






Languages
Pages
Legal

Preterm Birth
Present by:Dr.Worapa Asavaritikrai Health Promotion Center Region 4

Objective
• Definition
• Risk factors
• Diagnosis
• Treatment
Definition of Preterm Birth
• 37A birth that occurs before compppppp peepp pp ppppppppp (<259 days)
• Late preterm births, defined as 34-36+6 weeks of gestation (~ 75% of all preterm birth)
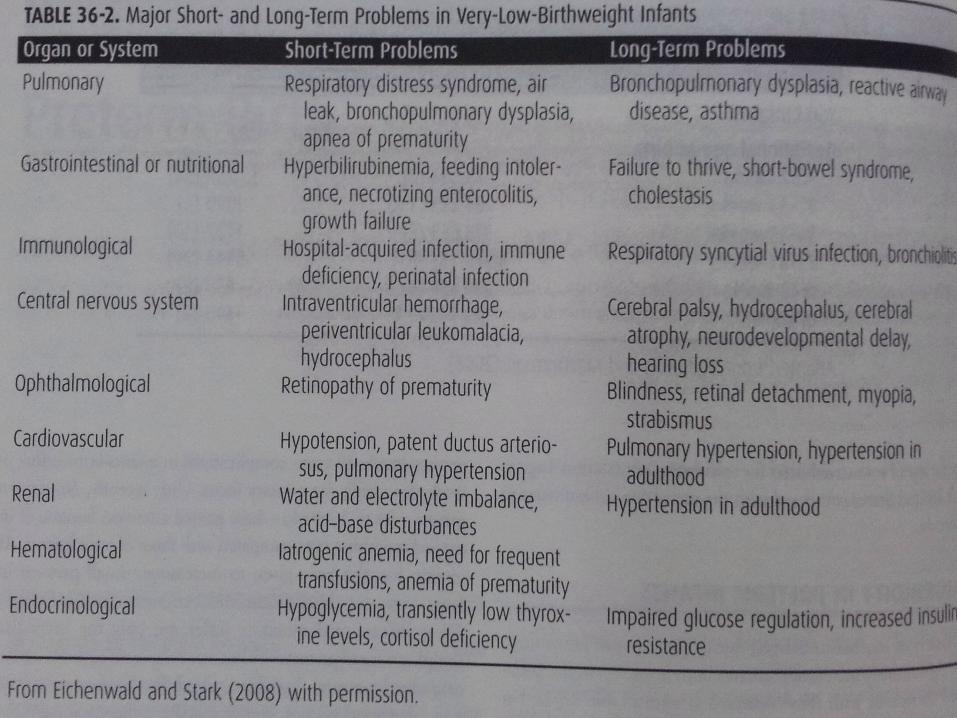
36-2
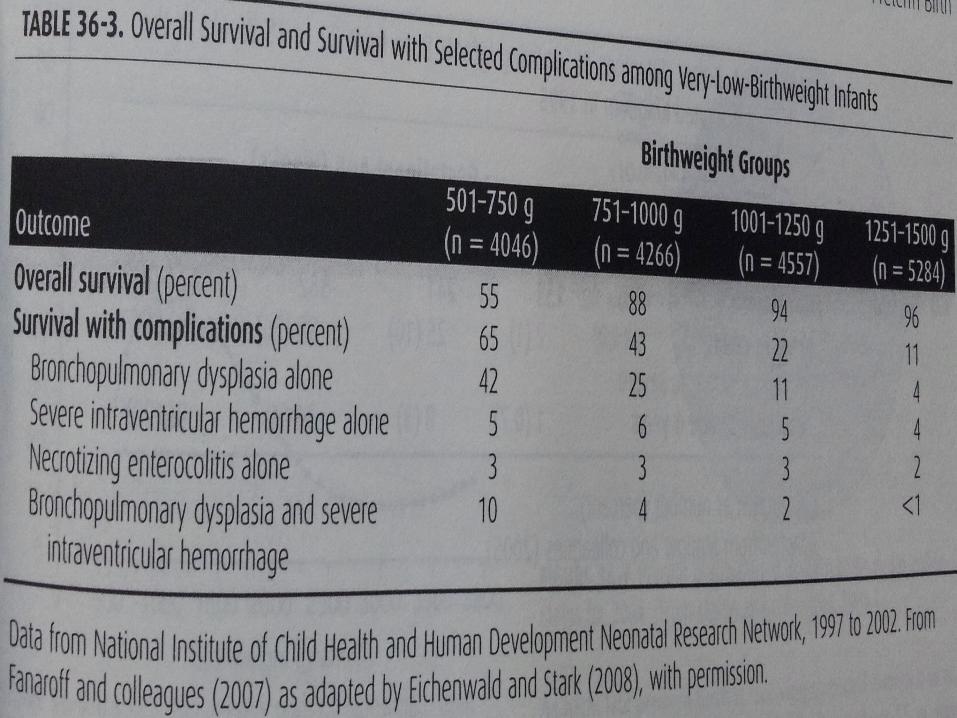
36-3

