







Languages
Pages
Legal


Patient Centered Medical Patient Centered Medical Home- what it can do for Home- what it can do for you and your patients! you and your patients!
Jennifer K. Phillips MDJennifer K. Phillips MD
Associate Professor UNM FCMAssociate Professor UNM FCM
NMAFP RuidosoNMAFP Ruidoso
7/18/20157/18/2015

What we want to What we want to accomplish todayaccomplish today
HistoryHistoryKey conceptsKey conceptsDataDataChange ManagementChange ManagementOur Vision Our Vision Team formation Team formation Ease of practice Ease of practice Pre-visit Information Pre-visit Information Planning VisitsPlanning VisitsManaging registriesManaging registriesFinal ThoughtsFinal Thoughts

Origins of the Medical Home Origins of the Medical Home
19671967• American Academy of PediatricsAmerican Academy of Pediatrics• Enhance the care of children with special needsEnhance the care of children with special needs
Community Oriented Primary CareCommunity Oriented Primary Care• Plan ahead for the needs of the population servedPlan ahead for the needs of the population served• Partner with the community and familyPartner with the community and family
Chronic Care Model Chronic Care Model • Enable patientsEnable patients• Proactive rather than reactive careProactive rather than reactive care
33Tollman, Soc Sci Med, 1991; Longlett, J Am Bd Fam Pract, 2001; Wagner
Joint Principles PCMH Joint Principles PCMH
• Personal physician relationship based carePersonal physician relationship based care• Physician directed medical practicePhysician directed medical practice• Whole person orientation Whole person orientation • Care is coordinated and integratedCare is coordinated and integrated• Quality and safetyQuality and safety• Enhanced accessEnhanced access• PaymentPayment
AAFP, AAP, ACP, AOA: March 2007AAFP, AAP, ACP, AOA: March 2007
Key conceptsKey concepts
PCMH was developed by primary care providers to PCMH was developed by primary care providers to encourage comprehensive health care, improve patient encourage comprehensive health care, improve patient outcomes, and lower medical costs.outcomes, and lower medical costs.
Patients in states with a greater number of primary care Patients in states with a greater number of primary care providers have better health outcomes.providers have better health outcomes.
The PCMH model emphasizes functional multidisciplinary The PCMH model emphasizes functional multidisciplinary teams that partner with patients as advisors.teams that partner with patients as advisors.
Community connections and health care navigators can Community connections and health care navigators can play an important role in the multidisciplinary team.play an important role in the multidisciplinary team.
Evidence-based medicine guides clinical decision Evidence-based medicine guides clinical decision making.making.
Outcomes are measured and quality and safety are our Outcomes are measured and quality and safety are our goals.goals.
Defining PCMHDefining PCMH
Primary carePrimary care Individualized, personal careIndividualized, personal care Patient centeredPatient centered Accessible: expanded hours, same day Accessible: expanded hours, same day
appointmentsappointments Full scope (entire patient population, mental Full scope (entire patient population, mental
health, laboratory, radiology, substance health, laboratory, radiology, substance abuse, nutrition, financial assistance) NO abuse, nutrition, financial assistance) NO SILOSSILOS
Culturally/linguistically appropriateCulturally/linguistically appropriate
NCQA requirements for NCQA requirements for PCMHPCMH
Written standards for patient access and patient communicationWritten standards for patient access and patient communication Use of data to show standards for patient access and communication Use of data to show standards for patient access and communication
are metare met Use of paper or electronic charting tools to organize clinical informationUse of paper or electronic charting tools to organize clinical information Use of data to identify important diagnoses and conditions in practiceUse of data to identify important diagnoses and conditions in practice Adoption and implementation of evidence-based guidelines for three Adoption and implementation of evidence-based guidelines for three
chronic conditionschronic conditions Active patient self-management supportActive patient self-management support Systematic tracking of test results and identification of abnormal resultsSystematic tracking of test results and identification of abnormal results Referral tracking, using a paper or electronic systemReferral tracking, using a paper or electronic system Clinical and or service performance measurement, by physician or Clinical and or service performance measurement, by physician or
across the practice across the practice Performance reporting, by physician or across the practicePerformance reporting, by physician or across the practice

