







Languages
Pages
Legal

Physical Examinationof the Shoulder
James A. Tom, MDSports Medicine and Shoulder Dept. of Orthopaedic Surgery
Drexel University College of MedicinePhiladelphia, PA
Evaluation of the Shoulder
• Thorough history of presenting complaint• Information regarding surrounding anatomy
• Neck• Elbow• Chest• Diaphragm
• Imaging studies based on clinical suspicion• Not simply ordered “to make the diagnosis”
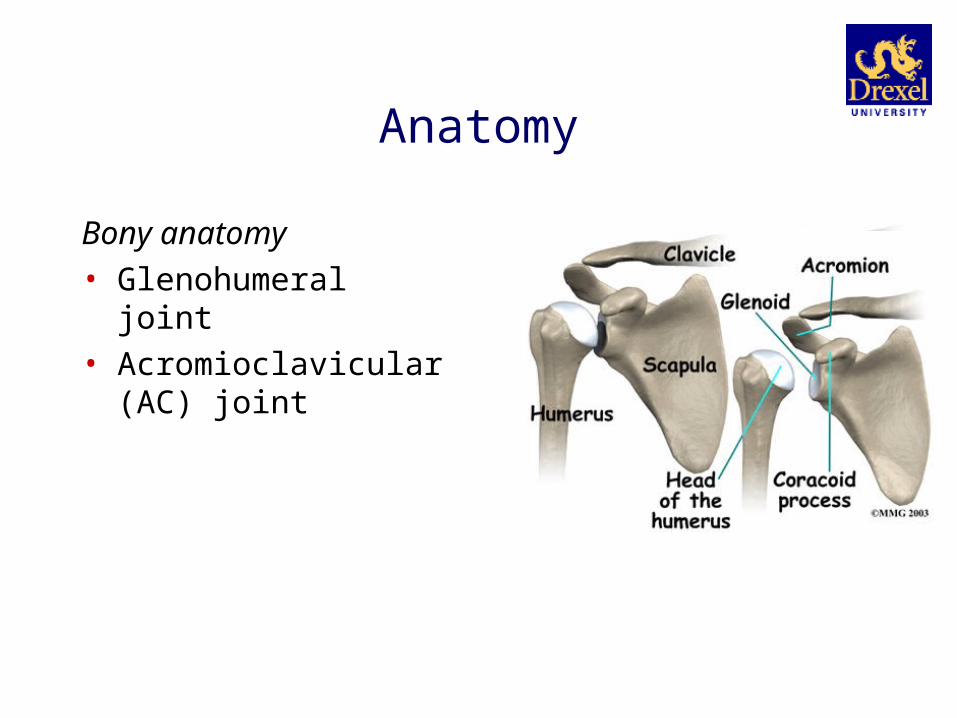
Anatomy
Bony anatomy• Glenohumeral joint• Acromioclavicular (AC) joint
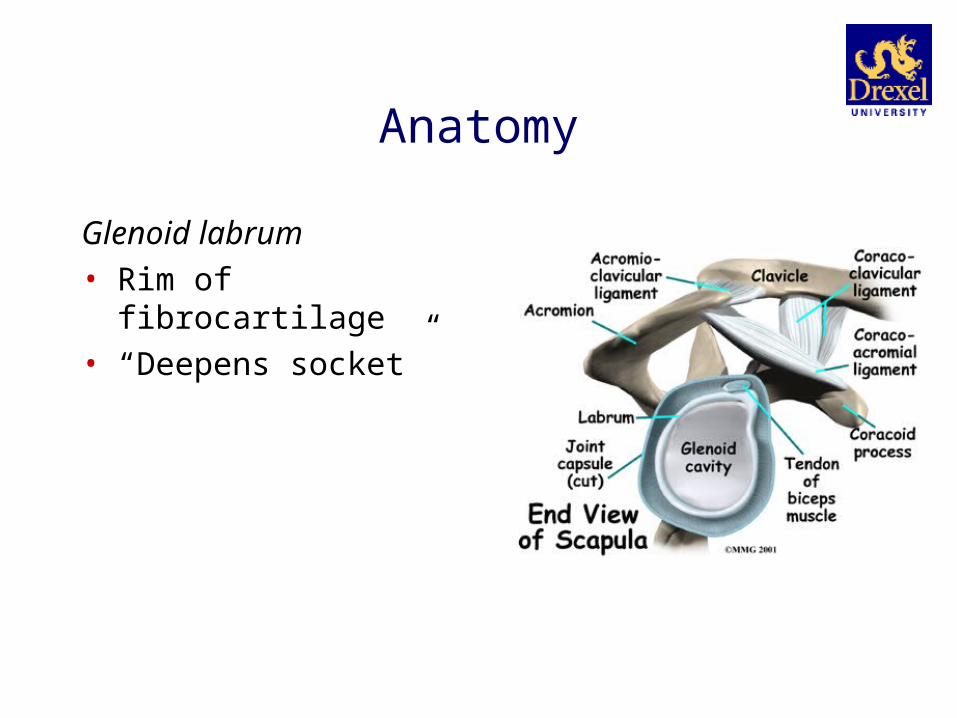
Anatomy
Glenoid labrum• Rim of fibrocartilage• “Deepens socket”

