







Languages
Pages
Legal

CME March 2015
David Moore
32 year old male
Approached a passer-by in Doubleview stating he had just been shot in the abdomen
Ambulance called by passer-by
On SJA arrival, patient hypotensive (85/50) and tachycardic at 120bpm
On examination of the abdomen, 3x wounds to anterior abdomen around the umbilicus ?Gunshot wounds
Patient brought to scghed
Stab wounds (SW) are more common than gunshot wounds (GSW)
SW have a lower mortality due to the lower energy transmitted.
In the USA, 90% of deaths related to penetrating abdominal injury (PAI) are caused by GSW.
Incidentally, blunt abdominal trauma has greater mortality than PAI (more difficult to diagnose, commonly associated with trauma to multiple organs/systems).
Prior to World War I, PAI was managed expectantly. During World War II, studies showed that early laparotomy improved survival.
By the late 1950’s, routine laparotomy was the standard treatment for PAI.
Over the last 30 years the pendulum has shifted towards selective management.
The introduction and refinement of diagnostic procedures and imaging studies, such as laparoscopy, CT scan, and focused abdominal sonography for trauma (FAST), has contributed significantly in the new trends of PAI management.
Laparotomy now thought unnecessary in 70% of abdominal stab wounds
Increased complication rates, length of stay, costs Immediate laparotomy indicated for:
1. Peritonism
2. Evisceration3. Haemodynamic instability4. Penetrating object is still in situ5. GI bleeding following PAI6. Free air (in stab wounds may represent the introduction of external air rather than GI perforation)
Any wound between the nipple line (T4) and the groin creases anteriorly, and from T4 to the curves of the iliac crests posteriorly
However, if the wound was caused by a projectile, then a PAI could result from an entry wound in almost any part of the body
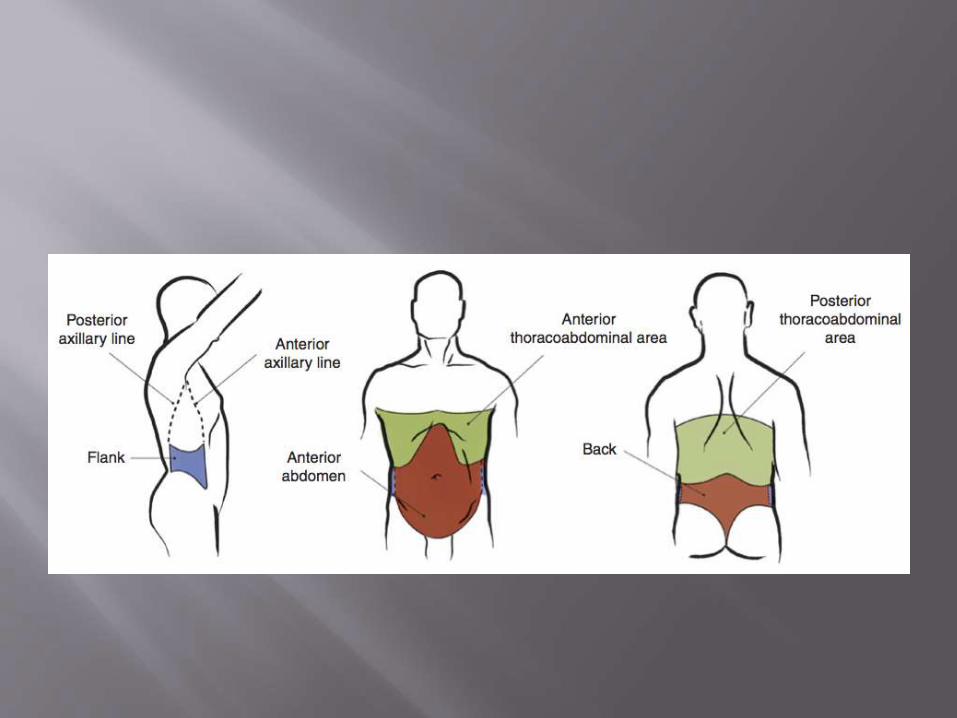
1. Anterior abdomen Between the anterior axillary lines; bound by the costal
margin superiorly and the groin crease distally
2. Thoracoabdominal area Area delimited by the costal margin
inferiorly and superiorly by the fourth intercostal space anteriorly, sixth intercostal space laterally and eighth intercostal space posteriorly. Note: injuries in this area increase likelihood of diaphragmatic, chest and mediastinal injuries.
3. Flanks Bound by anterior axillary line and posterior axillary line, inferior
costal margin superiorly to iliac crests
4. Back Between posterior axillary lines extending from costal margin to the iliac
crests
Stab wounds –
- Knives, ice picks, pens, coat hangers, broken bottles
- Liver, small bowel, spleen
Gunshot wounds
- small bowel, colon, liver
- often multiple organ injuries, bowel
perforations

