







Languages
Pages
Legal


Oral Hypoglycemic
AgentsH.Rezvanian.MD
Objectives
1. List oral hypoglycemic agents currently on the market
2. Classify oral hypoglycemic agents based on their mechanism, onset, duration, and place in therapy
3. Describe pros and cons of the different oral hypoglycemic agents available
4. Summarize limitations and contraindications of oral hypoglycemic agents
Classification and Diagnosis
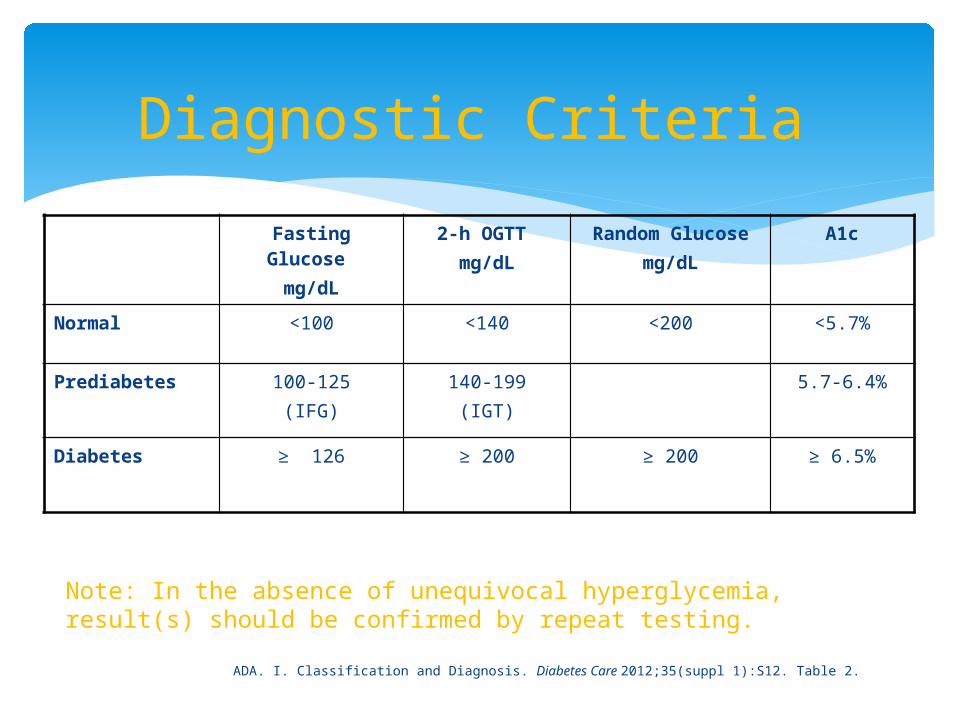
Diagnostic Criteria
Fasting Glucose mg/dL
2-h OGTT mg/dL
Random Glucosemg/dL
A1c
Normal <100 <140 <200 <5.7%
Prediabetes 100-125(IFG)
140-199(IGT)
5.7-6.4%
Diabetes ≥ 126 ≥ 200 ≥ 200 ≥ 6.5%
ADA. I. Classification and Diagnosis. Diabetes Care 2012;35(suppl 1):S12. Table 2.
Note: In the absence of unequivocal hyperglycemia, result(s) should be confirmed by repeat testing.
Prevention, Prevention, Prevention!
Refer patients with IGT, IFG, or A1C 5.7–6.4% to ongoing support program Target weight loss = 7% of total body weight Minimum of 150 min/week of moderate physical activity
Follow-up counseling important for success
Based on cost-effectiveness of diabetes prevention, third-party payers should cover such programs
In those with pre-diabetes, monitor for development of diabetes annually
ADA. IV. Prevention/Delay of Type 2 Diabetes. Diabetes Care 2012;35(suppl 1):S16
Prevention, Prevention, Prevention!
Medications shown to delay progression of IGT/IFG to T2DM Metformin (US DPP, NEJM 2002) Acarbose (STOP-NIDDM, Lancet 2002) Pioglitazone (ACT NOW, presentation 2008)
Consider metformin for prevention of type 2 diabetes if IGT, IFG, or A1C 5.7–6.4% Especially for those with BMI >35 kg/m2, age <60 years, and
women with prior GDM
None are FDA approved for Diabetes Prevention
ADA. IV. Prevention/Delay of Type 2 Diabetes. Diabetes Care 2012;35(suppl 1):S16
A1c Monitoring
Twice Yearly in those who have stable glycemic control and no therapy changes
Quarterly in patients whose therapy has changed or who are not meeting glycemic goals
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S18.