SURVIVAL RATE OF INFANTS
RAMATHIBODI HOSPITAL (2000-2008)

36-8
Reasons for preterm delivery
• 4 main direct reasons:– Maternal or fetal indications– Spontaneous unexplained preterm labor
with intact membranes– Idiopathic preterm premature rupture of
membranes (PPROM)– Twins
Cunningham et al, 23rd Ed Williams Obstetrics

Definition of PPROM
• Defined as rupture of the membranes before labor and prior to 37 wee ks of gestation
Antecedents & Contributing Factors
• Threatened Abortion• Lifestyle Factors• Racial & Ethnic Disparity• Work During Pregnancy• Genetic Factors• Periodontal Disease
Antecedents & Contributing Factors
• Birth Defects• Interval between Pregnancies & Preterm
Birth• Prior Preterm Birth• Infection• Bacterial Vaginosis
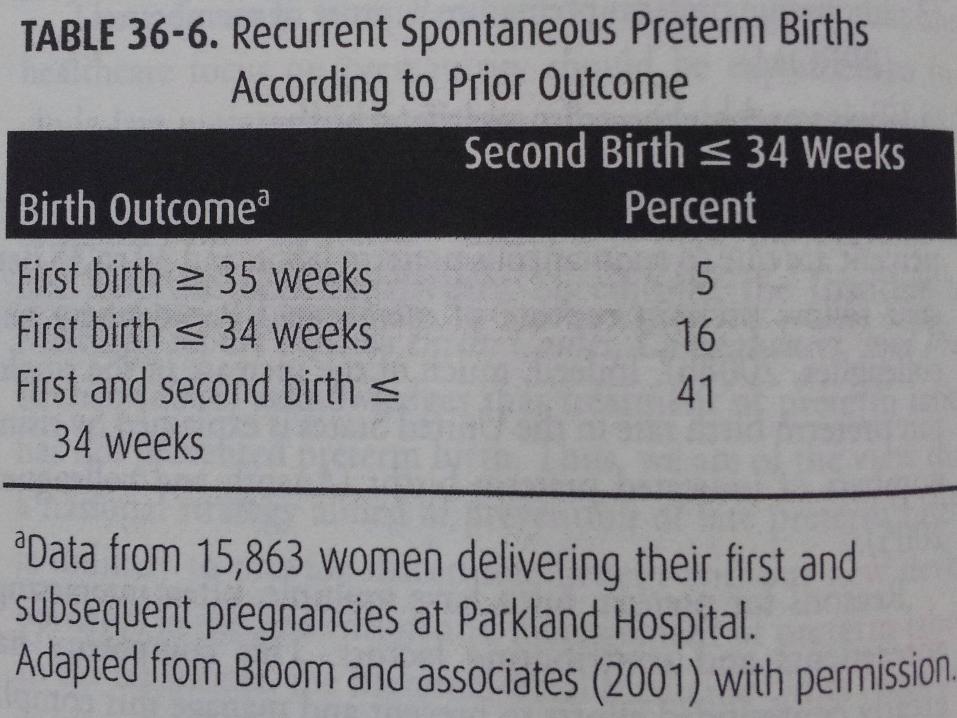
Table 36-6

36-10

ร่�างแผนการ่ดู�แลการ่เจ็�บคร่ร่ภ์�คลอดูก�อนก�าหนดู
Clinical Practice Guidelinen of Preterm labor
Prevention of preterm birth
• Primary Prevention• Secondary Prevention• Tertiary Prevention
Preventions of Preterm Birth