Practice Organization:Practice Organization: Establish team, define goals, follow and Establish team, define goals, follow and
monitor progressmonitor progress Staffing-team based care, define roles Staffing-team based care, define roles
and responsibilitiesand responsibilities Train staff on team based careTrain staff on team based care Risk-stratified care managementRisk-stratified care management

Quality CareQuality Care
Transition of care teamTransition of care team Performance measures to evaluate and Performance measures to evaluate and
improve care transitionsimprove care transitions Build community relationshipsBuild community relationships EHR-population health managementEHR-population health management
Patient-Centered CarePatient-Centered Care
Same day appointmentsSame day appointments Extended hoursExtended hours Self management: support and education, Self management: support and education,
Patient care action plans, home monitoring, Patient care action plans, home monitoring, Motivational InterviewingMotivational Interviewing
Communication with patients through email, web Communication with patients through email, web portalportal
Shared decision making, health coachShared decision making, health coach

LESSONS: LESSONS: 1.1. Team approach is critical-every team Team approach is critical-every team
member performing at the “top of their member performing at the “top of their license” license”
• Providers-providing evidence based medical care, medical Providers-providing evidence based medical care, medical reconciliation, multiple methods of communication/follow upreconciliation, multiple methods of communication/follow up
• Medical Assistants-giving vaccines, checking on health Medical Assistants-giving vaccines, checking on health maintenance, providing health maintenance, following up on maintenance, providing health maintenance, following up on referrals, testsreferrals, tests
• Nurses-following up for coordination of care (ER visit, Nurses-following up for coordination of care (ER visit, hospitalization, specialist), providing educationhospitalization, specialist), providing education
• Warm handoff to counselors, nutrition, other health professionalsWarm handoff to counselors, nutrition, other health professionals

2. Community Health workers are vital-2. Community Health workers are vital-provide trust in organization, education, provide trust in organization, education, community ties, help with community ties, help with language/cultural barrierslanguage/cultural barriers
3. Process-like a QI project-define 3. Process-like a QI project-define problem, select goals and how to change problem, select goals and how to change it, implement as team and then study it, implement as team and then study outcomeoutcome
CHALLENGES: CHALLENGES: Employee turn over, availabilityEmployee turn over, availability Team members and administration all Team members and administration all
have to have buy inhave to have buy in Cost- increased staffCost- increased staff Access in rural communitiesAccess in rural communities

The data and nothing but The data and nothing but the datathe data
Our data- We do Our data- We do great work! great work! And And we we have room for have room for improvement. improvement.
Why the team Why the team approach works to approach works to improve outcomes improve outcomes and quality of our and quality of our care.care.

Why teams?Why teams? Our main task is organizational!Our main task is organizational! The team approach works to improve outcomes and The team approach works to improve outcomes and
quality of care.quality of care. Patients value relationships with their health care Patients value relationships with their health care
workers above all else- smaller teams promote stronger workers above all else- smaller teams promote stronger relationships and improved continuity.relationships and improved continuity.
Interpersonal continuity of care is important to a Interpersonal continuity of care is important to a majority of patients, particularly those from vulnerable majority of patients, particularly those from vulnerable groups.groups.
We had a “team” of 75 people- now broken into teams We had a “team” of 75 people- now broken into teams of 7-8 peopleof 7-8 people

More functional teams- for More functional teams- for improved patient centered careimproved patient centered care
Everybody can’t be on one big team! 3-5 Everybody can’t be on one big team! 3-5 attendings, 9-10 residents, 4-5 PAs/nurse attendings, 9-10 residents, 4-5 PAs/nurse practitioners, 5 nurses, 20 MAs: about 50+ practitioners, 5 nurses, 20 MAs: about 50+ people!!people!!
Teams of 7-10 people are most functionalTeams of 7-10 people are most functional Functional units are characterized by “a small set Functional units are characterized by “a small set
of nodes with disproportionately high of nodes with disproportionately high connectedness.”connectedness.”
You can build this how we think it will work for your You can build this how we think it will work for your clinicclinic
The goal is effective coordination of careThe goal is effective coordination of care