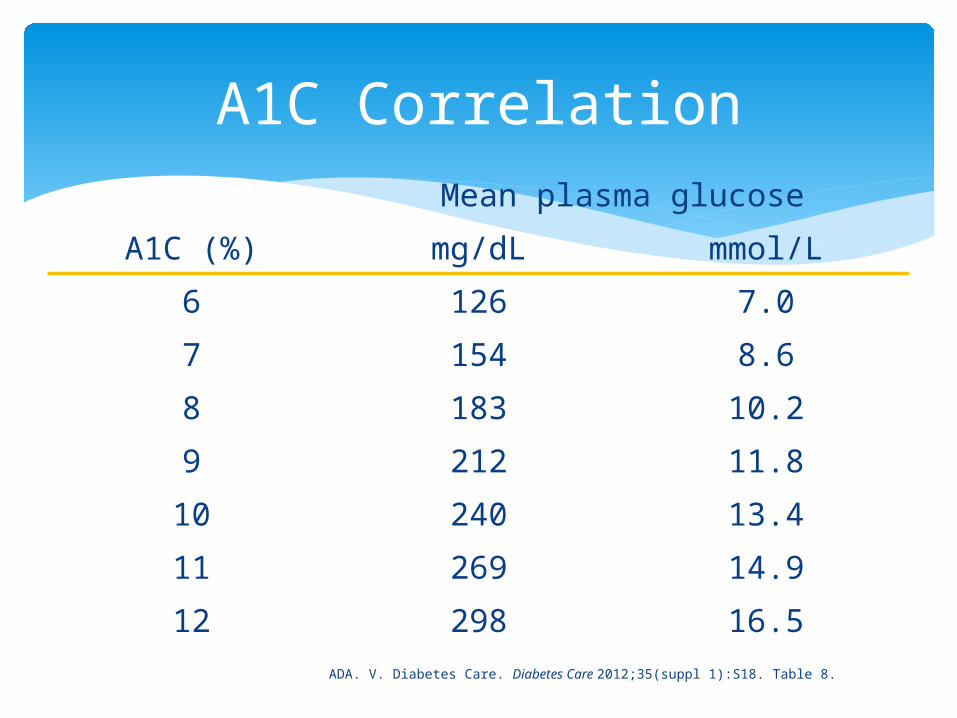
A1C CorrelationMean plasma glucose
A1C (%) mg/dL mmol/L
6 126 7.0
7 154 8.6
8 183 10.2
9 212 11.8
10 240 13.4
11 269 14.9
12 298 16.5
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S18. Table 8.
Easy A1c Correlation
NOTE: This is an estimate only
(A1C -2) x 30 i.e. A1C= 7%; (7-2) x30 = 150mg/dL
Goals
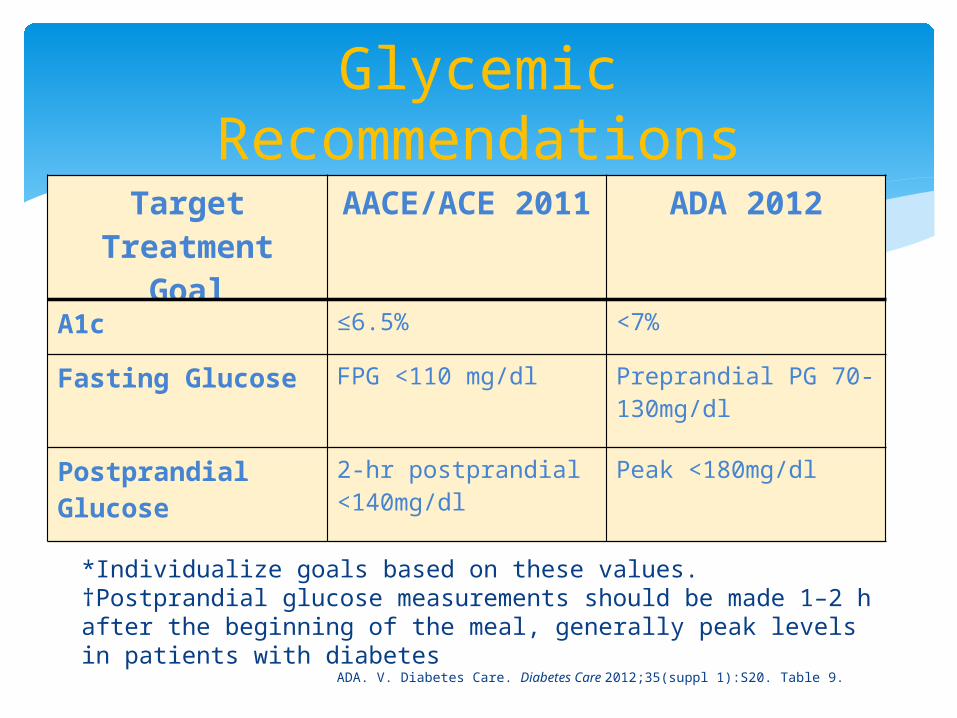
Glycemic Recommendations
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S20. Table 9.
*Individualize goals based on these values.†Postprandial glucose measurements should be made 1–2 h after the beginning of the meal, generally peak levels in patients with diabetes
Target Treatment
Goal
AACE/ACE 2011
ADA 2012
A1c ≤6.5% <7%
Fasting Glucose FPG <110 mg/dl Preprandial PG 70-130mg/dl
Postprandial Glucose
2-hr postprandial <140mg/dl
Peak <180mg/dl
Goals: A1c
Goal: <7% Lowering A1c <7% has been shown to reduce microvascular
complications and, if implemented soon after the diagnosis of diabetes, is associated with long-term reduction in macrovascular disease More stringent goals (i.e. 6.5%)are reasonable in patients if
it can be achieved without significant hypoglycemia or side effect New diagnosis of diabetes, long life expectancy and no
significant CVD
Less stringent goals (i.e. 8%) may be reasonable for those who have experienced severe hypoglycemia, limited life expectancy, advanced complications, or extensive comorbidities.
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S18-19.

