






Languages
Pages
Legal


10/10/2015
1
What Can We Treat and
What Should We Treat
Christian Spies, MD Interventional Cardiology
The Queen’s Medical Center
Associate Professor of Medicine
University of Hawaii
Percutaneous Mitral Valve Repair:
Innovative Procedures, Devices & State of
the Art Care for Arrhythmias, Heart Failure &
Structural Heart Disease October 8-10, 2015
Hilton Hawaiian Village, Honolulu, HI
Can treat (FDA approved): • Moderate to severe, degenerative mitral regurgitation in patients
who are deemed too high risk for surgery (STS score >6/8%)
Should treat (Not FDA approved): • Isolated moderate to severe, functional mitral regurgitation
irrespectively of the operability of the patient
What Can We Treat and
What Should We Treat

10/10/2015
2
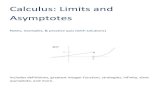
3 Nkomo et al. Lancet, 2006; 368: 1005-11.
> 9.3% for ≥75 year olds (p<.0001)
14
12
10
8
6
4
2
0
Pre
vale
nce (
%)
of m
odera
te
to s
evere
valv
e d
isease
Aortic valve disease
Age (years)
<45 45-54 55-64 65-74 >75
Mitral valve disease
All valve disease
Mitral Regurgitation Needs Assessment
Total MR Patients1,2
Eligible for Treatment3,4
(MR Grade ≥3+)
4,100,000
1,700,000
Annual MV Surgery5
Annual Incidence3
(MR Grade ≥3+) 250,000
30,000 Only 2% Treated Surgically
14% Newly Diagnosed
Each Year
1,670,000
Untreated Large
and Growing Clinical
Unmet Need
1. US Census Bureau. Statistical Abstract of the US: 2006, Table 12.
2. Nkomo et al. Burden of Valvular Heart Diseases: A Population-based Study, Lancet, 2006; 368: 1005-11.
3. Patel et al. Mitral Regurgitation in Patients with Advanced Systolic Heart Failure, J of Cardiac Failure, 2004.
4. ACC/AHA 2008 Guidelines for the Management of Patients with Valvular Heart Disease, Circulation: 2008
5. Gammie, J et al, Trends in Mitral Valve Surgery in the United States: Results from the STS Adult Cardiac Database, Annals of Thorac ic Surgery 2010.
Mitral Regurgitation 2009 U.S. Prevalence
Mitral Regurgitation Needs Assessment

10/10/2015
3
Annulus
Leaflets
Cordae
Papillary
Muscles
Adjacent
Myocardium
Mitral Regurgitation Anatomy
Primary: Anatomic abnormality
the mitral valve
• Leaflets
• Subvalvular
apparatus
• Chordae and
papillary muscles
Secondary : LV dilation; often
secondary to ischemic
heart disease
• Leads to mitral
annular dilation
• Incomplete coaptation
of the mitral valve
Mitral Regurgitation Classification
Primary = Degenerative MR
Secondary = Functional MR

10/10/2015
4
Primary
“The Valve”
Secondary
“The Ventricle”
Usually myxomatous Ischemic or not
Mitral Regurgitation Classification
8
Natural History
Avierinos JF, et al. Circulation 2002;106:1355
100
90
80
70
60
50
Surv
ival %
0 2 4 6 8 10
2 RF
1 RF
95 ±2
70 ±5
55 ±9
Risk Factors
Age 50 yrs
Atrial fibrillation
LA enlargement
Flail
Mild MR
MR 3
or
EF <50%
Years after diagnosis
Asymptomatic Degenerative MR

10/10/2015
5
9
Severity and Survival
Enriquez-Sarano M et al. NEJM 2005;352:875-83
Worse Survival
100
90
80
70
60
50
0
Surv
ival
(%)
Years
0 1 2 3 4 5
P<0.01
ERO <20mm2 (91 ±3%)
ERO 40mm2 (58 ±9%)
ERO 20-39mm2
(66 ±6%)
More CV Events
70
60
50
40
30
20
10
0 R
ate
of C
ard
iac E
vents
%
Years
0 1 2 3 4 5
P<0.01
ERO <20mm2 (15 ±4%)
ERO 20-39mm2
(40 ±7%)
ERO 40mm2 (62 ±8%)
Asymptomatic Degenerative MR
100
80
60
40
20
0
Surv
ival %
Years
0 1 2 3 4 5 6 7 8 9 10
EF 60%
EF 50-60%
EF <50%
P=0.0001
72 ±4%
53 ±9%
EF <60% is Abnormal in MR
32 ±12%
Enriquez-Sarano M, et al., Circulation 1994;90:830-837
EF and Surgical Outcome