Primary Prevention

Preconceptional
• Public educational interventions: – Increased awareness– Uterine curettage or endometrial biopsy– Reduce prevalence of smoking– Reduce risk of higher-order multiple
gestation– Socioeconomic approach
During Pregnancy
Smoking cessation in pregnancyPrenatal carePeriodontal care ?? Screening of low-risk women
Smoking cessation
A Cochrane review reported that smoking cessation programmes in pregnancy successfully reduce the incidence of preterm birth (RR 0·84, CI 0·72–0·98)
Lumley J.Cochrane Database Syst Rev 2004
Prenatal Care
High rate of preterm birth in women who receive no prenatal care than from the content of care for those who receive it

Periodontal care
Treatment during pregnency improved periodontal disease and it is safe, but it did not significantly alter rate of preterm birth
Michalowicz BS. N Engl J Med 2006; 355: 1885–94
Screening of low-risk women
-Screening and treatment of asymptomatic bacteriuria prevent pyelonephritis
-Given antibiotic in low-risk does not reduce this risk of preterm birth
Cunningham et al, 23rd Ed Williams Obstetrics
Secondary Prevention

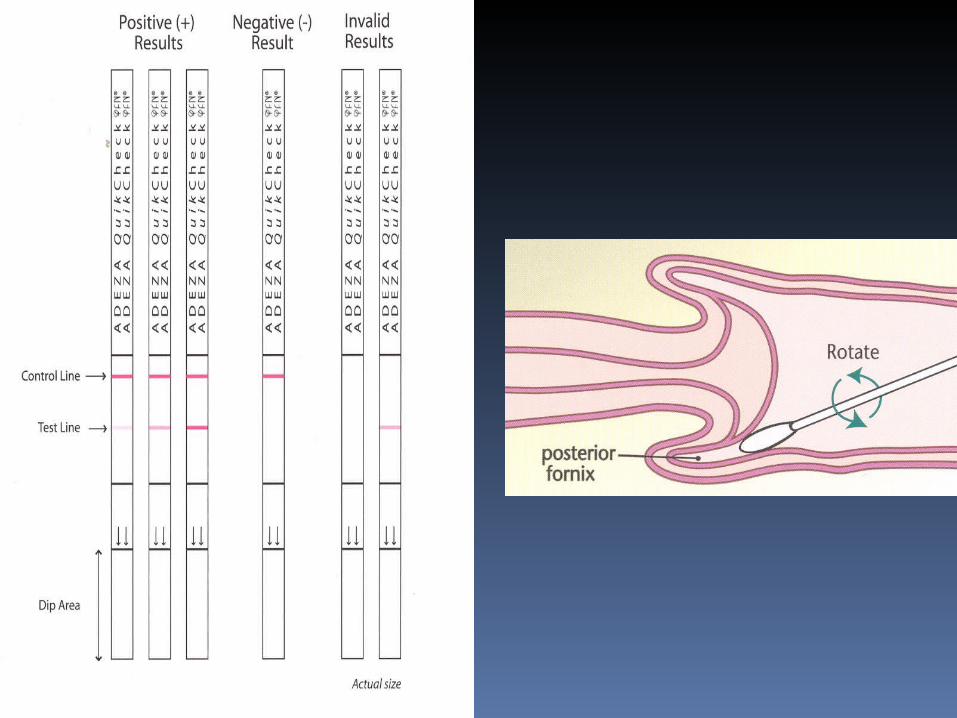
Fetal fibronectin testing
• Glycoprotein • Marker of choriodecidual disruption• Levels > 50 ng/mL ( >22 weeks) associated
with an increased risk of spontaneous preterm birth
The Cochrane Library 2009, Issue 2
Cervical length
• Cervical shortening is a risk factor for preterm delivery
• Especially useful in asymptomatic women : at 24 wks, a cervical length < 25 mm
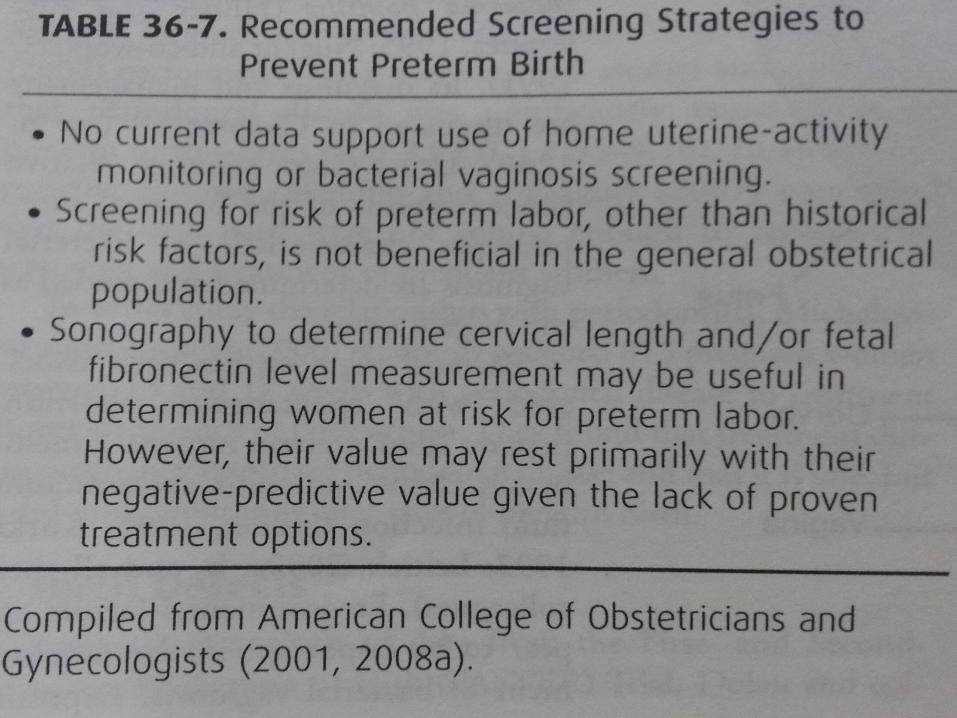
Table 36-7

