






Languages
Pages
Legal

Preventing VAPPreventing VAP
- evidence for a care bundle - evidence for a care bundle
VAPVAP
• Incidence
~ 10 - 30% ventilated patients
7-15 / 1000 ventilator days
• Atributable mortality of 0-50%
• Atributable increase LOS of ~ 3 weeks
Prevent VAP Care BundlePrevent VAP Care Bundle
Reduce time on ventilator:• Assess sedation requirements daily• Assess suitability for weaning and extubation daily
While on ventilator:• Semi-recumbent positioning• Oral chlorhexidine • ? Subglottic drainage
128 ventilated patients
Randomised: daily sedation break and titration v. standard care
Outcomes: duration of ventilation, ICU & hospital stay
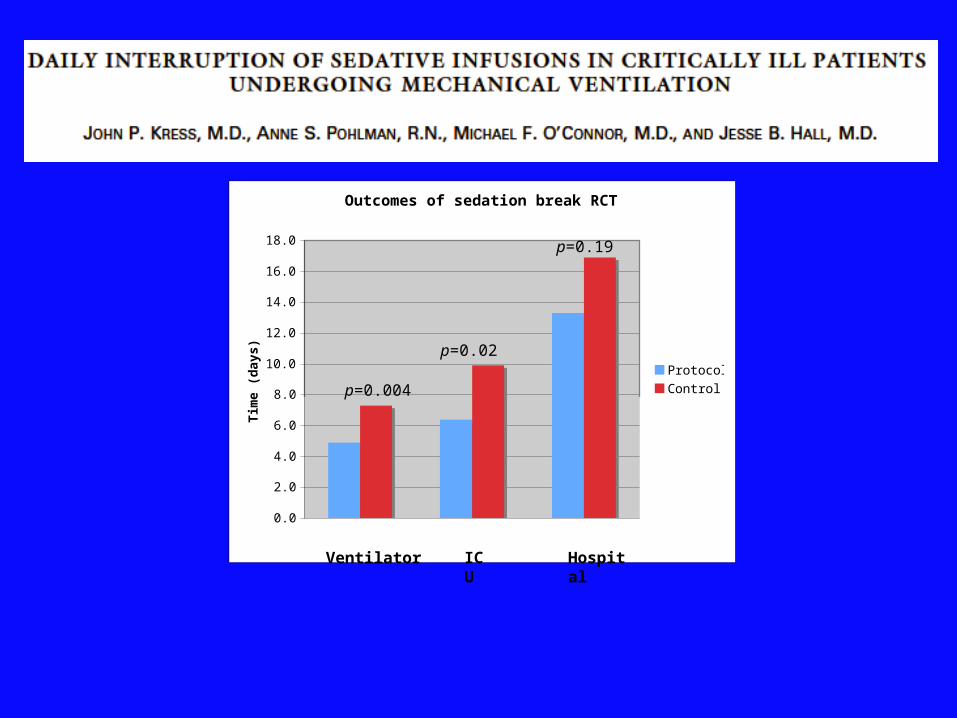
Outcomes of sedation break RCT
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0Tim
e (
days)
ProtocolControl
Ventilator ICU Hospital
p=0.004
p=0.02
p=0.19
Effect of a nursing-implemented sedation protocol on the duration of mechanical ventilation.
Brook AD, Ahrens TS, Schaiff R et al Crit Care Med.1999;27:2609-15
321 ventilated patients
Randomised: nurse-led sedation protocol v. standard care
Outcomes: duration of ventilation, ICU & hospital stay

Outcomes of Sedation Protocol RCT
0.0
5.0
10.0
15.0
20.0
25.0
Ventilator days ICU days Hosp days
Du
rati
on
(d
ays)
Protocol
Control
Effect of a nursing-implemented sedation protocol on the duration of mechanical ventilation.
Brook AD, Ahrens TS, Schaiff R et al Crit Care Med.1999;27:2609-15
P=0.003 P=0.013
P<0.001

300 ventilated patients
Randomised: daily weaning trial v. standard care
Outcomes: duration of ventilation, ICU & hospital stay


RCT of protocol-directed v. physician-directed weaning from mechanical ventilation.
Kollef MH, Shapiro SD, Silver P et al. Crit Care Med. 1997; 25:567-74

RCT of protocol-directed v. physician-directed weaning from mechanical ventilation.
Kollef MH, Shapiro SD, Silver P et al. Crit Care Med. 1997; 25:567-74


Avoiding VentilationAvoiding Ventilation
• Daily sedation titration and weaning protocols will reduce ventilator days and ICU stay
• VAP may be less common

• 86 ventilated patients• VAP in
23% supine patients
(28.4/1000 Vent d)
v.
5% semi-recumbent
(7.3/1000 Vent d)
NNT (95%CI) = 6 (3-23)