10/10/2015
6
11
100
80
60
40
20
0
Surv
ival %
Years
0 1 2 3 4 5 6 7 8 9 10
NYHA I-II
NYHA III-IV
P<0.0001
90 ±2
76 ±5
73 ±3
48 ±4
Tribouilly CM et al., Circulation 1999;99:400-5
Symptoms and Surgery
12
Patients without Class I Indications
100
80
60
40
20
0
Surv
ival %
Follow-up, y
0 5 10 15 20
Suri R et al., JAMA 2013;310:609-16
Early surgery
Medical management
Log-rank P<.001
Degenerative MR- Early Surgery is Better

10/10/2015
7
Wu AH, et al. J Am Coll Cardiol 2005;45:381-87
1.0
0.8
0.6
0.4
0.2
0.0
Event-
free S
urv
ival
Time (Days)
0 500 1000 1500 2000
Functional MR- No Mortality Benefit with Surgery
Glower. JACC 2012;60:1315-22
Functional MR- High Risk of Recurrence
0 1 2 3 4 5 6 7 8 9 10 12 14 16 18 20
Years
100
80
60
40
20
0 Fre
edom
Fro
m
Mitra
l R
egurg
itation
DMR >3+
DMR >2+
IMR > 2+

10/10/2015
8
Degenerative MR
Surgery for symptoms or
LV dysfunction
Functional MR
Asymptomatic
if repairable
and low risk
Medical
therapy first
No medical
option for valve
Consider CRT
Surgery only in highly
selected patients with HF
Surgery is Class I
Indication
Surgery is Class II b
Indication
Nishimura et al. JACC 2014;63:e57
Current General Principals
of Therapy
16 Mirabel M, et al. Eur Heart J 2007;28:1358-1365
No surgery in 49%
Predictors were
age, morbidity, non-
ischemic etiology,
MR severity
396 patients with symptomatic severe MR
53% degenerative
0
20
40
60
80
100
120
140
160Decision notto operate
Decision to
operate
P<0.0001
63% 59% 67% 42%
15%
<50 50-60 60-70 70-80 >80
Unoperated MR in Europe

10/10/2015
9
Percutaneous Mitral Valve Repair MitraClip® System
EVEREST II Trial
279 Patients enrolled at 37 sites
Randomized 2:1
Significant MR (3+-4+) Specific Anatomical Criteria
Device Group MitraClip System
N=184
Control Group Surgical Repair/Replacement
N=95
Feldman et al. Engl J Med 2011;364:1395-406.
Echocardiography Core Lab and Clinical Follow-Up:
Baseline, 30 days, 6 months, 1 year, 18 months, and
annually through 5 years

10/10/2015
10
EVEREST II Trial
Inclusion – Candidate for MV Surgery
– Moderate to severe (3+) or severe (4+) MR
• Symptomatic – >25% EF & LVESD
≤55mm
• Asymptomatic with one or more of the following
– LVEF 25-60%
– LVESD ≥40mm
– New onset atrial fibrillation
– Pulmonary hypertension
Exclusion – AMI within 12 weeks
– Need for other cardiac surgery
– Renal insufficiency • Creatinine >2.5mg/dl
– Endocarditis
– Rheumatic heart disease
– MV anatomical exclusions • Mitral valve area <4.0cm2
• Leaflet flail width (≥15mm) and gap (≥10mm)
• Leaflet tethering/coaptation depth (>11mm) and length (<2mm)
Feldman et al. Engl J Med 2011;364:1395-406.
All Etiologies included !
LCB = lower confidence bound
UCB = upper confidence bound
Safety Major Adverse Events
30 days
0 20 40 60
Device Group, n=180
Control Group, n=94
Met superiority hypothesis • Pre-specified margin =2%
• Observed difference = 32.9%
• 97.5% LCB = 20.7%
15.0%
47.9%
pSUP <0.0001
0 10 20 30 40 50 60 70 80 90 100
Effectiveness Clinical Success Rate
12 months
Control Group, n=89
Device Group, n=175
Met non-inferiority hypothesis • Pre-specified margin = 25%
• Observed difference = 7.3%
• 95% UCB = 17.8%
55%
73%
pNI =0.007
Feldman et al. Engl J Med 2011;364:1395-406.
EVEREST II Trial –
Primary Endpoints (ITT)