Oral Hypoglycemic Treatment
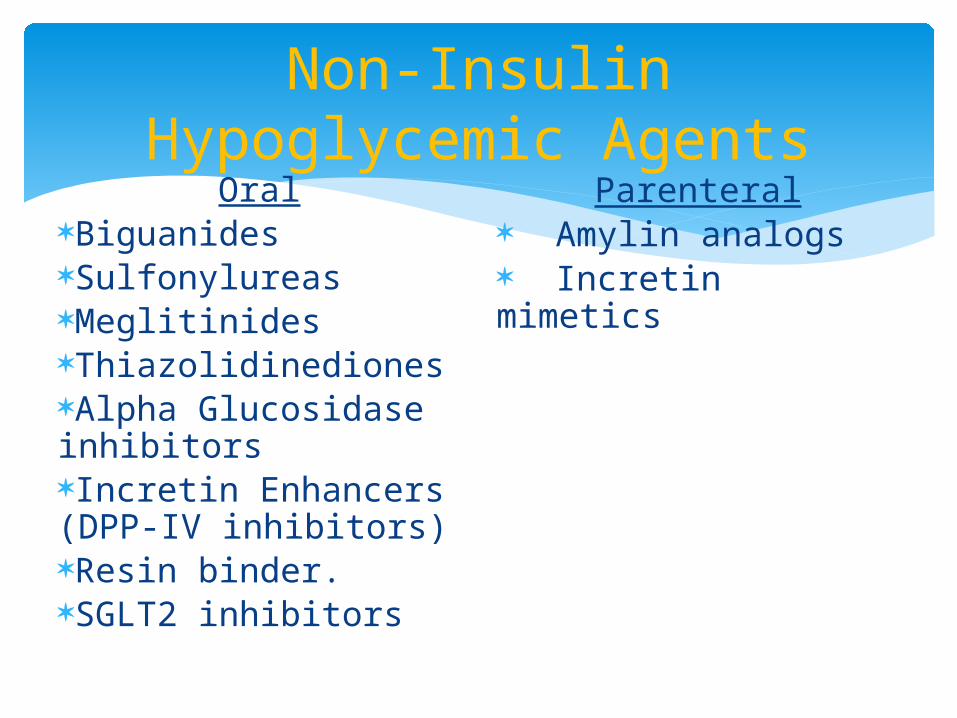
Non-Insulin Hypoglycemic Agents
OralBiguanidesSulfonylureasMeglitinidesThiazolidinedionesAlpha Glucosidase inhibitorsIncretin Enhancers (DPP-IV inhibitors)Resin binder.SGLT2 inhibitors
Parenteral Amylin analogs Incretin mimetics
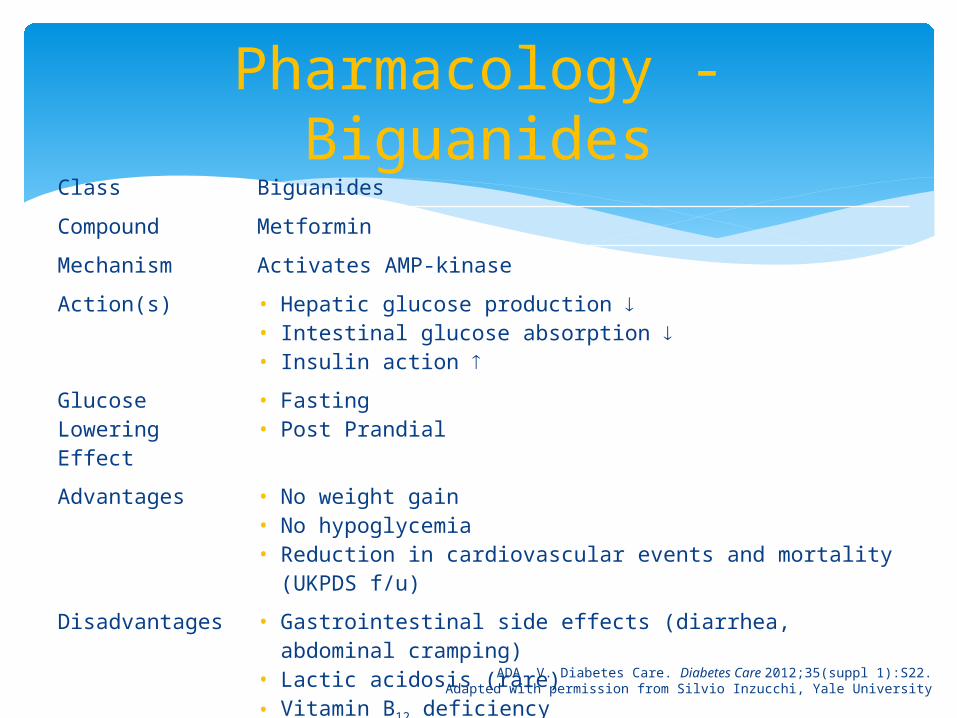
Pharmacology - Biguanides
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S22.Adapted with permission from Silvio Inzucchi, Yale University
Class Biguanides
Compound Metformin
Mechanism Activates AMP-kinase
Action(s) • Hepatic glucose production • Intestinal glucose absorption • Insulin action
Glucose Lowering Effect
• Fasting• Post Prandial
Advantages • No weight gain• No hypoglycemia• Reduction in cardiovascular events and mortality (UKPDS
f/u)
Disadvantages • Gastrointestinal side effects (diarrhea, abdominal cramping)
• Lactic acidosis (rare)• Vitamin B12 deficiency• Contraindications: reduced kidney function