Study group Semi-recumbent n = 112
Standardn = 109
Average bed elevationDay 1Day 7
28.1o
22.6o
9.8o
16.1o
VAP 11.6%
10.2/1000 Vent d
7.3%
7.8/1000 Vent d
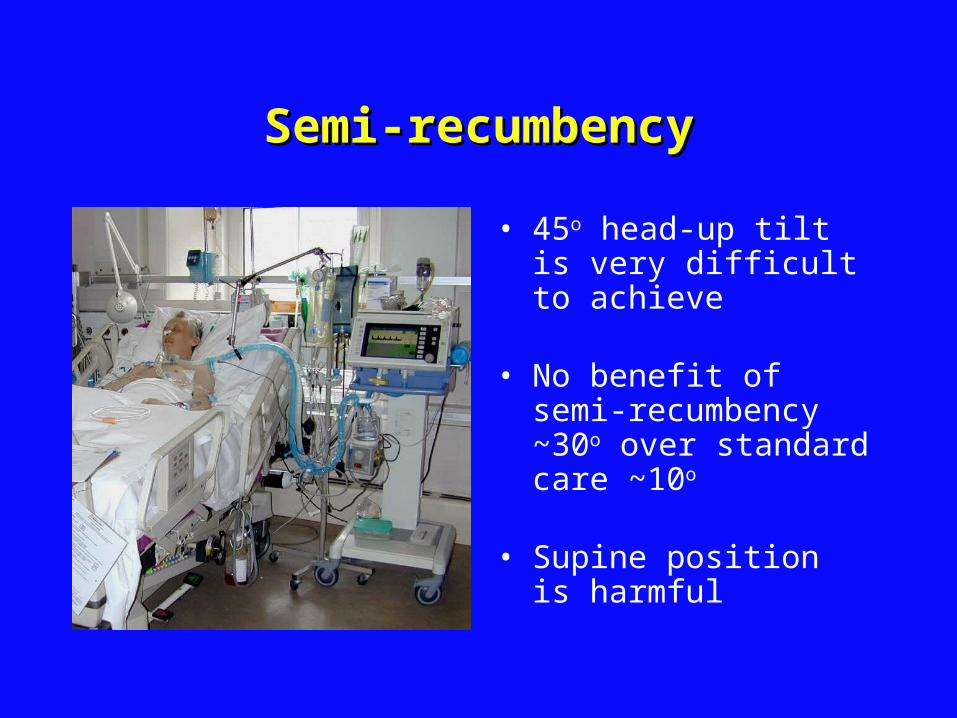
Semi-recumbencySemi-recumbency
• 45o head-up tilt is very difficult to achieve
• No benefit of semi-recumbency ~30o over standard care ~10o
• Supine position is harmful
Oro-pharyngeal AntisepticsOro-pharyngeal Antiseptics



Crit Care Med 2007; 35:595–602


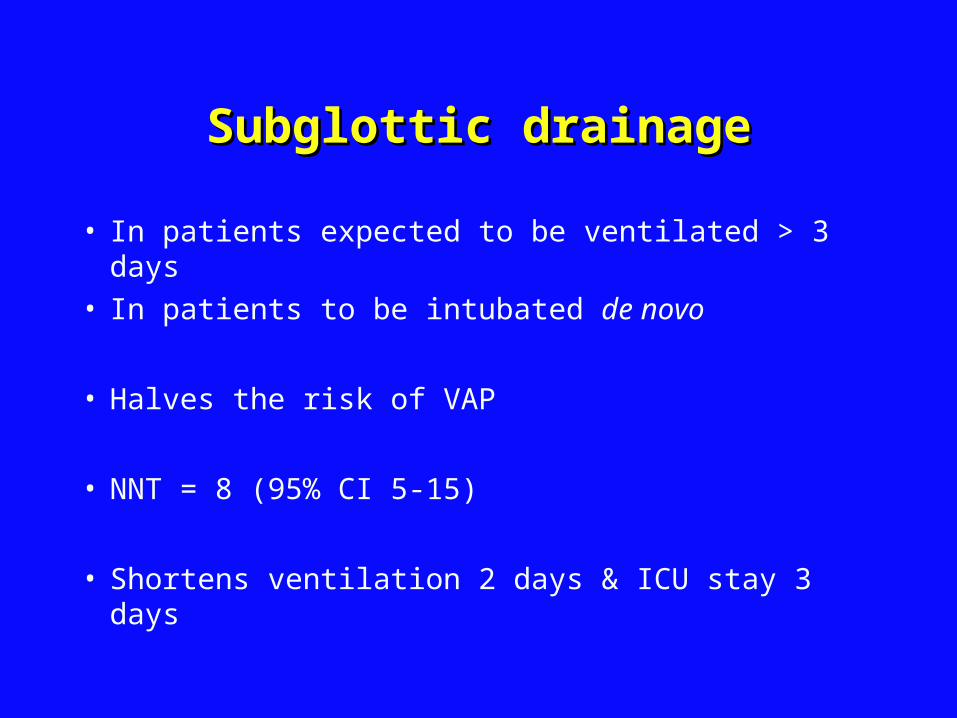
Subglottic drainageSubglottic drainage
• In patients expected to be ventilated > 3 days• In patients to be intubated de novo
• Halves the risk of VAP
• NNT = 8 (95% CI 5-15)
• Shortens ventilation 2 days & ICU stay 3 days