10/10/2015
11
Feldman et al. Engl J Med 2011;364:1395-406.
EVEREST II Trial –
Conclusions
FDA approval of MitraClip for all patients with mitral
regurgitation (degenerative and functional)?
Age: 82 ±9 years
Prior MI: 24%
Prior stroke: 10%
Diabetes: 30%
COPD: 32%
Renal disease: 28%
Mean STS Risk
13.2%
Lim et al. JACC 2014;64:182-192.
Prohibitive Surgical Risk
DMR Cohort (n=127)

10/10/2015
12
Primary Safety Endpoint Primary Safety Endpoint 30-day Observed Mortality Lower than Predicted
18.2% 4.8%0%
5%
10%
15%
20%
MeanMortality
Rate
N = 351
Observed Predicted
Mortality
HR Cohort (N=351):
Observed Mortality 95% UCB
4.8% 7.6%
Mean Predicted Mortality 95% LCB 95% UCB
Mean Predicted Mortality 95% LCB 95% UCB18.2% 17.3%
19.1%
p < 0.0001
As presented by Scott Lim MD, ACC 2013
ACC 2013, presented by Scott Lim, MD
Left Ventricular Volumes
Hospitalizations for Heart Failure
Left Ventricular End Diastolic Volume Left Ventricular End Systolic Volume
(N = 69) Paired
Data (N=69)
0.67
0.18
0.0
0.2
0.4
0.6
0.8
1.0
1 Year Prior… 1 Year Post…
HF
Ho
spit
aliz
atio
n R
ate
pe
r P
atie
nt Y
ear
73% Reduction
125
109
60
70
80
90
100
110
120
130
140
Baseline 1 Year
Vo
lum
em
L
-16 mL
0
49
46
30
35
40
45
50
55
60
Baseline 1 Year
0
-3 mL
4+
4+
3+
3+
2+
2+
1+
1+
0%
20%
40%
60%
80%
100%
Baseline 12 Months
Patie
nts
(%
)
Mitral Regurgitation Grade
0
1+
3+
4+
2+ Clinically Important Reduction
of Mitral Regurgitation
IV
IV IV
III
III III
II
II II
I
I I
0%
20%
40%
60%
80%
100%
Baseline 30 Days 12 Months
Patie
nts
(%
)
NYHA Functional Class
I
II
IV
III Clinically Important Improvement
in NYHA Functional Class
Clinically Important Reduction
in the Rate of Hospitalization
for Heart Failure
Clinically Important Reverse
LV Remodeling
Prohibitive Surgical Risk
DMR Cohort (n=127)

10/10/2015
13
Summary
• MitraClip® therapy safely reduces DMR in patients at
prohibitive risk for MV surgery
• In this group of prohibitive risk DMR patients, MitraClip
therapy provides meaningful clinical improvements
• Reduction of LV volumes
• Improvements in NYHA Functional Class
• Improvements in Quality of Life
• Reduction in Hospitalizations for Heart Failure
FDA Approval
MitraClip Delivery System Approved by FDA on October 24, 2013.
Indication for Use:
“The MitraClip Clip Delivery System is indicated for the
percutaneous reduction of significant symptomatic mitral
regurgitation (MR ≥ 3+) due to primary abnormality of the mitral
apparatus [degenerative MR] in patients who have been
determined to be at prohibitive risk for mitral valve surgery by a
heart team, which includes a cardiac surgeon experienced in
mitral valve surgery and a cardiologist experienced in mitral valve
diseased, and in whom existing comorbities would not preclude
the expected benefit from reduction of the mitral regurgitation.
Definition of Prohibitive Risk: STS score of surgical MV repair
>6% or mitral valve replacement >8%