Tertiary Prevention
Tertiary Prevention
• Early diagnosis of preterm labour• Treatment of women with acute risk of
preterm birth to arrest preterm labour : tocolysis antenatal corticosteroid use antibiotic for group B streptococcal
prophylaxis

• Regular contractions accompanied by cervical change at less than 37 weeks
• ACOG 1997 criteria preterm labor:– Contractions of four in 20 min. or eight
in 60 min. + progressive change in the cervix
– Cervical dilatation > 1 cm – Effacement > 80%.
Diagnosis of preterm labor
Regular contractions without cervical
change
Threatened preterm labor
Management of Preterm Labor
• PPROM• Preterm labor with intact membranes
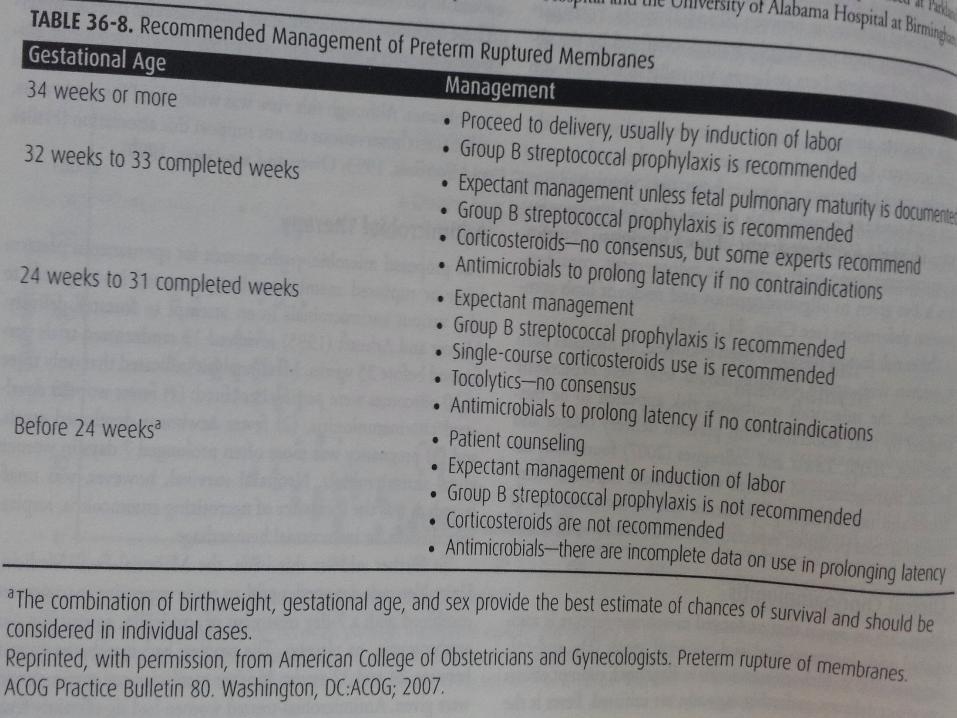
Table 36-8
Tocolytic agents
• ACOG 2007 has concluded that tocolytic agents do not markedly prolong gestation, but may delay delivery in some women for at least 48 hours
Tocolytic agents
• Β-Adrenergic receptor agonists– Ritodrine, Terbutaline
• Magnesium sulfate• Prostaglandin inhibitors• Calcium-channel blockers• Atosiban• Nitric oxide donors