Prevent VAP Care BundlePrevent VAP Care Bundle
• Assess sedation requirements daily• Assess suitability for weaning and extubation daily
• Semi-recumbent position• Oral chlorhexidine • ? Subglottic drainage

Do VAP prevention programmes Do VAP prevention programmes work?work?
Effect of an education program aimed at reducing the occurrence of ventilator-associated pneumonia. Zack JE et al Crit Care Med 2002; 30: 2407-12
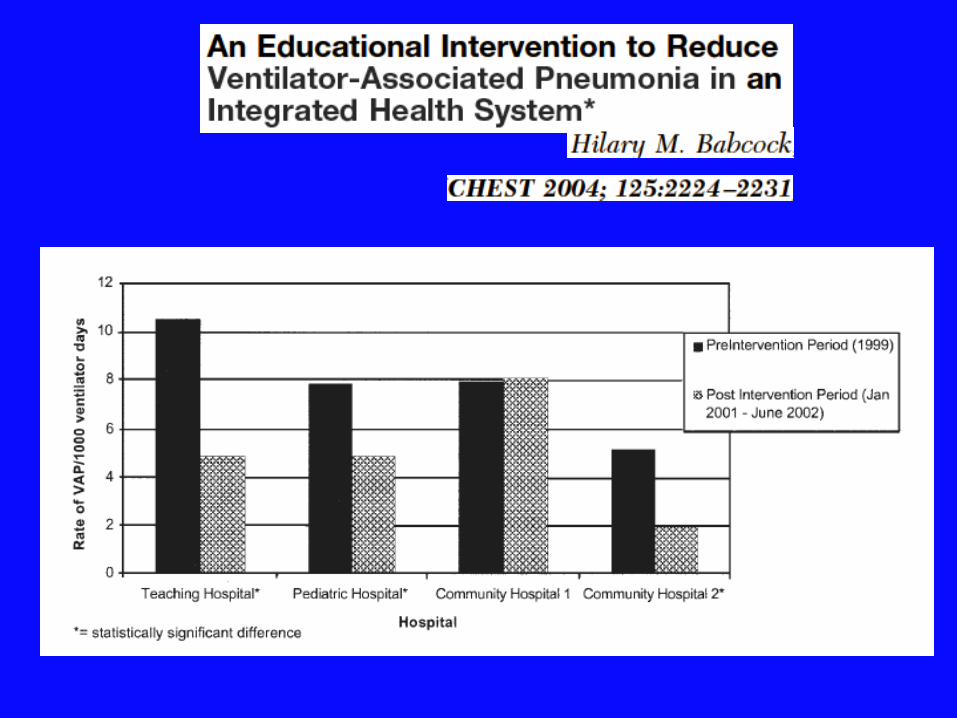
An educational intervention to reduce VAP in an integrated health system: a comparison of effects.Babcock HM et al Chest 2004; 125: 2224-31
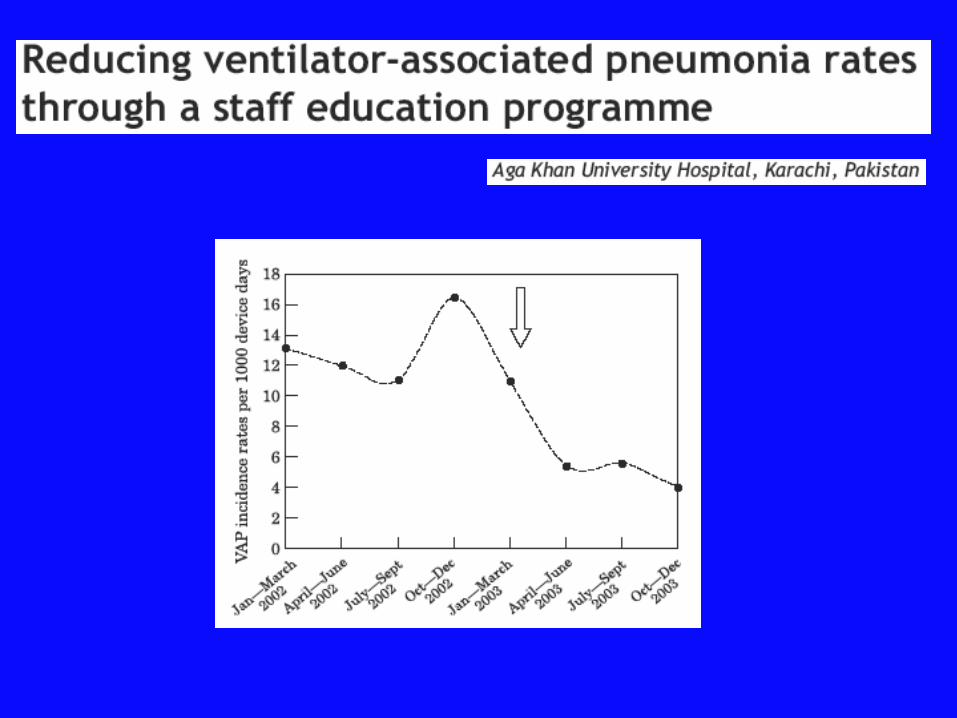
Reducing VAP rates through a staff education programme.Salahuddin N et al J Hosp Infect. 2004; 57 :223-7
Adherence to simple and effective measures reduces the incidence of VAP.Baxter AD et al Can J Anaesth. 2005; 52: 535-41