Cost Low – free at Marsh
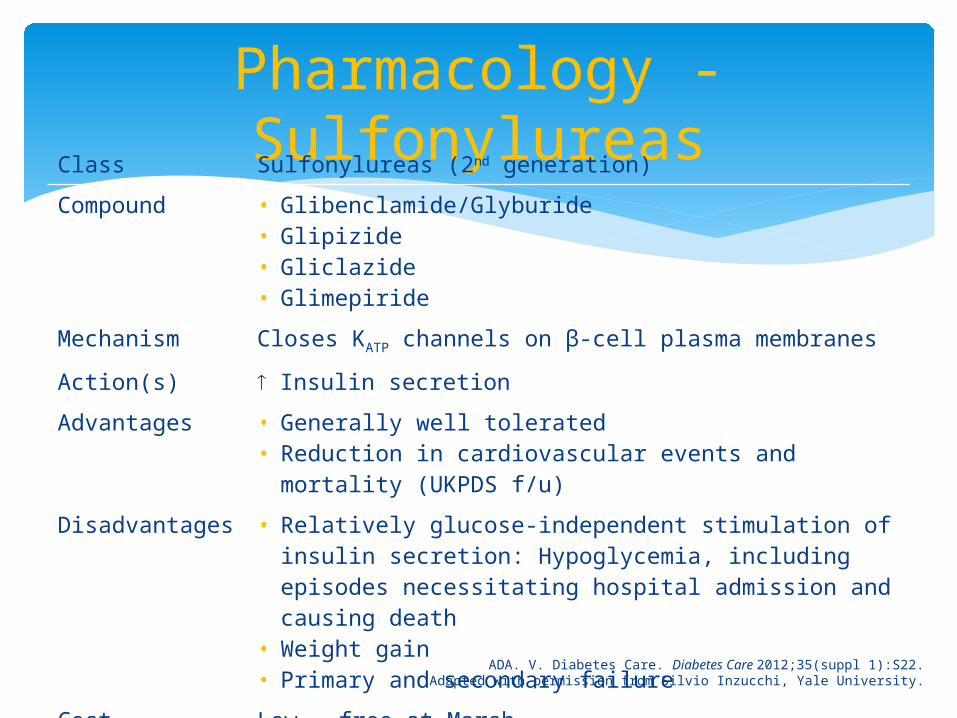
Pharmacology - Sulfonylureas
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S22.Adapted with permission from Silvio Inzucchi, Yale University.
Class Sulfonylureas (2nd generation)
Compound • Glibenclamide/Glyburide• Glipizide• Gliclazide• Glimepiride
Mechanism Closes KATP channels on β-cell plasma membranes
Action(s) Insulin secretion
Advantages • Generally well tolerated• Reduction in cardiovascular events and mortality
(UKPDS f/u)
Disadvantages • Relatively glucose-independent stimulation of insulin secretion: Hypoglycemia, including episodes necessitating hospital admission and causing death
• Weight gain• Primary and secondary failure
Cost Low – free at Marsh
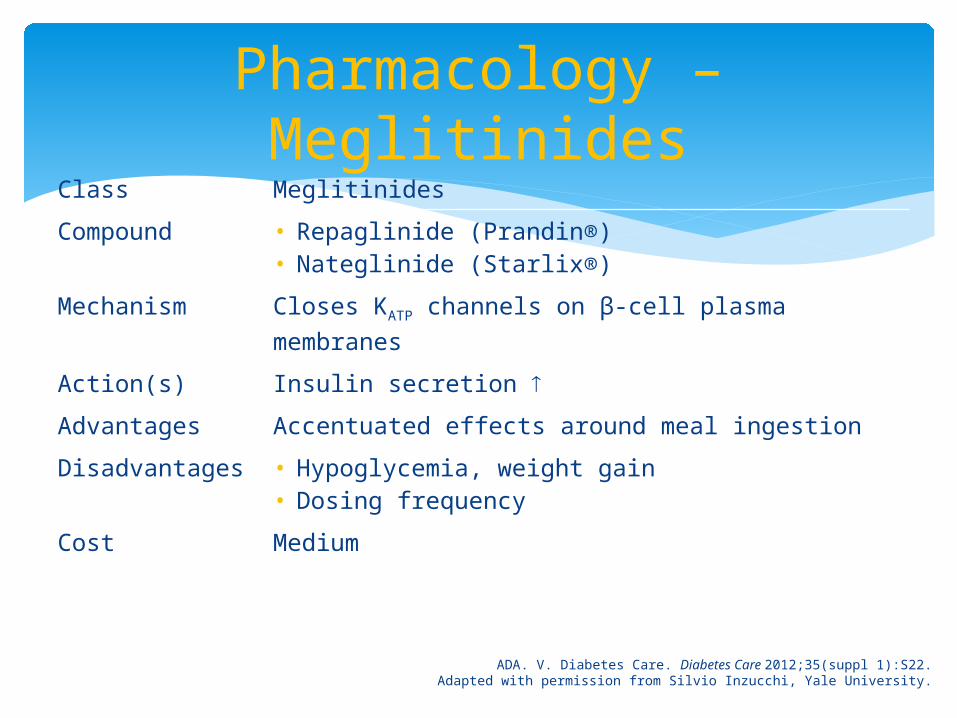
Pharmacology – Meglitinides
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S22.Adapted with permission from Silvio Inzucchi, Yale University.
