






Languages
Pages
Legal


Persistent Critical Illness
Theodore J. Iwashyna, MD, PhDUniversity of Michigan
Ann Arbor VA Center for Clinical Management Researchwhile on sabbatical at ANZIC-RC at Monash University
1 November 2016 -- CCCF

This is joint work with:
• Carol Hodgson
• David Pilcher
• Michael Bailey
• Allison van Lint
• Shaila Chavan
• Neil Orford
• John Santamaria
• Rinaldo Bellomo
• Liz Viglianti
• Kyle Kepreos
• Brenda Vincent
• Wyndy Wiitala
• Joanne McPeake
• Tara Quasim
• Martin Shaw

It is our hypothesis that
there exists a substantial and growing group of patients
who are ICU-dependent, in the sense that they are are unable to
live for more than a few days outside of intensive-care-like services
whose current problems are driven by their ongoing cascading
critical illnesses rather than their original ICU admitting diagnosis
who account for a substantial portion of our bed-days
for whom we have little specific expertise in promoting their
recovery (as opposed to continuing their resuscitation)
but who are not immutably fated to such limbo, but rather whose
care we could improve both via improved ICU patient selection but
also by changing care & communication practices in the ICU
Iwashyna, Hodgson, Pilcher, Orford, Santamaria, Bailey, Bellomo (2015) Crit Care & Resusc 17:215.

Persistent Critical Illness:
“those patients whose reason for
being in the ICU is now more related
to their ongoing critical illness than
their original reason for admission to
the ICU”
A novel concept in the family of
“Chronic Critical Illness”
• Persistent critical illness (as defined
here)
• Chronic Critical Illness / Medically
Complex patients
• Diseases with long intrinsic
recovery times
• Prolonged weaning
• Prolonged ICU length of stay
Iwashyna, Hodgson, Pilcher, Orford, Santamaria, Bailey, Bellomo (2015) Crit Care & Resusc 17:215.

Iwashyna, Hodgson, Pilcher, Bailey, Bellomo (2015) Critical Care & Resuscitation 17:153.
Role N=101
Relative
Distribution
ICU Consultant 59 70 %
Research Coordinator 10 12 %
Nurse 14 17 %
Project Manager 1 1 %
Dietitian 11 13 %
Physiotherapist 4 5 %
Other 2 2 %
Persistent Critical Illness, as Characterized by Australian and New
Zealand ICU Clinicians
Aim: determine, via websurvey, the perspectives of members of the
ANZICS CTG regarding patients with persistent critical illness.
Time to Onset of Persistent Critical Illness: 10 days (IQR: 7-14)
Incidence Estimate: 10% (IQR: 5%-15%) of all ICU Patients
Fraction of Prolonged ICU Length of Stay that is Due to
Persistent Critical Illness: 50% (IQR: 20% - 60%)

Iwashyna, Hodgson, Pilcher, Bailey, Bellomo (2015) Critical Care & Resuscitation 17:153.
Typical Problems of the
Persistently Critically Ill0% 25% 50% 75% 100%
Respiratory Insufficiency
Delirium
Acquired Neuromuscular…
Sepsis
Kidney Injury
Malnutrition
Skin Breakdown and…
Traumatic Brain Injury
Severe Wounds
Pancreatitis
Heart Failure
Liver Failure
Gastrointestinal Bleeding
Severe Burns
Stroke
Endocrinopathies
Percent of Respondents (n=78)
90% identified ongoing
mechanical ventilation
as the typical need

Iwashyna, Hodgson, Pilcher, Bailey, Bellomo (2015) Critical Care & Resuscitation 17:153.
Not Persistently Critically Ill:
Diseases with Long Intrinsic
Recovery Times0% 25% 50% 75% 100%
Neuromuscular Disease
Head Trauma
Pancreatitis
Intracranial Haemorrhage
Neurologic Infection
Hepatic Failure
Multiple Trauma Excluding…
Isolated Cervical Spine…
Cardiogenic Shock
Pneumonia
Cardiac Arrest
Intestinal Surgery
Ischemic Stroke
Seizure
Percent of Respondents (n=78)

Iwashyna, Hodgson, Bailey, Pilcher, van Lint, Chavan, Bellomo (2016) Lancet Resp Med 4:566.
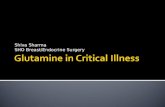
Timing of Onset and Burden of Persistent Critical Illness
Aim 1: Test the “persistent critical illness” hypothesis that there
is a point in the ICU stay beyond which ICU-admission
diagnosis and severity of illness in the first 24 hours no longer
differentiates patients regarding their probability of in-hospital
death.
Aim 2: Measure the timing of such a population-level transition.
Aim 3: Characterize the utilization of such persistently critically
ill patients.