Anatomy
Joint capsule
Anatomy
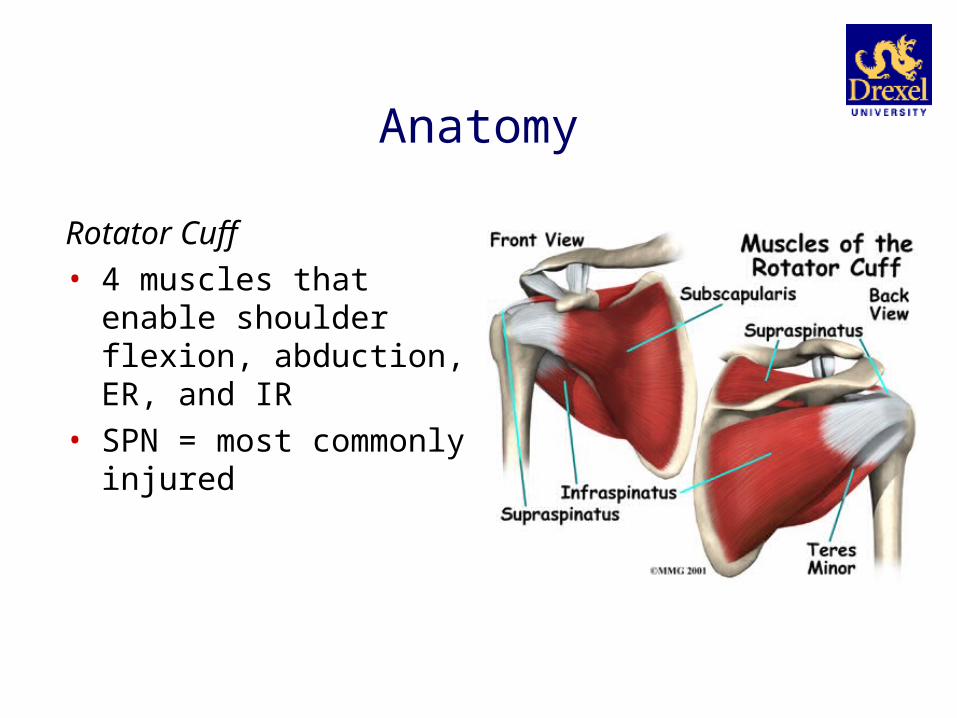
Rotator Cuff• 4 muscles that enable shoulder
flexion, abduction, ER, and IR• SPN = most commonly injured
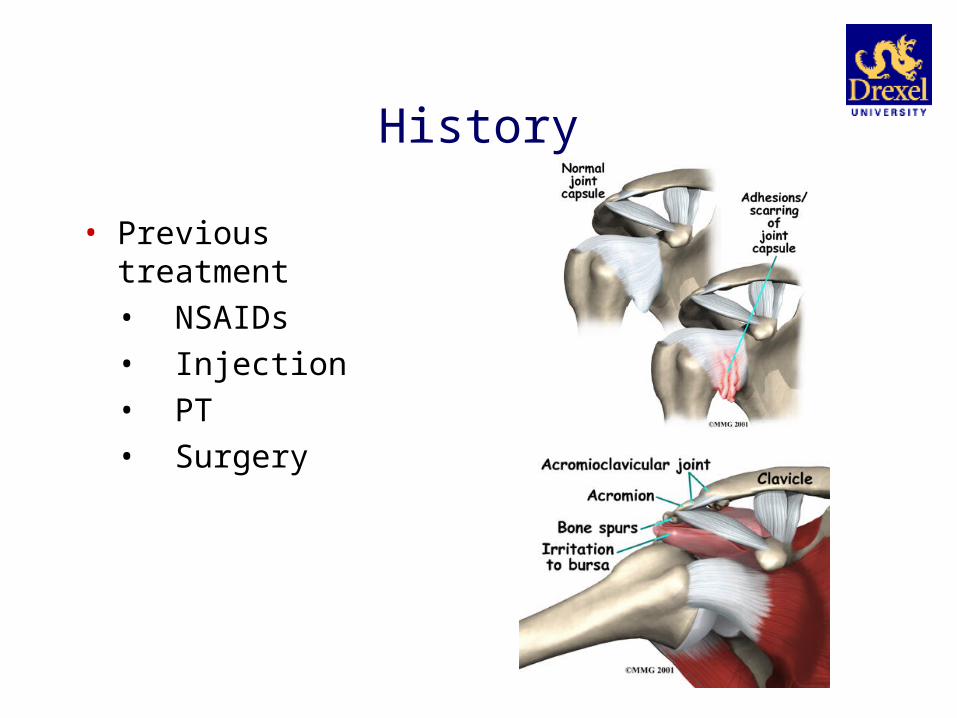
History
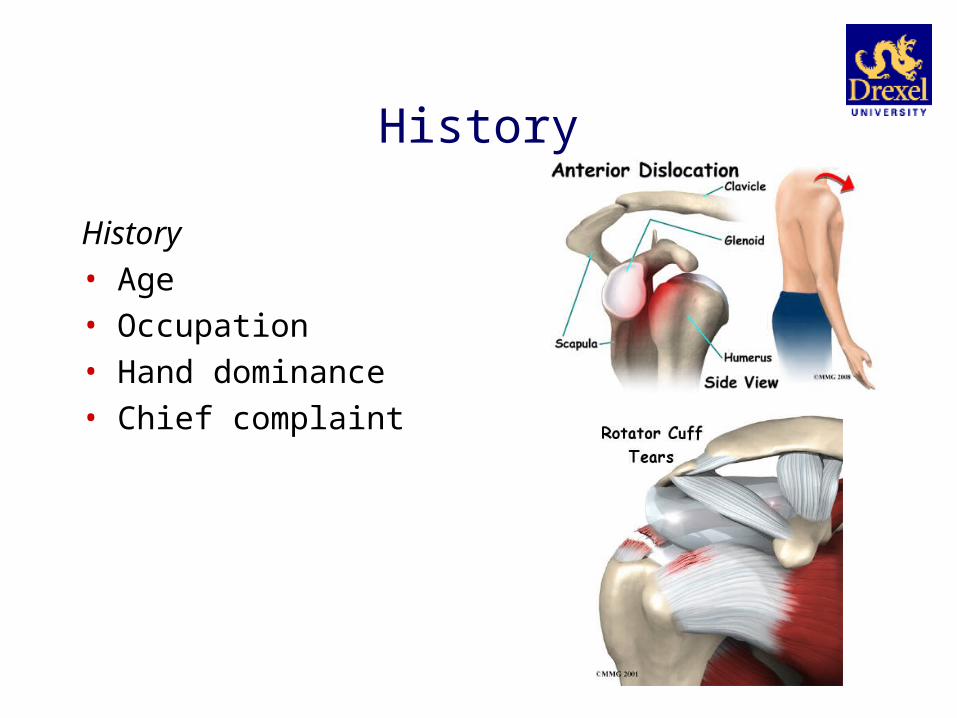
History• Age• Occupation• Hand dominance• Chief complaint