What does the literature What does the literature say?say?
The literature supports a positive correlation between The literature supports a positive correlation between contact with primary care and demonstrated health contact with primary care and demonstrated health benefits.benefits.
North Carolina saved >$200 million per year in health North Carolina saved >$200 million per year in health care costs from 2003-2006 after care costs from 2003-2006 after instituting models of instituting models of PCMH which was attributed to effective PCMH which was attributed to effective coordination of care and a focus on preventative coordination of care and a focus on preventative care.care.
Practice characteristics such as patient registries, Practice characteristics such as patient registries, continuity, coordination and community orientation are continuity, coordination and community orientation are associated with improved population health.associated with improved population health.

Quit putting out fires, Quit putting out fires, prevent firesprevent fires
““Rather than uncoordinated, episodic Rather than uncoordinated, episodic care, we need to offer care that is well care, we need to offer care that is well organized, coordinated, integrated, organized, coordinated, integrated, characterized by effective characterized by effective communication, and based on communication, and based on continuous healing relationships.”continuous healing relationships.”
-Eric Larson-Eric Larson

We have room to improveWe have room to improve
We can work with less stress!We can work with less stress! We can improve patient outcomes and We can improve patient outcomes and
the quality of our work with more the quality of our work with more coordination.coordination.
Work smarter not harder!Work smarter not harder!

HgbA1CHgbA1C
Diabetes DX HgbA1C performed in Diabetes DX HgbA1C performed in last 6 months in our diabetic patients last 6 months in our diabetic patients in 2010 59%in 2010 59%
Out of 896 patients with Diabetes at Out of 896 patients with Diabetes at UNM SEH clinic in 2015 it is now UNM SEH clinic in 2015 it is now 65.5% and at some of our UNM clinics 65.5% and at some of our UNM clinics it has reached as high at 76%! And it has reached as high at 76%! And still rising. still rising.

LipidsLipids
Diabetes DX LDL performed in last 12 Diabetes DX LDL performed in last 12 months in 2010 months in 2010 59%59%
Out of 896 patients with Diabetes at Out of 896 patients with Diabetes at UNM SEH clinic in 2015 it is now UNM SEH clinic in 2015 it is now 67.4% and at some of our UNM clinics 67.4% and at some of our UNM clinics it has reached as high at 77.7%! And it has reached as high at 77.7%! And still rising. still rising.
ChangeChange

Why change?Why change? Improved patient outcomes and patient Improved patient outcomes and patient
satisfaction.satisfaction. This may help us enjoy our work more!This may help us enjoy our work more! Primary care could be abandoned by US Primary care could be abandoned by US
medical students who see it as a path to medical students who see it as a path to difficulty.difficulty.
Family Medicine should be leaders in Family Medicine should be leaders in implementing new and innovative ways to implementing new and innovative ways to deliver high-quality care. deliver high-quality care.
Yes We Can! Yes We Can!

Dream big!Dream big!
Our Vision of Our Vision of the Patient the Patient Centered Centered Medical Home Medical Home
How?How?
Chronic care model vs. acute care modelChronic care model vs. acute care model Planned visitsPlanned visits Advanced accessAdvanced access Patient Centered vs. Doctor CenteredPatient Centered vs. Doctor Centered Prevention integrated into all visit typesPrevention integrated into all visit types Warm handoffs to teammatesWarm handoffs to teammates IT supportIT support

PreventiveMedicine
SpecialtyCare
MedicalAssistants
MedicationRefills Acute Care
NursingCase
Manager
Test Results
HealthcareSupport
Team
ChronicDisease
Monitoring
PROVIDER
Traditional Work Flow Traditional Work Flow DesignDesign
Source: Southcentral Foundation, Anchorage AK