Class Meglitinides
Compound • Repaglinide (Prandin®)• Nateglinide (Starlix®)
Mechanism Closes KATP channels on β-cell plasma membranes
Action(s) Insulin secretion
Advantages Accentuated effects around meal ingestion
Disadvantages • Hypoglycemia, weight gain• Dosing frequency
Cost Medium
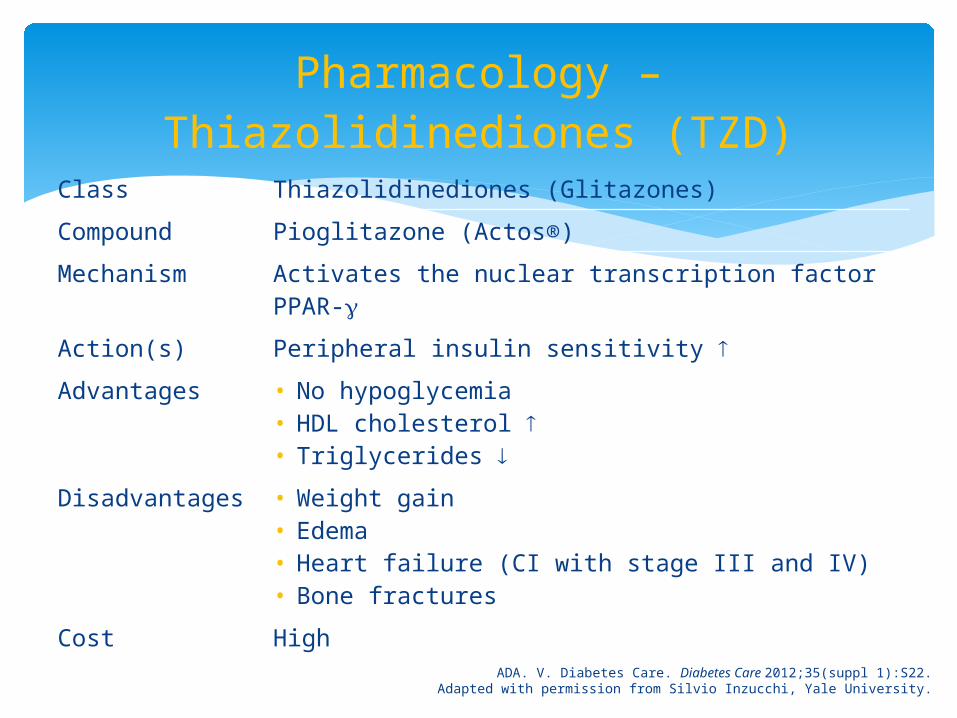
Pharmacology – Thiazolidinediones (TZD)
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S22.Adapted with permission from Silvio Inzucchi, Yale University.
Class Thiazolidinediones (Glitazones)
Compound Pioglitazone (Actos®)
Mechanism Activates the nuclear transcription factor PPAR-
Action(s) Peripheral insulin sensitivity
Advantages • No hypoglycemia• HDL cholesterol • Triglycerides
Disadvantages • Weight gain• Edema• Heart failure (CI with stage III and IV)• Bone fractures
Cost High
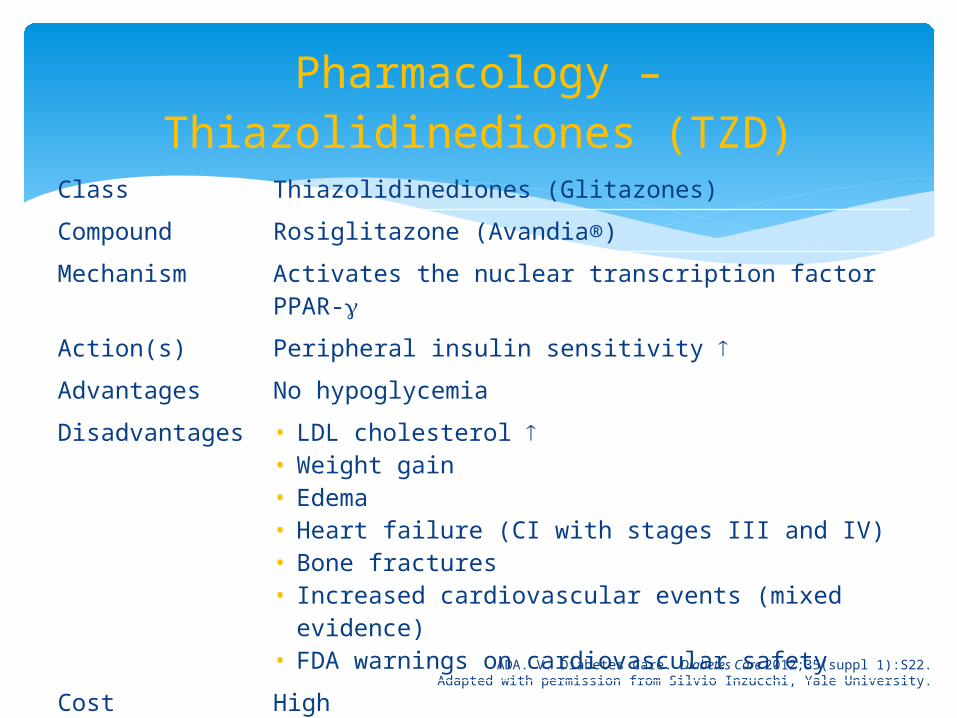
Pharmacology – Thiazolidinediones (TZD)
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S22.Adapted with permission from Silvio Inzucchi, Yale University.