History
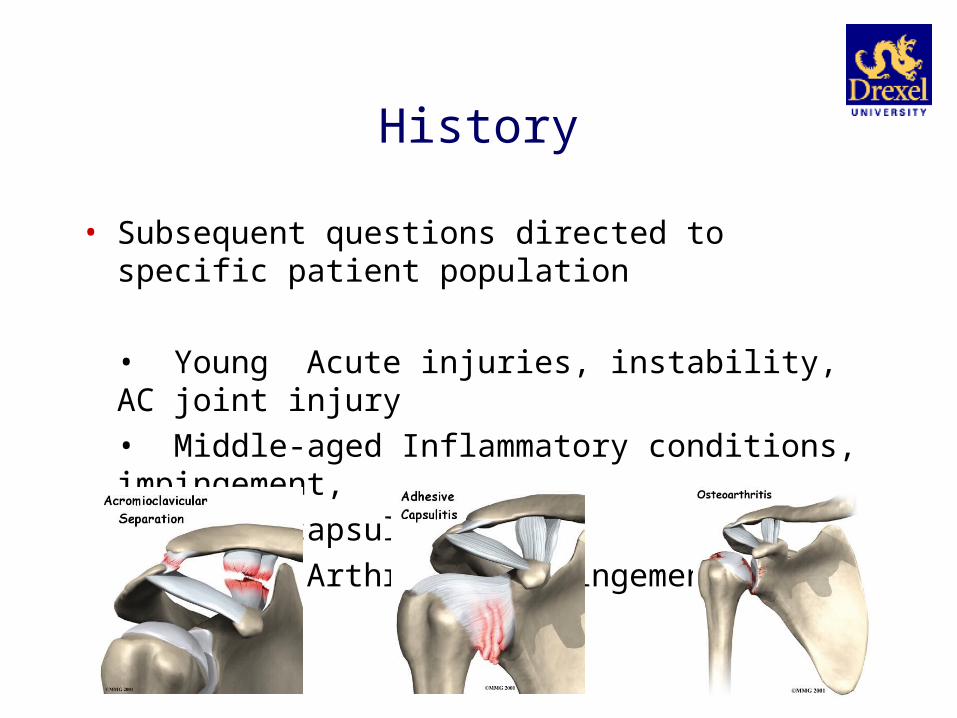
• Subsequent questions directed to specific patient population
• Young Acute injuries, instability, AC joint injury• Middle-aged Inflammatory conditions, impingement,
adhesive capsulitis• Older Arthritis, impingement, RTC pathology