Parallel Work Flow Parallel Work Flow DesignDesign
MedicationRefills
ChronicDisease
Monitoring
TestResults
AcuteCare
PreventiveMedicine
Point of Care Testing
HealthcareSupport
Team
MedicalAssistants
Nursing
ProviderPROVIDER
Adapted from Southcentral Foundation, Anchorage AK
It takes a villageIt takes a village
We are all important members of the We are all important members of the healthcare team- we need optimize the healthcare team- we need optimize the role of each team member while role of each team member while maintaining our flexibility.maintaining our flexibility.
We should strive for less complexity.We should strive for less complexity. We need to consider the needs of our We need to consider the needs of our
population.population.

Essential ConceptsEssential Concepts
Each health care professional works to the Each health care professional works to the ““top of their licensetop of their license””
““Do today’s work today”Do today’s work today” ““Max Packing” Max Packing” each visiteach visit Integrate not just co-locate services, Integrate not just co-locate services,
especially behavioral health and pharmacyespecially behavioral health and pharmacy Between visit care as important as during Between visit care as important as during
visit carevisit care Joy in the work place!Joy in the work place!
Components of Planned Components of Planned VisitVisit
1.1. Pre-Visit data collection Pre-Visit data collection 2.2. Pre-Visit patient call Pre-Visit patient call 3.3. Standing orders Standing orders 4.4. Visit pre-work includes Health Maintenance, Condition Visit pre-work includes Health Maintenance, Condition
Management, Previous encounter notes Management, Previous encounter notes 5.5. HuddleHuddle6.6. Activity setting before or after clinician encounterActivity setting before or after clinician encounter7.7. Summary of visit to patientSummary of visit to patient8.8. Enrollment in Patient PortalEnrollment in Patient Portal9.9. Tracking referrals and ordered testsTracking referrals and ordered tests
Nurse Goal SettingNurse Goal Setting
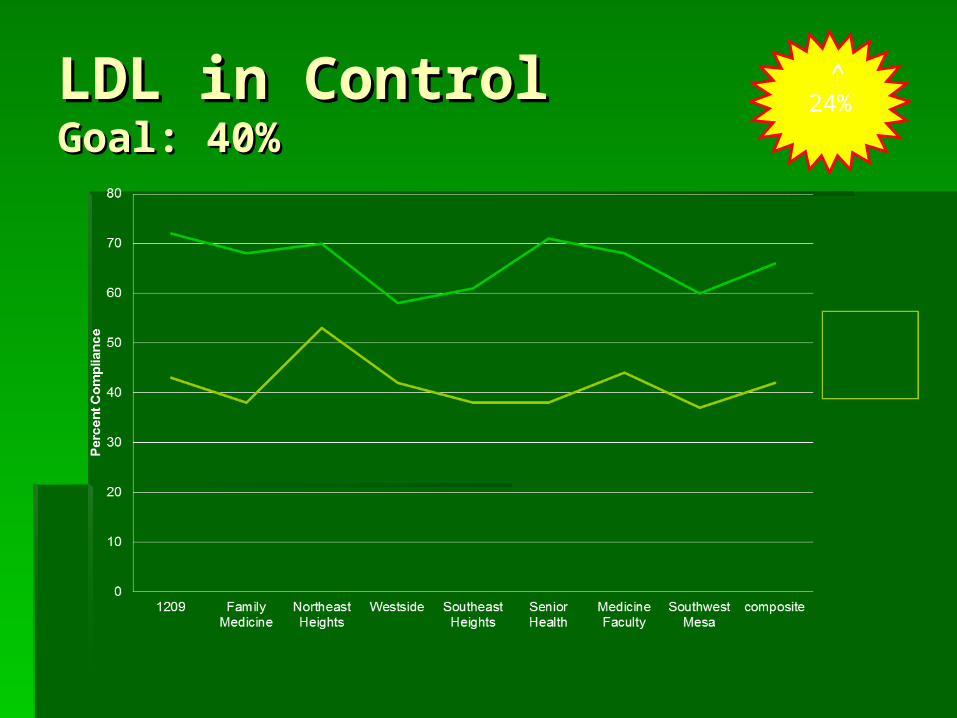
LDL in ControlLDL in ControlGoal: 40%Goal: 40%
24%