Iwashyna, Hodgson, Bailey, Pilcher, van Lint, Chavan, Bellomo (2016) Lancet Resp Med 4:566.
Characteristic All Patients
Median Age (IQR) – yr 65 (51–75)
Mean Age (SD) – yr 61∙5 (17∙7)
Male sex – no. (%) 602,455 (58∙6)
APACHE III Score on Admission 49∙1 (26∙6)
Median risk of death on admission
(ANZROD) (IQR) – %2∙2 (0∙5–6∙9)
Mean risk of death on admission
(ANZROD) (SD) – %10∙0 (18∙3%)
Median duration of ICU stay (IQR) – days 1∙7 (0∙9–3∙0)
Median duration of hospital stay (IQR) –
days8∙4 (4∙6–15∙6)
Major Diagnostic Category – no. (%)
Cardiovascular (CABG/Valve) 162,858 (15∙8)
Other cardiovascular 137,445 (13∙4)
Respiratory 155,376 (15∙1)
Gastrointestinal 180,351 (17∙5)
Neurological 110,270 (10∙7)
Trauma 46,304 (4∙5)
Sepsis 52,066 (5∙1)
Other 183,565 (17∙9)
Characteristic All Patients
Hospital Outcome – no. (%)
Death 102,948 (10∙0)
Discharge to
Home 782,520 (76∙1)
Rehabilitation or Long-term Care 77,418 (7∙5)
Other Hospital 65,349 (6∙3)

Iwashyna, Hodgson, Bailey, Pilcher, van Lint, Chavan, Bellomo (2016) Lancet Resp Med 4:566.

Iwashyna, Hodgson, Bailey, Pilcher, van Lint, Chavan, Bellomo (2016) Lancet Resp Med 4:566.
1
10
20
30
Od
ds R
atio
fo
r D
ea
th,
Co
mp
ari
ng
Pa
tie
nts
wh
o h
ad
Hig
h L
ike
liho
od
of
De
ath
on
Ad
mis
sio
n t
o t
ho
se
with
Lo
w L
ike
liho
od
0 10 20 30ICU Days Completed

Iwashyna, Hodgson, Bailey, Pilcher, van Lint, Chavan, Bellomo (2016) Lancet Resp Med 4:566.

Iwashyna, Hodgson, Bailey, Pilcher, van Lint, Chavan, Bellomo (2016) Lancet Resp Med 4:566.
Reason for ICU Admission
Number in Validation
Cohort
Day on which Acute
Characteristics are No
Longer More Predictive
than Antecedent
Characteristics Alone
Day on which Acute
Characteristics are No
Longer Statistically
Significantly More
Predictive than Antecedent
Characteristics Alone
Cardiac Surgical 75,340 22 6
Cardiovascular 64,716 11 9
Respiratory 74,213 9 7
Gastrointestinal 86,722 12 8
Neurologic 51,453 9 7
Trauma 22,108 17 9
Sepsis 24,977 7 6

Iwashyna, Hodgson, Bailey, Pilcher, van Lint, Chavan, Bellomo (2016) Lancet Resp Med 4:566.
Hospital Outcome 10 or Fewer Days More Than 10 Days
Death 90,323 (9∙2) 12,625 (24∙4)
Discharge
to home 758,552 (77∙7) 23,698 (49∙9)
to Rehabilitation or
Long-term Care
68,584 (7∙0) 8,834 (17∙2)
to Other Hospital 59,627 (6∙1) 6,082 (11∙8)
The 51,509 patients who stayed 10 days or more accounted for:
5.0% of all ICU patients in Australia and New Zealand;
32.8% of all ICU bed-days (1,029,354 ICU bed days); and
14.6% of all hospital-bed-days by ICU patients (2,197,108 hospital bed days).

Interim Conclusions
• Persistent critical illness can be defined and is probably not just relabelling
currently described syndromes of chronic critical illness.
• Many ANZ clinicians identify consistent features of persistent critical illness
and have concerns about these patients.
• The “persistent critical illness” hypothesis that there is a point in the ICU
stay beyond which ICU-admission diagnosis and severity of illness in the
first 24 hours no longer differentiates patients regarding their probability of
in-hospital death is supported, with onset somewhere during the second
week.