History
• History of injury• Acute• Chronic
• Mechanism of injury (MOI)• Secondary gain
• Litigation• Worker’s Compensation• Psychiatric illness

History
• Pain• Character• Location• Intensity• Duration• Radiation• Factors associated with exacerbation / relief• Interference with work /
daily activities (ADLs)
• Objective measuresVASValidated scoring
systems
History
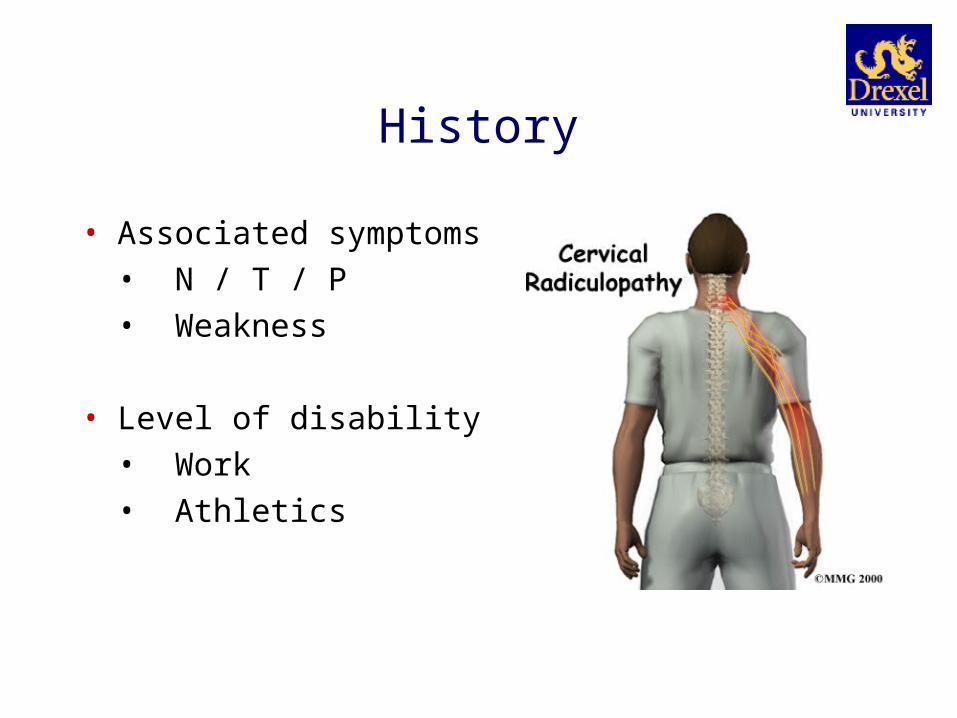
• Associated symptoms• N / T / P• Weakness
• Level of disability• Work• Athletics
History
• Previous treatment• NSAIDs• Injection• PT• Surgery
Physical Exam
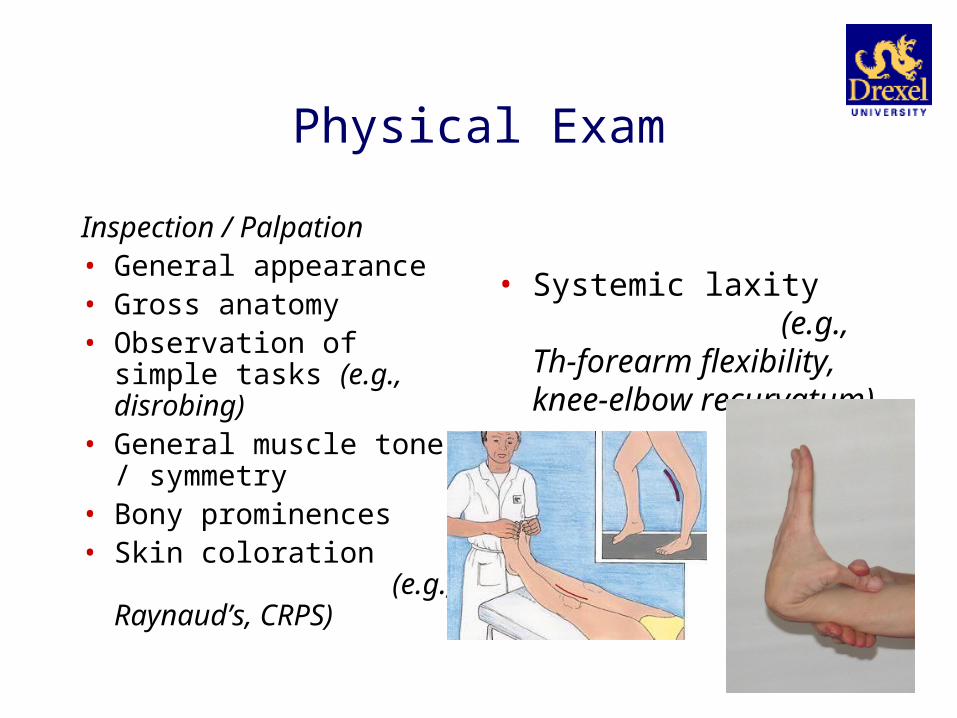
Inspection / Palpation• General appearance• Gross anatomy• Observation of simple tasks
(e.g., disrobing)• General muscle tone /
symmetry• Bony prominences• Skin coloration
(e.g., Raynaud’s, CRPS)
• Systemic laxity (e.g., Th-forearm flexibility, knee-elbow recurvatum)
Physical Exam
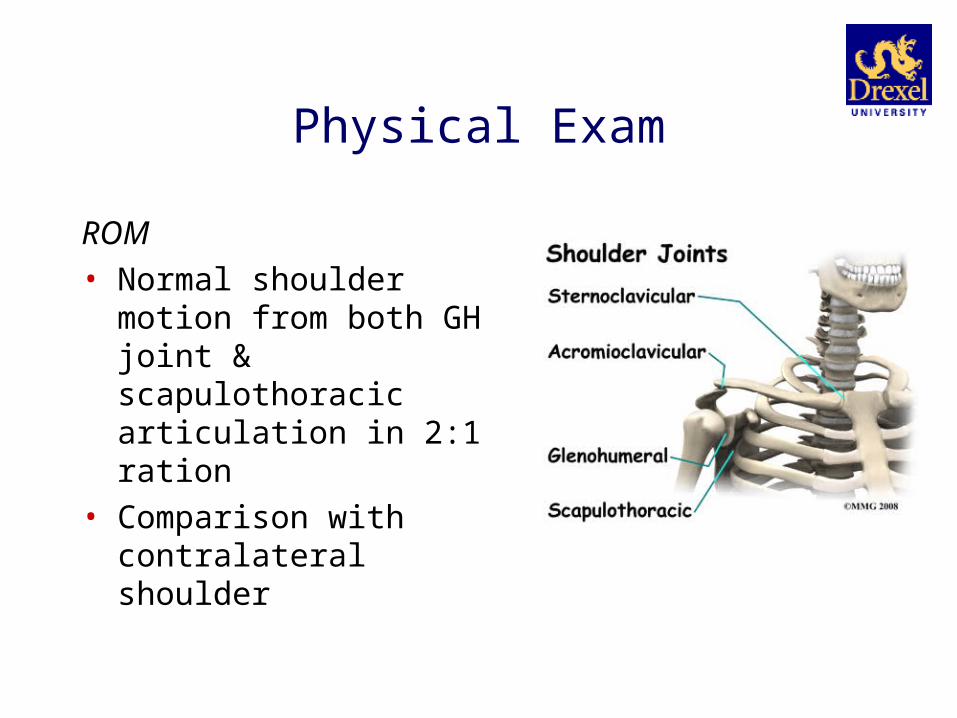
ROM• Normal shoulder motion from
both GH joint & scapulothoracic articulation in 2:1 ration
• Comparison with contralateral shoulder

