






Languages
Pages
Legal

Pediatric Respiratory Distress

I. Pediatric Respiratory System
A. Developmental Aspects B. Respiratory parameters by age C. Recognition of Respiratory Distress D. Causes of Respiratory Distress in Pediatrics E. Investigation of Pediatric Respiratory Distress F. Treatment of Respiratory Distress
II. Case Management Examples
• Case 1: 20 month old male with fever, stridor• Case 2: 20 month old female with fever, stridor• Case 3: 5 year old male with URI and sudden
shortness of breath/ fever • Case 4: 5 year old female with URI and
shortness of breath/no fever• Case 5: 5 week old with ER presentation of
shortness of breath
Pediatric Respiratory System
• The younger the child the smaller the trachea is relative to body size
• “Stenting” cartilage rings in trachea stiffen over the first 12 months
• The lung will grow 15 fold from birth to adulthood• The “bony bellows” of the ribs are pliable (cartilage) at
young ages• The abdominal muscles are the “accessory” muscles of
respiration in toddlers• Infants are obligate nose breathers• Pediatric cardiac arrests are almost always precipitated
by respiratory arrest

Respiratory Parameters
• Newborn respiratory rate is 40 breaths per minute (+/-)
• Adolescent respiratory rate is 12-15 breaths per minute
• Tidal volume x respiratory rate= minute ventilation
• Minute ventilation requirements vary by energy needs
• Various disorders will affect tidal volume
Recognition of Respiratory Distress
• Inspection (i.E. Color, work of breathing)
• CNS status
• Vital signs
• Anticipation of deterioration

Causes of Pediatric Respiratory Distress
• Airway obstruction (large vs. Small airway)
• Alveolar disease• CNS disorder• Cardiovascular collapse • Metabolic changes (acidosis, fever)• Muscle drive disorder (abdominal
distension)

Investigation of Pediatric Respiratory Distress
• History
• Examination (including vital signs)
• Oximetry
• Pulmonary function testing
• Imaging
• Blood gases
Treatment of Respiratory Distress
• First reach for Oxygen
• treat the underlying cause
• support work of breathing with technology required/available
Case 1
• A 20 month old male is brought to the emergency room with fever to 104 degrees onset today. He has not had URI symptoms, but is having difficult breathing (retractions, nasal flaring) with a “muffled, thickened” quality to his respirations. He appears very anxious and is drooling. It is influenza season and you query the parents about whether he had influenza vaccination- their response is that they do not believe in vaccination. What approach is called for?
Epigottitis
• Etiology: Hemophilus influenza type B• DX by inspection of epiglottis in controlled situation
(Operating Room)• (Lateral neck soft tissue Xrays often challenging to
interpret)• Cultures of blood and epiglottis• Treatment by intubation, airway management,
antimicrobials• Prevention: Hemophilus vaccination has virtually
eliminated epiglottitis• Outcome: generally fatal if no intervention, otherwise
almost certain recovery
Case 2
• A 20 month old female comes to the Emergency Room with URI symptoms and fever to 104 degrees. She has had a hoarse voice and a”seal bark” quality to her cough. The parents noted that she seemed much better while they were driving in to the ER- but it worsened again here. She has intercostal retractions, though, does not appear anxious. Her older brother (age 8) had had a URI and sore throat a few days ago.
Croup• Etiology: usually parainfluenza virus• Mechanism: edema of glottic/ subglottic trachea• (Parainfluenza may also cause interstitial
pneumonitis)• DX: clinical picture• CXR may show “steeple sign” of subglottic region• Treatment: expectant management,
Dexamethasone may help more significant subglottic edema
• Course usually 5-7 days
Case 3
• This 5 year old male is brought to the office with onset of fever and shortness of breath today. He had been experiencing a “typical” URI for the last 4 days. His temp is 102.5 degrees and he has pale color with mild intercostal retractions. Oximeter is reading 88% on room air and respiratory rate is 38 breaths per minute.
Bacterial Pneumonia
• Many infectious agents may cause “pneumonia”- viral, bacteria, fungal
• Pediatric bacteria: pneumococcus, mycoplasma
• Pneumococcus: sequela post URI, lobar infiltrate
• DX= exam confirmed by CXR• Treatment: appropriate antimicrobial choice
(PCN resistance?)• Prevention: vaccination