HgA1C in ControlHgA1C in ControlGoal: 40%Goal: 40% 26%


TeamworkTeamwork
TeamsTeams
Team formation Team formation What makes up a functional What makes up a functional
unit? - usually no more that 7 -10 unit? - usually no more that 7 -10 peoplepeople
Physician, midlevel (PA/NP), RN, Physician, midlevel (PA/NP), RN, Mas--- patient in the center!Mas--- patient in the center!

Ease of practiceEase of practice
Help us! what can the system do to help Help us! what can the system do to help providers be more efficient and patient providers be more efficient and patient centered?centered?
Every team member is functioning to the Every team member is functioning to the very top of their ability.very top of their ability.
Providers are left with work that Providers are left with work that only they only they can do.can do.
Providers don’t triage the messages!Providers don’t triage the messages! Providers don’t discharge patients!Providers don’t discharge patients!

Pre-visit InformationPre-visit Information
Diagnosis- problem list is being updatedDiagnosis- problem list is being updated Patient registry-problem list gets people on Patient registry-problem list gets people on
registryregistry Look at future patient list together? When?Look at future patient list together? When? Standardized orders for HCMStandardized orders for HCM Standardized visits on each teamStandardized visits on each team Labs ordered before visit- patients calledLabs ordered before visit- patients called How can this work?How can this work? Preventative Maintenance protocolsPreventative Maintenance protocols

What’s next for you?What’s next for you?
Start dateStart date Motivational interviewing training?Motivational interviewing training? Group visits? DM2, depression, prenatal, Group visits? DM2, depression, prenatal,
well childwell child Constant quality improvement (QI) in Constant quality improvement (QI) in
areas of diabetes, dyslipidemia, areas of diabetes, dyslipidemia, hypertension, obesity and metabolic hypertension, obesity and metabolic syndrome.syndrome.
Education for nurses in chronic care Education for nurses in chronic care management- nurse education visitsmanagement- nurse education visits
NCQA PCMH RecognitionNCQA PCMH Recognition
20102010
12 UNMH Clinics 12 UNMH Clinics
Level 1Level 1

NCQA PCMH Recognition at NCQA PCMH Recognition at UNM Status 2015 Level 3!UNM Status 2015 Level 3!
1.1. TrumanTruman2.2. Young Children’s Health CareYoung Children’s Health Care3.3. Carrie Tingley PediatricsCarrie Tingley Pediatrics4.4. General Pediatric ClinicGeneral Pediatric Clinic5.5. ASAP Primary CareASAP Primary Care6.6. Family Medicine Family Medicine 7.7. Northeast Heights Northeast Heights 8.8. Southeast Heights Southeast Heights 9.9. WestsideWestside10.10. 1209120911.11. Senior HealthSenior Health12.12. Southwest Mesa Southwest Mesa
SRMC, Atrisco HHS too early to apply

Who’s on the Clinical Who’s on the Clinical Care TeamCare Team
1.1. Clinic NursesClinic Nurses2.2. Medical AssistantsMedical Assistants3.3. Nurse Practitioners and Physician AssistantsNurse Practitioners and Physician Assistants4.4. Pharmacy CliniciansPharmacy Clinicians5.5. Behavioral HealthBehavioral Health6.6. Nurse Case ManagersNurse Case Managers7.7. Clinical Social WorkersClinical Social Workers8.8. Physical Therapists, PodiatristsPhysical Therapists, Podiatrists9.9. Special Programs, Milagro and FocusSpecial Programs, Milagro and Focus