Class Thiazolidinediones (Glitazones)
Compound Rosiglitazone (Avandia®)
Mechanism Activates the nuclear transcription factor PPAR-
Action(s) Peripheral insulin sensitivity
Advantages No hypoglycemia
Disadvantages • LDL cholesterol • Weight gain• Edema• Heart failure (CI with stages III and IV)• Bone fractures• Increased cardiovascular events (mixed evidence)• FDA warnings on cardiovascular safety
Cost High
TZDs and the FDA
Rosiglitazone Restricted by FDA – can only be used by patients
currently benefiting from therapy or do not get adequate DM treatment from other agents and not willing to use pioglitazone
1-800-AVANDIA
Pioglitazone FDA alert – ongoing analysis of risk of bladder
cancer (with prolonged use >12 months) Lexi-Drugs Online [Internet]. Hudson (OH) : Lexi-Comp, Inc. 1978-2012[cited 2012 August 1].
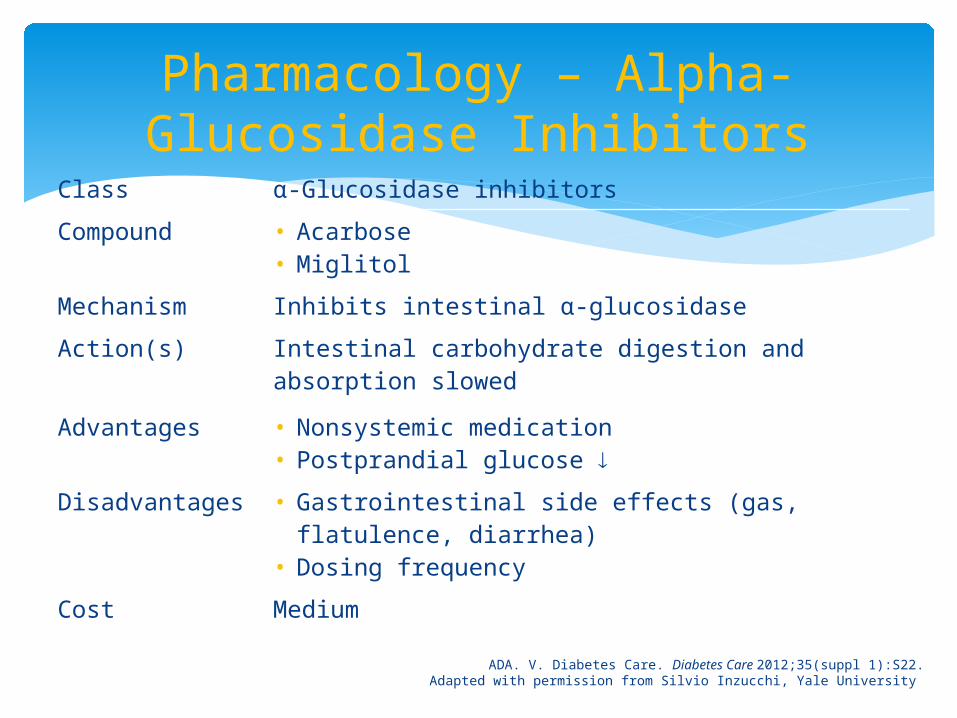
Pharmacology – Alpha-Glucosidase Inhibitors
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S22.Adapted with permission from Silvio Inzucchi, Yale University.
Class α-Glucosidase inhibitors
Compound • Acarbose• Miglitol
Mechanism Inhibits intestinal α-glucosidase
Action(s) Intestinal carbohydrate digestion and absorption slowed
Advantages • Nonsystemic medication• Postprandial glucose
Disadvantages • Gastrointestinal side effects (gas, flatulence, diarrhea)
• Dosing frequency
Cost Medium
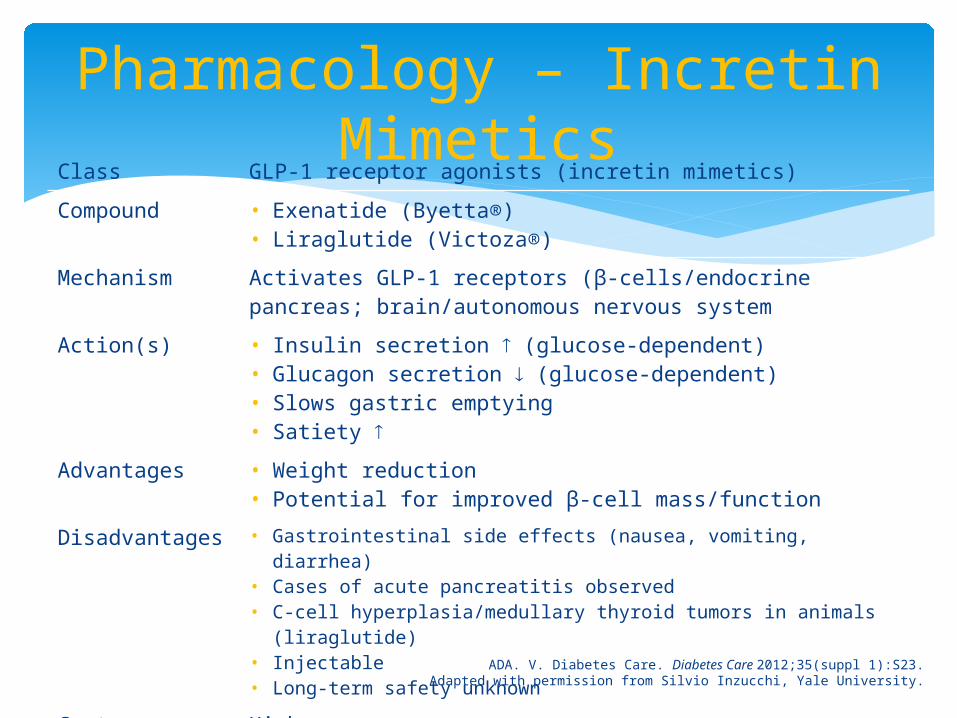
Pharmacology – Incretin Mimetics
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S23.Adapted with permission from Silvio Inzucchi, Yale University.