Physical Exam
• Active / Passive ROM• Discrepancy indicative of
specific disease
• Abduction 180° Adduction 45°
Flexion 180° Extension 45° IR 55° ER 45°

Physical ExamStrength• Graded system of manual muscle testing• Objective description of strength
• 5/5 FROM vs. gravity & full resistance4/5 FROM vs. gravity & some resistance3/5 FROM vs. gravity but no resistance2/5 FROM at gravity neutral1/5 Muscle contracts but no motion0/5 Muscle unable to contract
• Neurologic problem or muscle injury

Impingement
Neer’s impingement sign• Subacromial impingement• Passive FE of arm
impingement of SPN tendon under CA arch
• (+) test = reproduction of pain

Impingement
Not Neer’s impingement test• Subacromial injection with local
anesthestic• Most sensitive / specific test for
impingement
• (+) = pain relief after injection

Impingement
Hawkin’s impingement sign• Subacromial impingement• Adducted shoulder flexed
forward to 90° with IR
• (+) test = reproduction of pain

Rotator Cuff Tear
SPN stress test• ~ “empty (beer / soda) can sign”• Supraspinatus tear• Resisted abduction of internally
rotated and forward flexed arm (in scapular plane)
• Performed in supination to eliminate sx of impingement
• (+) = pain and weakness
Rotator Cuff Tear
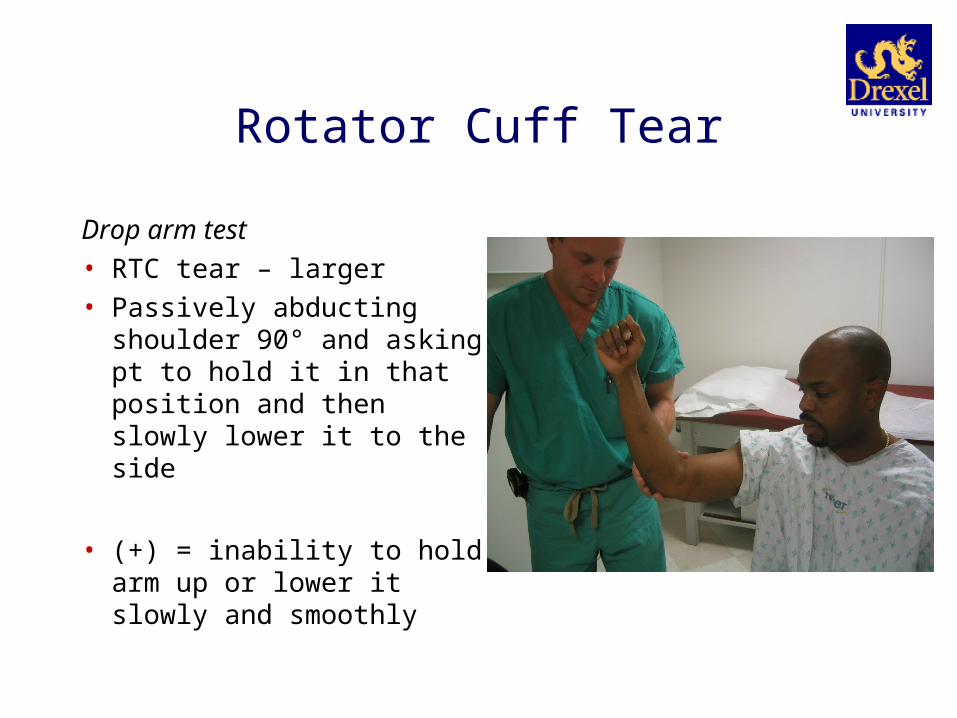
Drop arm test• RTC tear – larger• Passively abducting shoulder
90° and asking pt to hold it in that position and then slowly lower it to the side
