more oriented to primary care achieve: more oriented to primary care achieve: • lower per capita expenditureslower per capita expenditures• lower medication uselower medication use• higher patient satisfactionhigher patient satisfaction
Increase of one primary care physician Increase of one primary care physician per 10,000 population associated with:per 10,000 population associated with:• 6 percent decrease in all-cause mortality6 percent decrease in all-cause mortality• 3 percent decrease in low birth-weight, and 3 percent decrease in low birth-weight, and
stroke mortalitystroke mortality
SOURCE: B. Starfield, et al, “The Effects of Specialist Supply on Populations’ Health,” Health Affairs (March 2005); W5-97.

There are large variations There are large variations in both costs of care and in both costs of care and in frequency of in frequency of interventions. Areas with interventions. Areas with high use of resources and high use of resources and greater supply of greater supply of specialists have NEITHER specialists have NEITHER better quality of care better quality of care NOR better results from NOR better results from care. care. Starfield 12/05
SP 3343
Sources: Fisher et al, Ann Intern Med 2003; Part 1: 138:273-87; Part 2: 138:288-98. Baicker & Chandra, Health Aff 2004; W4:184-97. Wennberg et al, Health Aff 2005; W5:526-43.

ProblemsProblems

ProblemsProblems
►UndervaluedUndervalued►UnderinvestedUnderinvested►UnderpaidUnderpaid

Problems--UndervaluedProblems--Undervalued
►Primary care can’t compete for the Primary care can’t compete for the hearts and minds of US Medical studentshearts and minds of US Medical students Average debt now $115k-$150kAverage debt now $115k-$150k LifestyleLifestyle
►Family Medicine filling >50% IMGs, Family Medicine filling >50% IMGs, losing programslosing programs
►General Internal Medicine, exodus to General Internal Medicine, exodus to subspecialties and hospitalssubspecialties and hospitals
►General Pediatrics—benefits from General Pediatrics—benefits from feminization, low-paying subspecialties feminization, low-paying subspecialties

Footprint of the University of Florida residency program in Jacksonville
Losing Losing ProgramsPrograms

Problem – UnderinvestedProblem – Underinvested
►Medicare voluntary reporting P4P Medicare voluntary reporting P4P programprogram 1.5% bonus 1.5% bonus
VSVS
►UK General Practice contractUK General Practice contract 25% bonus25% bonus

UK ExperienceUK Experience
►Actually began in 1990Actually began in 1990 Payment for health targets, preventionPayment for health targets, prevention GP fundholdingGP fundholding
►Contractual leverage over hospitals (cost Contractual leverage over hospitals (cost control)control)
►Build-out primary care services (access)Build-out primary care services (access)
Primary Care Organization developmentPrimary Care Organization development►Primary care trusts now control 80% of NHS Primary care trusts now control 80% of NHS
budgetbudget►Responsible for Responsible for Quality, Access, and CostsQuality, Access, and Costs

The New GP ContractThe New GP Contract
► In 2005, point-based bonus payments In 2005, point-based bonus payments 136 measures:136 measures: GP income related to achieving disease GP income related to achieving disease
specific quality standardsspecific quality standards Patient experience indicatorsPatient experience indicators Organisational indicatorsOrganisational indicators
► New money - Up to $77,000 more per New money - Up to $77,000 more per physician possiblephysician possible


US vs UKUS vs UK
►Comparison of US and UK practices on Comparison of US and UK practices on common measures: common measures:
US practices 41%US practices 41% UK 97%UK 97%

Problem-UnderinvestmentProblem-Underinvestment
►UK invested a decade and billions to UK invested a decade and billions to reorganize and empower primary carereorganize and empower primary care
►P4P was icing on the cakeP4P was icing on the cake

Problem--UnderpaidProblem--Underpaid
► Piecework payment for outpatient services Piecework payment for outpatient services greater fragmentation of medical care greater fragmentation of medical care greater use of outpatient technological servicegreater use of outpatient technological service
► Less attention given to continuity, Less attention given to continuity, integration of care, preventive medicineintegration of care, preventive medicine
► Decreased payments to primary-care Decreased payments to primary-care physicians and increased pressure to see physicians and increased pressure to see more patients more patients reduced time spent with each patientreduced time spent with each patient the quality of primary care suffered the quality of primary care suffered
Relman, AS. Medicine And The Free Market. The Health Of Nations. The New Republic 3/7/05

Medicare PaymentsMedicare Payments
►Basal payment (Conversion Factor, “SGR”)Basal payment (Conversion Factor, “SGR”) Evaluation & Management (E&M) affected by Evaluation & Management (E&M) affected by
growth in imaging, proceduresgrowth in imaging, procedures Expect 10-15% cuts next 2 yearsExpect 10-15% cuts next 2 years
►RBRVS “defies gravity”RBRVS “defies gravity” Real increases for primary care not possibleReal increases for primary care not possible
►20% increase in E&M really only 5% for FP and GIM20% increase in E&M really only 5% for FP and GIM
Distortions, lack of data for basing relative valueDistortions, lack of data for basing relative value
Gingsberg PB, Berenson RA. NEJM 356(12). 3/22/07Dodoo et al, in review

Number and Intensity of Medicare Number and Intensity of Medicare servicesservices
(1999 – 2003)(1999 – 2003)
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Evaluation &Management
Major procedures
Other non-majorprocedures
Imaging Tests
Pe
rce
nta
ge
ch
an
ge
19
99
-20
03
Source: Medicare Payment Advisory Commission (MedPac), Analysis of Medicare Claims
data, “Testimony before US House of Representatives”, Nov 17, 2005

Problem—Is any change Problem—Is any change possible?possible?
►"when those boomers start retiring en "when those boomers start retiring en masse, then that will be a tsunami of masse, then that will be a tsunami of spending that could swamp our ship of spending that could swamp our ship of state if we don't get serious…We state if we don't get serious…We suffer from a fiscal cancer…suffer from a fiscal cancer…the real the real problem is health care costsproblem is health care costs""
U.S. Comptroller General David U.S. Comptroller General David WalkerWalker
60 Minutes March 4, 200760 Minutes March 4, 2007

PropositionsPropositions

PropositionProposition
►Patient Centered Medical HomePatient Centered Medical Home Transform organization and financing of Transform organization and financing of
primary care = better value, primary care = better value, accountability, transparencyaccountability, transparency
ERISA Industry CommitteeERISA Industry Committee National Business Group on HealthNational Business Group on Health IBM, GM, GEIBM, GM, GE

PropositionProposition
►Change Medicare, others will followChange Medicare, others will follow Blow up “SGR”Blow up “SGR” Split “SGR” into E&M; Non-E&M and Split “SGR” into E&M; Non-E&M and
purposefully bolster E&Mpurposefully bolster E&M Change Relative Value Update processChange Relative Value Update process
►Reinstate laws of financial gravityReinstate laws of financial gravity►Purposefully revalue primary carePurposefully revalue primary care

PropositionProposition
►Abandon current Medicare Policies for Abandon current Medicare Policies for Primary CarePrimary Care
►Goroll Proposition—Comprehensive Goroll Proposition—Comprehensive Primary Care PaymentPrimary Care Payment PC panels of 1250 - 2000 pts per physicianPC panels of 1250 - 2000 pts per physician $500 per pt per year ($1M per physician)$500 per pt per year ($1M per physician) 25% to physician ($250k per year)25% to physician ($250k per year) 75% to invest in infrastructure75% to invest in infrastructure 3% increase overall spending, greater 3% increase overall spending, greater
offsets are likely outcomeoffsets are likely outcome
Top Related