Class GLP-1 receptor agonists (incretin mimetics)
Compound • Exenatide (Byetta®)• Liraglutide (Victoza®)
Mechanism Activates GLP-1 receptors (β-cells/endocrine pancreas; brain/autonomous nervous system
Action(s) • Insulin secretion (glucose-dependent)• Glucagon secretion (glucose-dependent)• Slows gastric emptying• Satiety
Advantages • Weight reduction• Potential for improved β-cell mass/function
Disadvantages • Gastrointestinal side effects (nausea, vomiting, diarrhea)• Cases of acute pancreatitis observed• C-cell hyperplasia/medullary thyroid tumors in animals
(liraglutide)• Injectable• Long-term safety unknown
Cost High
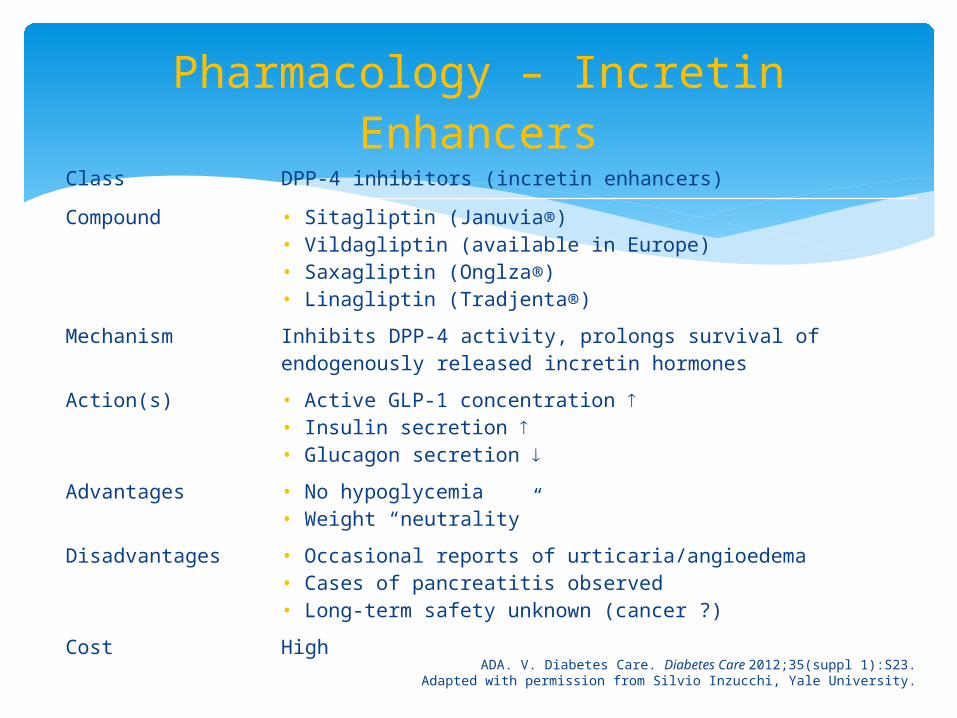
Pharmacology – Incretin Enhancers
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S23.Adapted with permission from Silvio Inzucchi, Yale University.
Class DPP-4 inhibitors (incretin enhancers)
Compound • Sitagliptin (Januvia®)• Vildagliptin (available in Europe)• Saxagliptin (Onglza®)• Linagliptin (Tradjenta®)
Mechanism Inhibits DPP-4 activity, prolongs survival of endogenously released incretin hormones
Action(s) • Active GLP-1 concentration • Insulin secretion • Glucagon secretion
Advantages • No hypoglycemia• Weight “neutrality”
Disadvantages • Occasional reports of urticaria/angioedema• Cases of pancreatitis observed• Long-term safety unknown (cancer ?)