Interim Conclusions
• The “persistent critical illness” hypothesis that there is a point in the ICU
stay beyond which ICU-admission diagnosis and severity of illness in the
first 24 hours no longer differentiates patients regarding their probability of
in-hospital death is supported, with onset somewhere during the second
week in both ANZ and VA2014.
• Next steps include:
• Patterns post-discharge mortality and healthcare utilization
• Detailed examination of the evolution of ICU patients in this time frame
• Understanding the relative importance of non-resolution; cascading new
problems; complications of care; and iatrogenesis in mechanisms

Please email me at [email protected] or tweet me @iwashyna for copies of
slides or to continue the conversation

ExploratoryEmpirical Work
Articulate theConcept
ConsensusConference
Workable Case Definition& Admin Operationalization
Validation
MeasureBurden
Prognostication &Risk Stratification
Interventions
Critical Care & Resuscitation “Point of View” published
Presentations to Assorted Bodies done
Survey of ANZ Clinicians published
Timing of Onset and Burden under review
Criterion Validation 1: Do case def pts meet clinician judgement gold standar d?
Predictive Validation 2: Do case def pts have higher subsequent mortality , readmits?
Replications of Timing Analysis: VA and ICNARC
Goal: Define a clear, clinically relevant case definition
First round convened, consensus 2/3 drafted
Second round February - March 2016
Cascades of Primary Problems possible VA MERIT
ANZ Time Course of Complications & Hospital-Acquir ed Conditions data being obtained
Survey respondents offered 188
recommendations for possible
interventions to improve care.

ExploratoryEmpirical Work
Articulate theConcept
ConsensusConference
Workable Case Definition& Admin Operationalization
Validation
MeasureBurden
Prognostication &Risk Stratification
Interventions
Critical Care & Resuscitation “Point of View” published
Presentations to Assorted Bodies done
Survey of ANZ Clinicians published
Timing of Onset and Burden under review
Criterion Validation 1: Do case def pts meet clinician judgement gold standar d?
Predictive Validation 2: Do case def pts have higher subsequent mortality , readmits?
Replications of Timing Analysis: VA and ICNARC
Goal: Define a clear, clinically relevant case definition
First round convened, consensus 2/3 drafted
Second round February - March 2016
Cascades of Primary Problems possible VA MERIT
ANZ Time Course of Complications & Hospital-Acquir ed Conditions data being obtained
Survey respondents offered 188
recommendations for possible
interventions to improve care.

Iwashyna, Hodgson, Bailey, Pilcher, van Lint, Chavan, Bellomo (2015) under review
Thank you for your attention.
Email me at [email protected] or
tweet me @iwashyna for copies of slides
or to continue the conversation.

Van den Berge (1998) Verhandelingen - Koninklijke Academie voor Geneeskunde van Belgie 60:487.

http://innovation.cms.gov/Files/reports/ChronicallyCriticallyIllPopulation-Report.pdf;Kahn et al (2010) JAMA 303:2253.; Kahn et al (2015) Crit Care Med 43:282.

Iwashyna, Hodgson, Pilcher, Bailey, Bellomo (2015) Critical Care & Resuscitation forthcoming.
0 10 20 30 40
Die before leaving the hospital?
Die in the 6 months afterdischarge from hospital?
Survive 6 months after dischargewith high level support in a…
Survive 6 months after dischargewith significant assistance at…
Be alive and well at 6 monthsafter discharge?
0 10 20 30 40
Die before leaving the hospital?
Die in the 6 months afterdischarge from hospital?
Survive 6 months after dischargewith high level support in a…
Survive 6 months after dischargewith significant assistance at…
Be alive and well at 6 monthsafter discharge?
Persistently Critically Ill:
Prolonged ICU Length of Stay

Iwashyna, Hodgson, Pilcher, Bailey, Bellomo (2015) Critical Care & Resuscitation forthcoming.
0
5
10
15
Fre
qu
ency
Quality of Care for Persistently Critically Ill
Poor Care Excellent CareExcellent Care
0
5
10
15
Fre
que
ncy
Care is Stressful for Team
Very Stressful Not Stressful
0
5
10
15
20
Fre
qu
en
cy
Care is Cost Effective
Not At All VeryVery Cost Effective
Top Related