Airway
Breathing
Circulation
Disability
Exposure
General Trauma principles:
Airway management, 2x large bore IVs, fluid
resuscitation, major haemorrhage protocol.
Cover penetrating wounds and eviscerations with sterile dressings.
Prophylactic Abx: Decrease risk of intraabdominal sepsis (eg Cephazolin 2g).
In general, leave foreign bodies in and remove in theatre.
Pulseless Arrive without pulses but with witnessed recent or current
signs of life (e.g. PEA)
Major vascular injury most likely
Need immediate laparotomy in theatre within 5 minutes of
arrival
Second option is thoracotomy in ED and cross-clamp aorta.
Both have very low functional survival yields.
Haemodynamically Unstable Require immediate laparotomy!
Includes non-responders and transient responders to initial
fluid bolus
Unnecessary investigations or interventions should be avoided.
CXR and FAST scan can help if unsure that abdomen is source
of bleeding.
There are multiple stab wounds/gunshot wounds to multiple cavities
The wounds are at, or cross, junctional zones (e.g. costal margin, groin, buttock wounds).
There is evidence or the possibility of cardiac tamponade
The diagnosis of massive haemothorax may be made clinically, with a FAST scan, chest tube or CXR
Selective management used to reduce the number of laparotomies
Investigations to determine if there is intraperitoneal injury requiring operative repair
Strategy depends on abdominal region
Note: Haemodynamically normal patients with clinical signs of peritonitis, or with evisceration of bowel should be taken immediately to theatre
The goal of any algorithm for PAI should be to identify injuries requiring surgical repair, and avoid unnecessary laparotomy with its associated morbidity.
There are several options for evaluating PAI in the haemodynamically normal trauma patient without signs of peritonitis.
Many of these patients will have some superficial tenderness around the wound site, but no signs of peritoneal injury/inflammation.
CXR - Peritoneal penetration is confirmed by free air under diaphragm, but absence of free air does not rule it out.
Ultrasound (FAST) – Looking for free fluid in the abdomen or evidence of abdominal fascia violation.However, there are false negatives for intra-abdominalinjury….FAST is not great at picking up small amounts of fluid which may be associated with a hollow viscus injury.So, a positive FAST indicates peritoneal penetration but a negative FAST does not exclude significant injury and so should be used in combination with otherinvestigations
Local wound explorationCan be performed in the ED as follows:
universal precautions
perform procedure under sterile conditions
Local anesthesia is injected at the wound site
The wound track is followed through the layers of the abdominal wall or until its termination.
The goal is to identify the end point of the tract, this usually requires extension of the wound to allow adequate visualisation.
A positive result is penetration of the posterior rectus fascia or the transversus fascia below the rectus line.
Note: Wounds overlying the rib cage should not be explored (may cause pneumothorax).
Diagnostic Peritoneal Lavage (DPL)
The role of DPL in the haemodynamically normal patient is to
identify hollow viscus injury (stomach, small bowel, colon) or diaphragmatic injury.
Disadvantages: It is invasive, does not evaluate the retroperitoneum, has a significant false positive rate.
A positive result is >100,000 RBCs for anterior abdominal wounds and 10,000 RBCs for thoracoabdominal wounds.
DPL is now used only if FAST and CT not available.
CT abdomen (with IV contrast) Optimal method for determining both peritoneal penetration and
intra-peritoneal injury unless emergency laparotomy is indicated
~97% sensitive for peritoneal violation
Of all the diagnostic modalities CT gives the best assessment of retroperitoneal structures.
Be aware that some diaphragmatic injuries will be missed on CT –although sensitivity is approaching 95% with new CT scanners –
Patients require close observation and consideration of other tests (e.g. the laparoscopy)
Serial physical Examination
Best sensitivity and negative predictive value of all modalities.
Patient is admitted under the General Surgeons for 24 hours. Hourly obs. Regular abdominal examination for signs of developing peritonitis
If patient develops any signs of haemodynamic instability or peritonitis then a laparotomy is performed
If the patient is well the following day they start a normal diet and are discharged once diet is tolerated.
Thoracoabdominal wounds - Big concern is
diaphragmatic injury – occurs in around 7% of thoracoabdominalwounds. Where there is evidence of thoracic and abdominal injury there must, by definition, be an injury to the diaphragm.
If concerned, Laparoscopy/thoracoscopy is recommended.
Flank or back wounds - Be highly suspicious for injury
to retroperitoneal organs e.g. Colon, kidney, lumbar vessels. Colon is the injury most often missed. Consider triple-contrast CT scan +/-Laparotomy.
32 yo male. Alleged gunshot to abdomen. 3x wounds to anterior abdomen - ?shotgun pellets. Hypotensive and tachycardic…
You get the call. How would you manage this patient??
Major trauma call
Major haemorrhage pack
Appropriate setting and staff
Preparation – bilateral chest drains if required
- Drugs (anaesthetics, analgesia,
inotropes)
- Airway equipment + difficult
airway trolley
On arrival, ABCDE
Wide bore cannulae bilaterally
Fluid resuscitation: Initially 2 units RBC and 1 unit FFP via rapid infuser
CXR – No haemothorax/pneumothorax
Fast scan +ve
IV Abx – Cephazolin 2g
Tranexamic acid 1g
Patient taken to theatre for Laparotomy-intraperitoneal bleed. 3x gunshot pellets removed from abdomen.
Top Related