Why Recognize PCMH?Why Recognize PCMH?
1.1. Patient satisfactionPatient satisfaction
2.2. Doctor satisfactionDoctor satisfaction
3.3. Demand for primary care expandingDemand for primary care expanding
4.4. Current system rewards high volume acute Current system rewards high volume acute care, specialized care and procedures not care, specialized care and procedures not coordinated, comprehensive, continuouscoordinated, comprehensive, continuous
5.5. Triple Aim + Ease of Practice= quadruple Triple Aim + Ease of Practice= quadruple aimaim

91%91%believe it is important to have believe it is important to have
one place or doctor responsible for their primary one place or doctor responsible for their primary carecare
and for coordinating care between practitionersand for coordinating care between practitioners

Political SupportPolitical Support
PPACA, State fundingPPACA, State funding
InsuranceInsurance
Business EndorsementBusiness Endorsement
AMA Joint PrinciplesAMA Joint Principles
Specialty OrganizationsSpecialty Organizations

Specialty Organizations Specialty Organizations Endorse PCMHEndorse PCMH
1.1. The American Academy of Chest Physicians The American Academy of Chest Physicians 2.2. The American Academy of Hospice and Palliative Medicine The American Academy of Hospice and Palliative Medicine 3.3. The American Academy of Neurology The American Academy of Neurology 4.4. The American College of Cardiology The American College of Cardiology 5.5. The American College of Osteopathic Family Physicians The American College of Osteopathic Family Physicians 6.6. The American College of Osteopathic Internists The American College of Osteopathic Internists 7.7. The American Geriatrics Society The American Geriatrics Society 8.8. The American Medical Directors Association The American Medical Directors Association 9.9. The American Society of Addiction Medicine The American Society of Addiction Medicine 10.10. The American Society of Clinical Oncology The American Society of Clinical Oncology 11.11. The Society for Adolescent Medicine The Society for Adolescent Medicine 12.12. The Society of Critical Care Medicine The Society of Critical Care Medicine 13.13. The Society of General Internal Medicine The Society of General Internal Medicine

New Clinic AccessNew Clinic Access
2012 SRMC2012 SRMC 2013 AHHS2013 AHHS 2015 North Valley2015 North Valley 2016 South Valley2016 South Valley 2017 Paseo2017 Paseo 2018 Heights2018 Heights
Questions and CommentsQuestions and Comments

Impact on Triple Aim + Impact on Triple Aim +
SatisfactionSatisfaction
•CostCost•ED, UCC, Re-ED, UCC, Re-admitadmit•Population healthPopulation health•Preventive Preventive servicesservices•AccessAccess•Patient Patient satisfactionsatisfaction•Doctor satisfactionDoctor satisfaction
Patient-Centered Primary Care CollaborativeAnnual Update January 2015

References:References:
J Ark Med Soc. 2012 Jun;108(13):300-3. 2012 Jun;108(13):300-3. Bringing home the patient centered Bringing home the patient centered
medical home: lessons learned from medical home: lessons learned from an academic family medical center.an academic family medical center.
Howard J11, , White P, Chronister K, , Chronister K, Balamurugan A.Balamurugan A.
PCMH model AAFP PCMH model AAFP

Key ResourcesKey Resources
AHRQ PCMH Resource Center, See handout AHRQ PCMH Resource Center, See handout Foundational Articles Foundational Articles http://www.pcmh.ahrq.gov/portal/server.pt/community/pcmh__home/148http://www.pcmh.ahrq.gov/portal/server.pt/community/pcmh__home/14833
AAFP and TransforMed www.aafp.orgAAFP and TransforMed www.aafp.org
Patient Centered Primary Care Collaborative http://pcpcc.net/what-we-Patient Centered Primary Care Collaborative http://pcpcc.net/what-we-dodo
NCQA http://ncqa.org/tabid/631/Default.aspxNCQA http://ncqa.org/tabid/631/Default.aspx
Summary of the National Demonstration Project and Recommendations Summary of the National Demonstration Project and Recommendations for the PCMH www.annfammed.org/cgi/content/abstract/8/Suppl_1/S80for the PCMH www.annfammed.org/cgi/content/abstract/8/Suppl_1/S80
Top Related