Terbutaline
Dose CI Maternal SE Fetal SE
0.25 mg SC every 20 min to 3 h (hold for P>120 bpm)
Cardiac arrhythmia, poorly control thyrotoxicosis or DM
Cardiac arrhythmia, pulmonary edema, MI, hypotension, hyperinsulinemia, antidiuresis, hypokelemia,
Tachycardia, hyperinsulinemia, hyperglycemia, neonatal hypoglycemia, hypocalcemia, hypotesion, myocardial and septal hypertrophy, MI
Hearne AE, Nagey DA. Therapeutic agents in preterm labor: tocolytic agents. Clin Obstet Gynecol 2000;43:787-801
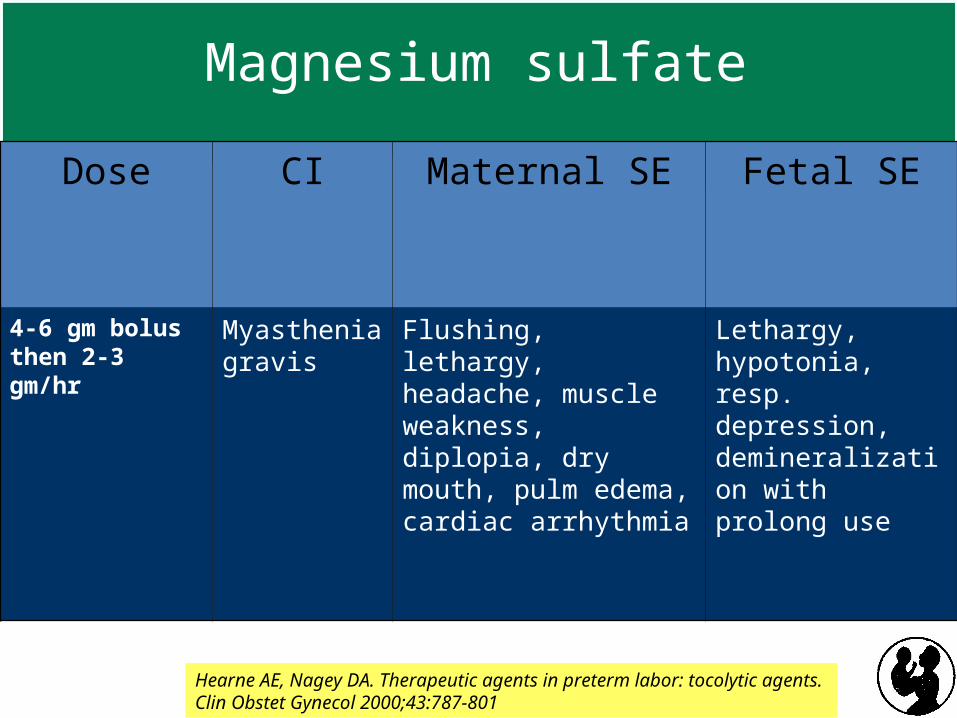
Magnesium sulfate
Dose CI Maternal SE Fetal SE
4-6 gm bolus then 2-3 gm/hr
Myasthenia gravis
Flushing, lethargy, headache, muscle weakness, diplopia, dry mouth, pulm edema, cardiac arrhythmia
Lethargy, hypotonia, resp. depression, demineralization with prolong use
Hearne AE, Nagey DA. Therapeutic agents in preterm labor: tocolytic agents. Clin Obstet Gynecol 2000;43:787-801
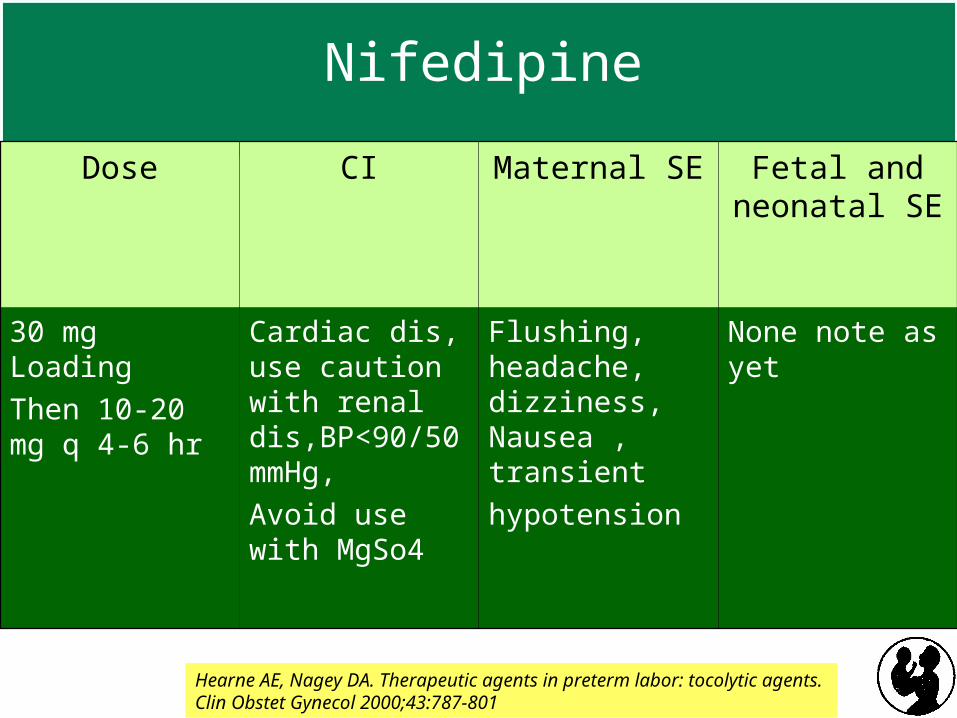
Nifedipine
Dose CI Maternal SE Fetal and neonatal SE
30 mg Loading
Then 10-20 mg q 4-6 hr
Cardiac dis, use caution with renal dis,BP<90/50mmHg,
Avoid use with MgSo4
Flushing, headache, dizziness, Nausea , transient
hypotension
None note as yet
Hearne AE, Nagey DA. Therapeutic agents in preterm labor: tocolytic agents. Clin Obstet Gynecol 2000;43:787-801
Corticosteroid Therapy
• Enhance fetal lung maturation• Rescue therapy?• Betamethasone is superior to Dexamethasone• Regimens:
– Two doses of Betamethasone 12 mg IM q 24 hrs
– Four doses of Dexamethasone 6 mg IMq 12 hrs
• Goal is neonatal sepsis preventionGoal is neonatal sepsis prevention• Not to prevent preterm birthNot to prevent preterm birth
Group B streptococcus prophylaxis

Group B streptococcus prophylaxis
Centers for Disease Control and Prevention, 2002d

Cunningham et al, 23rd Ed Williams Obstetrics
Recommended Management of Preterm
Labor
• Confirmation of preterm labor• GA <34 weeks: corticosteroids are given for
enhancement of fetal lung maturation• GA <34 weeks: reasonable to attempt
inhibition of contractions to delay delivery while given corticosteroid & group B streptococcal prophylaxis
• GA >34 weeks: monitor for labor progression & fetal well-being

Thank You
Top Related