10/10/2015
14
Medical Therapy
Less Invasive
Increased MR Reduction
MV Surgery
MitraClip®
Options for Degenerative MR
STS score > 6/8%
• Limited treatment options
(medications, CRT)
• Surgery with no mortality
benefit
• High recurrence rate after
surgical MV repair
• Class IIb indication in recent
guidelines to consider
surgery
Functional Mitral Regurgitation

10/10/2015
15
• Treating Centers: 491
• Patients: 20,018
• Implant Rate: 96%
• Etiology
• Functional MR 65%
• Degenerative MR 22%
• Mixed 13%
Data as of 03/31/2015. Source: Abbott Vascular.
FMR 65%
DMR 22%
Mixed 13%
Etiology
Realism: 70% FMR
Access-EU: 69% FMR
TRAMI: 71% FMR
Worldwide Mitraclip Experience
Functional Mitral Regurgitation
Beigel et al. JACC 2014;64:2688-2700

10/10/2015
16
Transcatheter Valve Treatment
Sentinel Pilot Registry (TCVT)
• TCVT: Transcatheter Valve Treatment Sentinel Pilot Registry
• Part of European Society of Cardiology
• Prospective, independent registry of consecutive patients
• 628 Patients at 25 centers in 8 countries
Nickenig G. Et al. J Am Coll Cardiol 2014;64:875–84
TCVT – Baseline Characteristics
Nickenig G. Et al. J Am Coll Cardiol 2014;64:875–84

10/10/2015
17
TCVT – Procedural Characteristics
TCVT – NYHA Class

10/10/2015
18
TCVT – Degree of MR
TCVT – Echo Characteristics

10/10/2015
19
Cardiovascular Outcomes Assessment of the MitraClip
Percutaneous Therapy for Heart Failure Patients with
Functional Mitral Regurgitation
Purpose
• COAPT is a landmark trial to further study the
MitraClip device in symptomatic FMR patients with
heart failure
• COAPT is the first randomized controlled clinical trial
to compare non-surgical (medical) standard of care
treatment to a percutaneous intervention to reduce
MR

10/10/2015
20
To evaluate the safety and effectiveness of
the MitraClip System for treatment of
functional mitral regurgitation (FMR ≥3+) in
symptomatic heart failure subjects who are
treated per standard of care and who have
been determined by the site’s local heart team
as not appropriate for mitral valve surgery
STS score is no inclusion or exclusion criterion!
Objective
41
Randomize 1:1
Clinical and TTE follow-up:
Baseline, Treatment, 1-week (phone)
1, 6, 12, 18, 24, 36, 48, 60 months
Control group
Standard of care
N=215
Symptomatic heart failure subjects who are treated per standard of care
Determined by the site’s local heart team as not appropriate for mitral valve surgery
Specific valve anatomic criteria
MitraClip
N=215
Significant FMR (≥3+ by core lab)
Goals: 430 patients at up to 79 US sites
Trial Design

10/10/2015
21
0
25
50
75
100
125
150
175
200
225
250
275
300
325
350
375
400
425
450
D-1
2
J-1
3
F-1
3
M-1
3
A-1
3
M-1
3
J-1
3
J-1
3
A-1
3
S-1
3
O-1
3
N-1
3
D-1
3
J-1
4
F-1
4
M-1
4
A-1
4
M-1
4
J-1
4
J-1
4
A-1
4
S-1
4
O-1
4
N-1
4
D-1
4
J-1
5
F-1
5
M-1
5
A-1
5
M-1
5
J-1
5
J-1
5
A-1
5
S-1
5
O-1
5
N-1
5
D-1
5
J-1
6
F-1
6
M-1
6
Nu
mb
er
of
Su
bje
cts
Months
Randomization Projection
Projected
Actual
Accelerated
Current Enrollment
Can treat (FDA approved): • Moderate to severe, degenerative mitral regurgitation in patients
who are deemed too high risk for surgery (STS score >6/8%)
Should treat (Not FDA approved): • Isolated moderate to severe, functional mitral regurgitation
irrespectively of the operability of the patient
Percutaneous Mitral Valve Repair: What Can We Treat and What Should We Treat
Top Related