54
Rate per 1000 ventilator days
VAP in five ICUs at BarnesVAP in five ICUs at Barnes ––JewishJewishhospital: October 1999hospital: October 1999––September 2001September 2001
20
0
5
10
15
Oct1999
Dec Feb Apr Jun Aug Oct Dec Feb Apr Jun Aug
Interventionrespiratory therapy
2000 2001
Mean
NNISa
Zack et al. Crit Care Med 2002;30:2407 –2412a National Nosocomial Infection Surveillance (NNIS) data

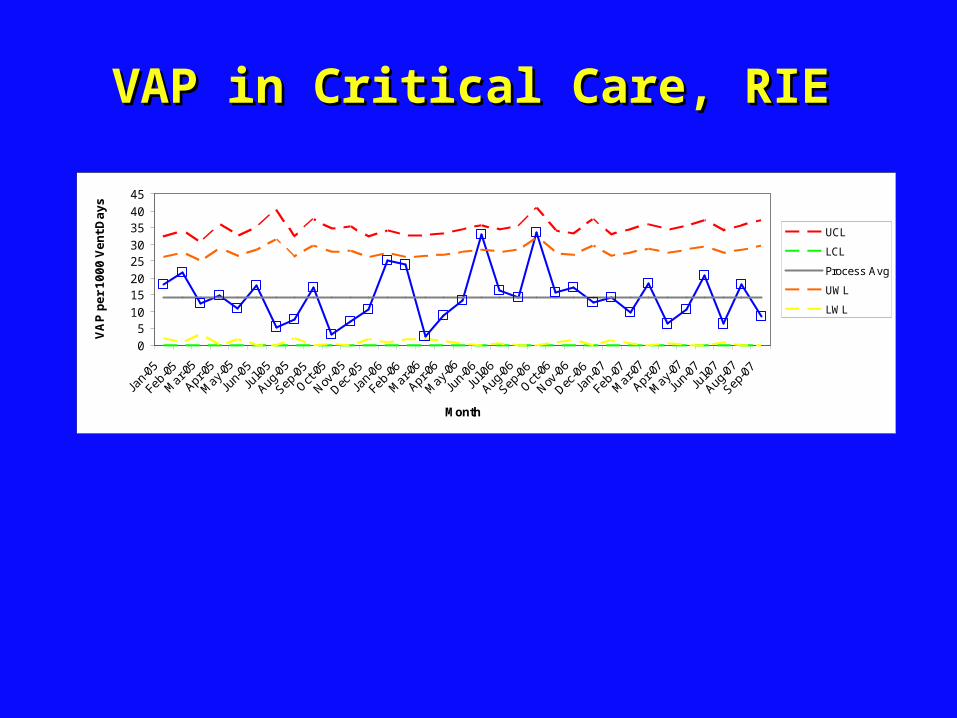
VAP in Critical Care, RIEVAP in Critical Care, RIE
0
510
1520
2530
3540
45
Month
VA
P p
er
10
00
Ve
nt
Da
ys
UCL
LCL
Process Avg
UWL
LWL

ConclusionConclusion
• There is reasonable evidence from RCTs and their metanalyses to support the elements of the proposed ‘ Prevent VAP Care Bundle’
• Other groups have halved VAP rates through education programmes, reinforcing adoption of protocols to prevent VAP
Top Related