• (+) = inability to hold arm up or lower it slowly and smoothly
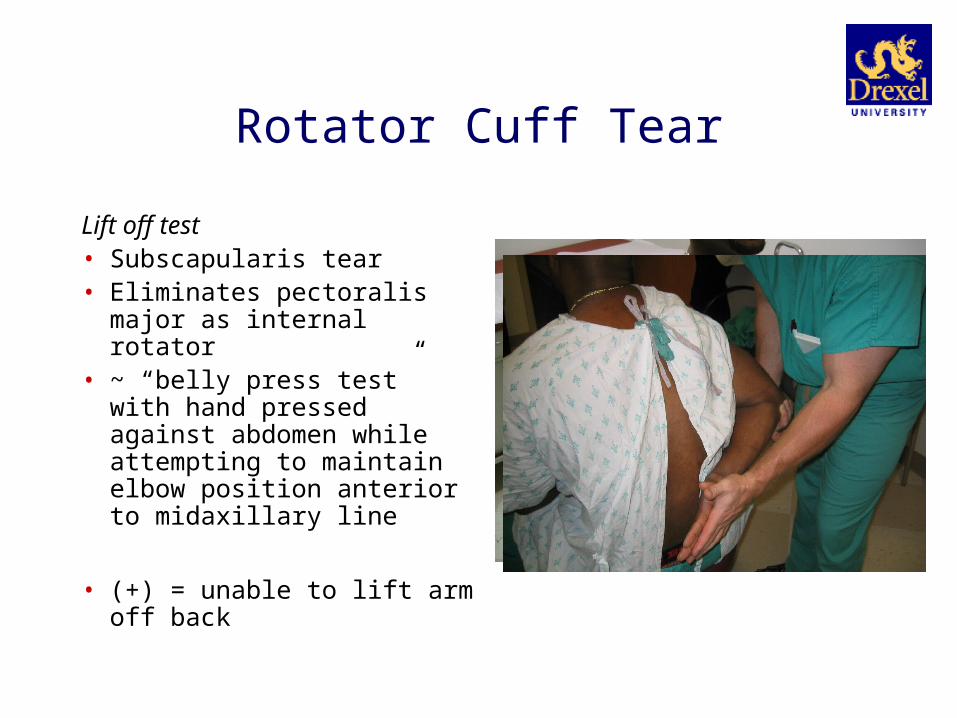
Rotator Cuff Tear
Lift off test• Subscapularis tear• Eliminates pectoralis major as
internal rotator• ~ “belly press test” with hand
pressed against abdomen while attempting to maintain elbow position anterior to midaxillary line
• (+) = unable to lift arm off back
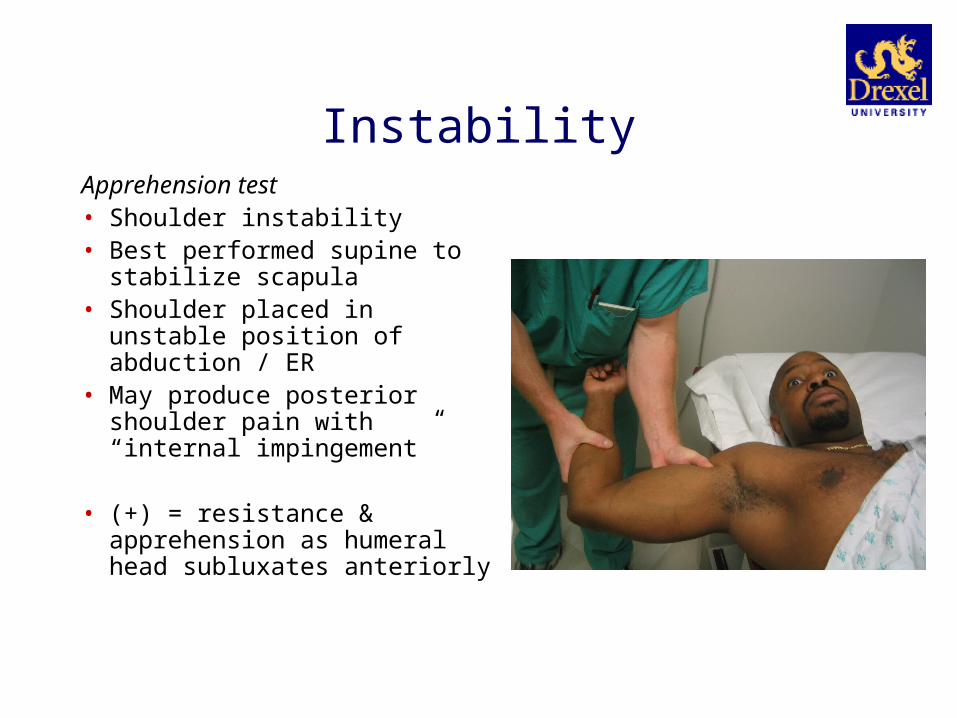
InstabilityApprehension test• Shoulder instability• Best performed supine to stabilize
scapula• Shoulder placed in unstable
position of abduction / ER• May produce posterior shoulder
pain with “internal impingement”
• (+) = resistance & apprehension as humeral head subluxates anteriorly
Instability
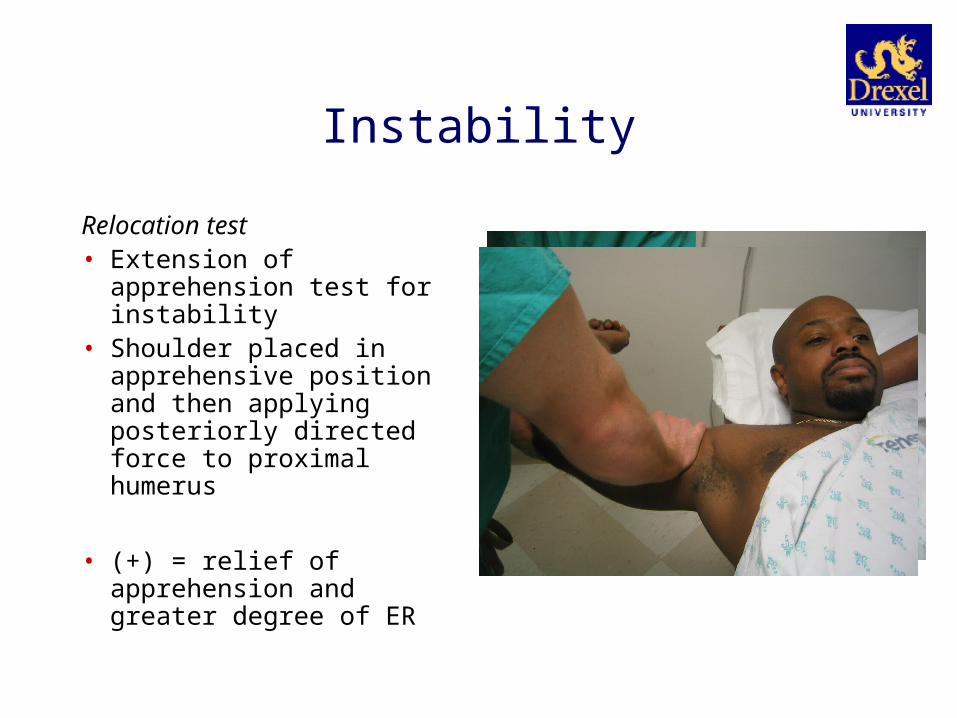
Relocation test• Extension of apprehension
test for instability• Shoulder placed in
apprehensive position and then applying posteriorly directed force to proximal humerus
• (+) = relief of apprehension and greater degree of ER
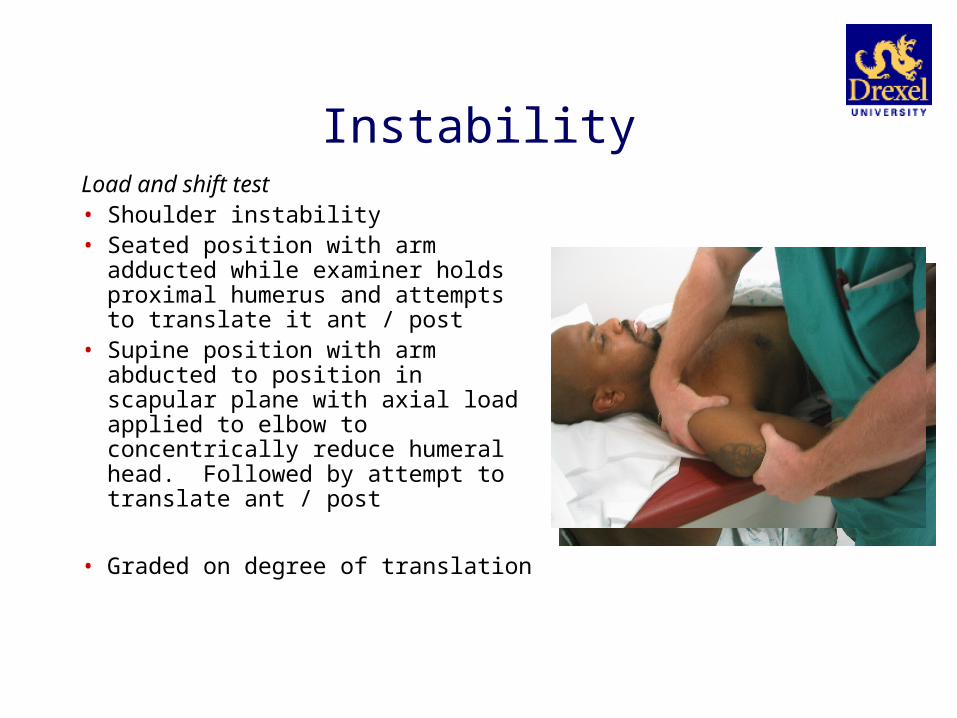
InstabilityLoad and shift test• Shoulder instability• Seated position with arm adducted
while examiner holds proximal humerus and attempts to translate it ant / post
• Supine position with arm abducted to position in scapular plane with axial load applied to elbow to concentrically reduce humeral head. Followed by attempt to translate ant / post
• Graded on degree of translation