Case 4• Late in the afternoon you are seeing a 5 year old
female with the chief complaint of shortness of breath. She has had URI symptoms for 3 days. Last night slept poorly and parents noted lack of energy and her complaints of “hard to breathe”. Parents note that she has had this pattern a few times in the past, but it was mild and never lasted more than 2 days. She has no fever but does show some accessory muscle use and intercostals retractions. Pale in color, her respiratory rate is 50 breaths per minute and oximeter is 88% on room air.
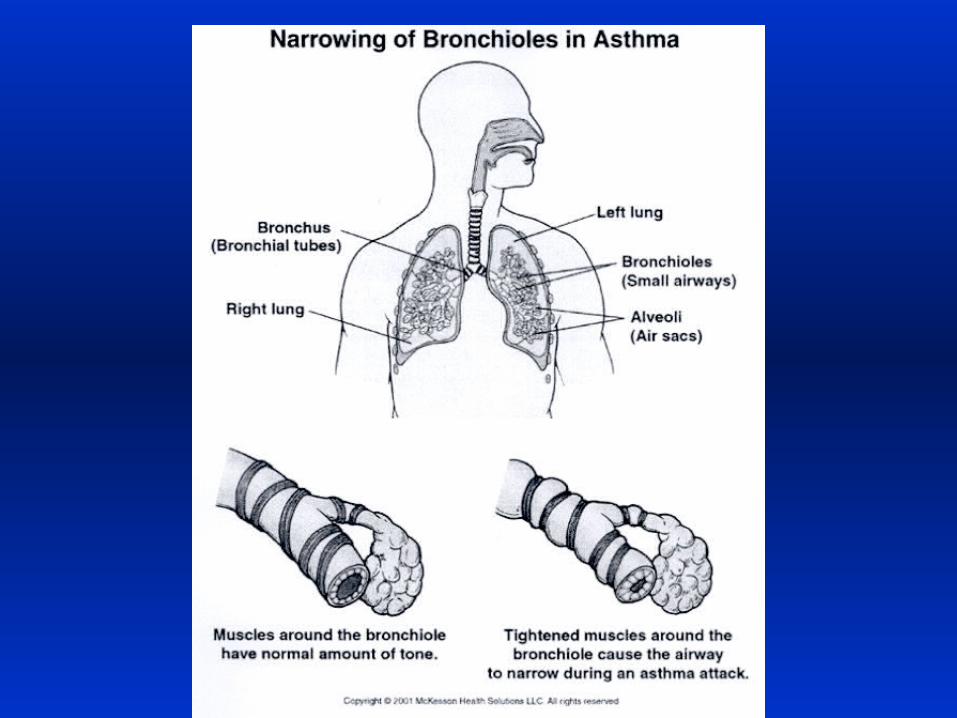
Asthma:
• Mechanism: spasm and/or edema of bronchioles
• Etiology is inflammatory trigger: infection, allergy, exertion
• Treatment: Beta 2 agonists, leukotriene inhibitors, corticosteroids
• Prevention: education, pharmacologic agents, environmental control
• Prognosis: resolution common under age 7 years, lifetime if older
Case 5
• Later that night during your ER clerkship you are tagging with one of the ER doctors when one of the nurses grabs her by the arm and urgently guides her to an exam room. It holds a 5 week old male with poor color and extreme work of breathing- abdominal heaving, retractions and a respiratory rate of 80 breaths per minute. Heart rate is 187 beats per minute. Oximeter is 68%. Parents note that he was fine until this morning but seemed to have more difficulty eating until 30 minutes ago when he became limp and poorly responsive.
Respiratory Syncytial Virus (RSV)
• RNA virus• Marked coryza symptoms in older children• Children under age 2 often have asthma-like
picture• Mechanism: bronchiolar edema/ severe
mucosal damage• Treatment: supportive care• Prevention by passive immunization
(monoclonal antibody)

• You are the first year FP resident doing your ER rotation and trying to get a quick supper in when your pager goes off. The ER charge nurse insists that you come immediately to assess a 2 y-o male in respiratory distress.
• When you get to the exam room he is laying in his father’s arms, pasty in color with profound retractions, and poorly aware. HR=180, RR= 30, Oximeter = 82%.
• Parents note that he was fine until this evening. They had been at a high school basketball game and he had been playing under the bleachers when he suddenly started to cough- progressing to respiratory distress.

Foreign Body Aspiration
• Generally under the age of two (up to four?)• Mechanism: f.b. migrating to airway causing ball
valve obstructive effect• History= often sudden change in respiratory status• Exam= respiratory distress, asymmetric breath
sounds• CXR= unilateral lung hyperexpansion (often right
side) with possible mediastinal shift away from involved side
• Treatment= removal of f.b. by bronchoscopy• Complications= pneumothorax, pneumonia
Pediatric Respiratory Distress Last Thoughts
• The respiratory system is the most vulnerable in Pediatrics
• Deterioration may progress rapidly• Simple airway management techniques may
buy time• Equipment required may have to be sized for
age• Accurate, rapid assessment and graded
supportive care take precedence over lavishing time on diagnosis
Top Related