Instability
Sulcus sign• Inferior shoulder laxity• Downward traction of arm as it
hangs at side (neutral rotation and neutral flex-ext)
• (+) = gap between humerus and acromion
Instability
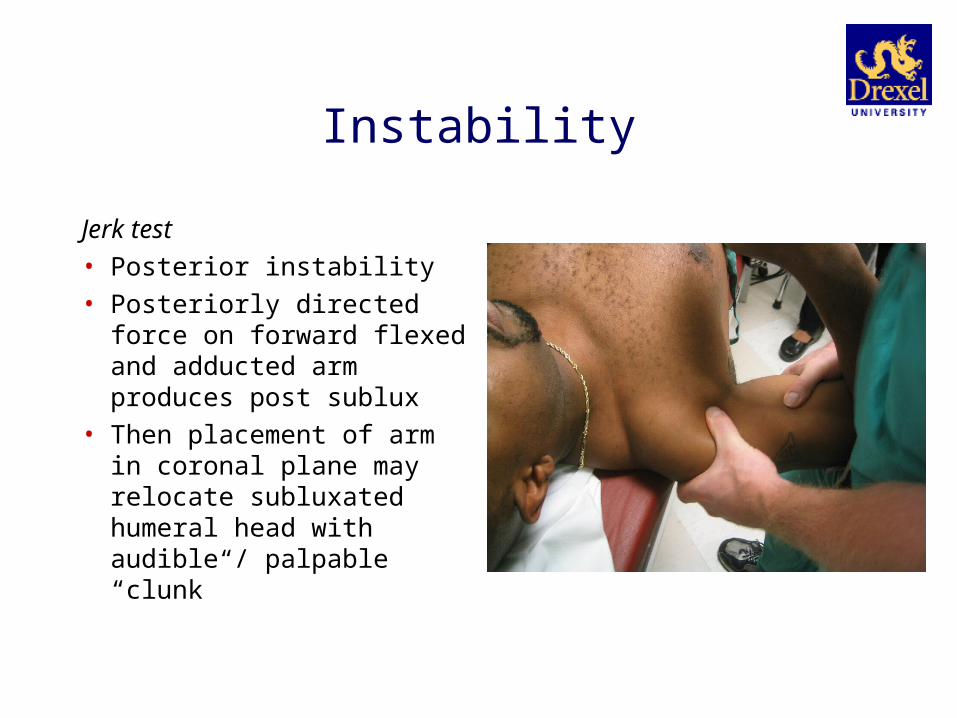
Jerk test• Posterior instability• Posteriorly directed force on
forward flexed and adducted arm produces post sublux
• Then placement of arm in coronal plane may relocate subluxated humeral head with audible / palpable “clunk”

Biceps Tendon Disease
O’Briens’s test• “Active compression test”• Superior labral – biceps pathology
(SLAP lesions)• Shoulder forward flexed 90° and
slightly adducted across body while elbow kept straight and arm internally rotated. Resists downward force on arm.
• (+) = reproduction of pain and relative relief with supination
Biceps Tendon Disease
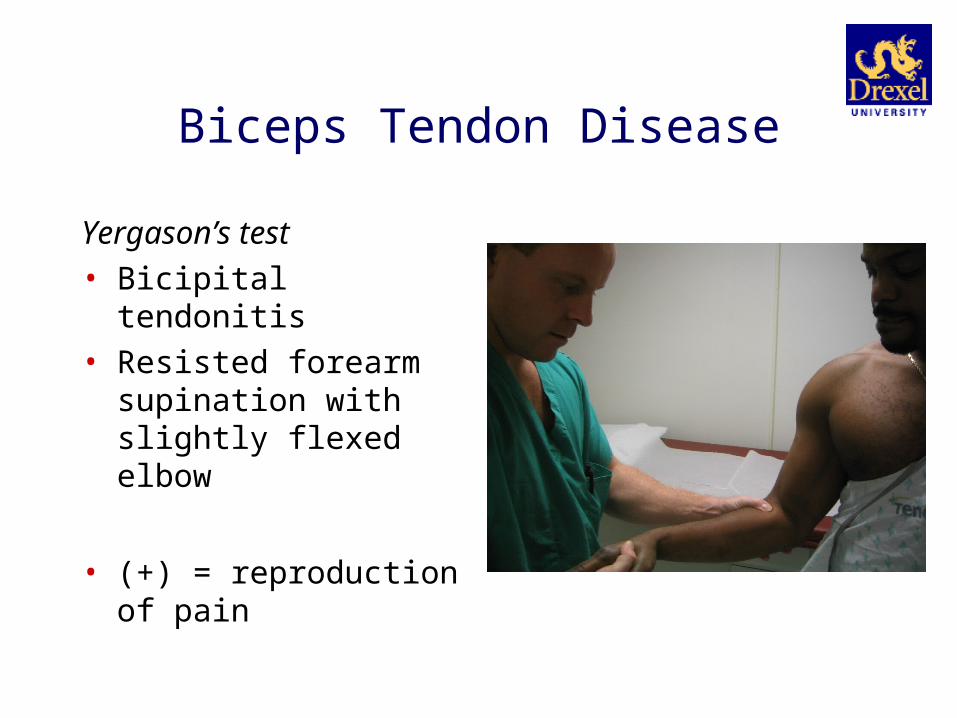
Yergason’s test• Bicipital tendonitis• Resisted forearm supination
with slightly flexed elbow
• (+) = reproduction of pain

Biceps Tendon Disease
Speed’s test• Bicipital tendonitis• Elbow extended as patient
forward flexes shoulder against resistance
• (+) = reproduction of pain

AC Joint Degeneration
Cross-body adduction test• AC joint degeneration• Passively adducting arm across
chest while palpating AC joint
• (+) = pain in area of AC joint

Thank You
Top Related