Cost High
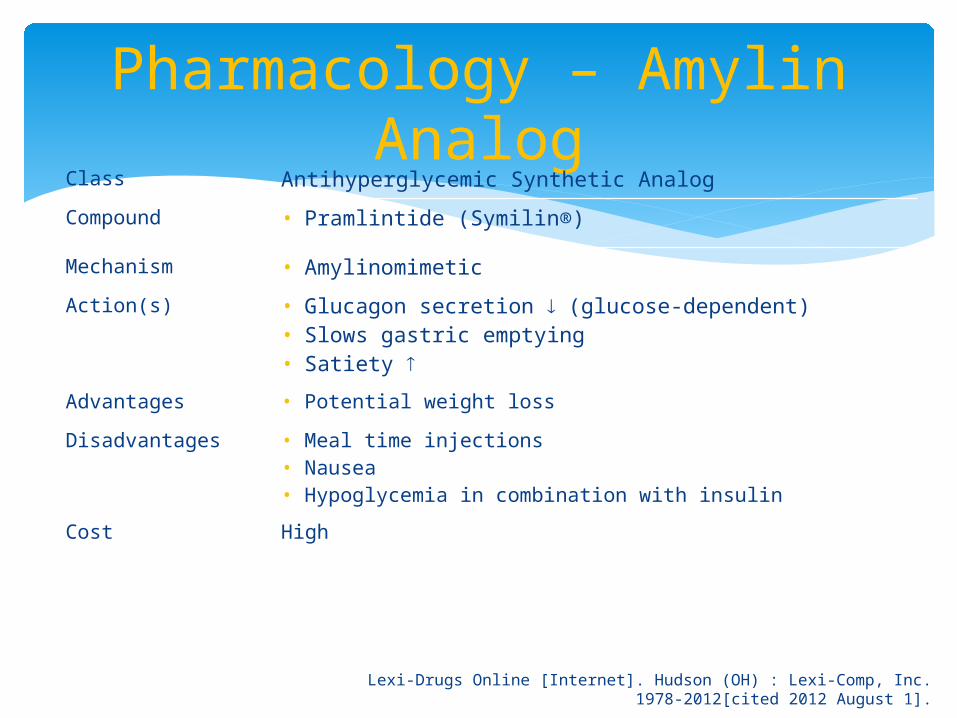
Pharmacology – Amylin Analog
Class Antihyperglycemic Synthetic Analog
Compound • Pramlintide (Symilin®)
Mechanism • Amylinomimetic
Action(s) • Glucagon secretion (glucose-dependent)• Slows gastric emptying• Satiety
Advantages • Potential weight loss
Disadvantages • Meal time injections• Nausea• Hypoglycemia in combination with insulin
Cost High
Lexi-Drugs Online [Internet]. Hudson (OH) : Lexi-Comp, Inc. 1978-2012[cited 2012 August 1].
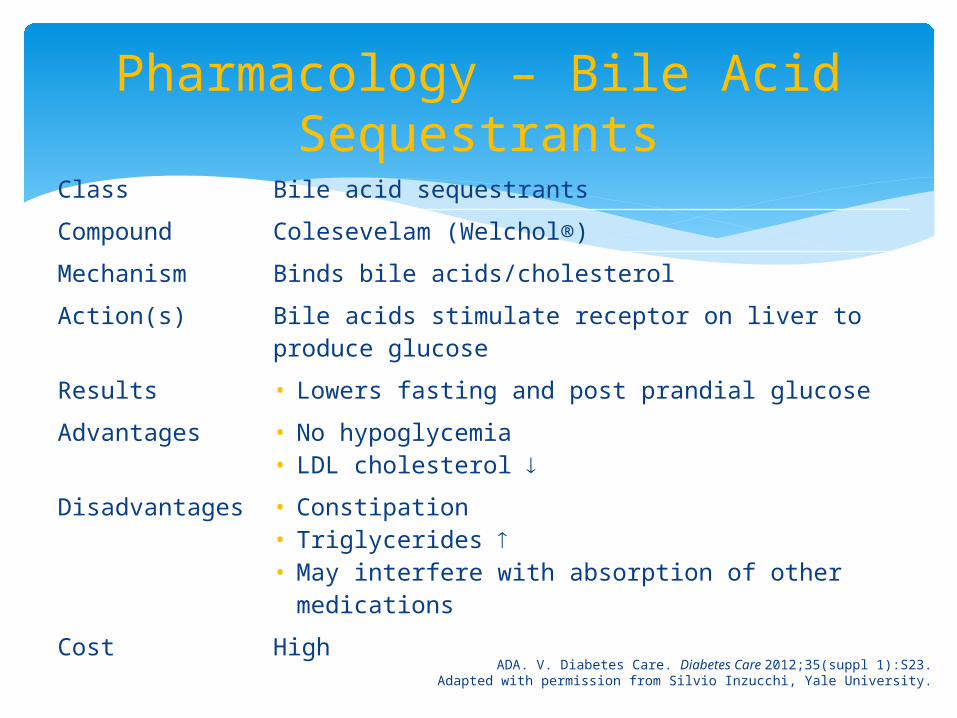
Pharmacology – Bile Acid Sequestrants
ADA. V. Diabetes Care. Diabetes Care 2012;35(suppl 1):S23.Adapted with permission from Silvio Inzucchi, Yale University.
Class Bile acid sequestrants
Compound Colesevelam (Welchol®)
Mechanism Binds bile acids/cholesterol
Action(s) Bile acids stimulate receptor on liver to produce glucose
Results • Lowers fasting and post prandial glucose
Advantages • No hypoglycemia• LDL cholesterol
Disadvantages • Constipation• Triglycerides • May interfere with absorption of other
medications
Cost High
The Role of SGLT-2 Inhibitors in the Management of Patients
with Type 2 Diabetes
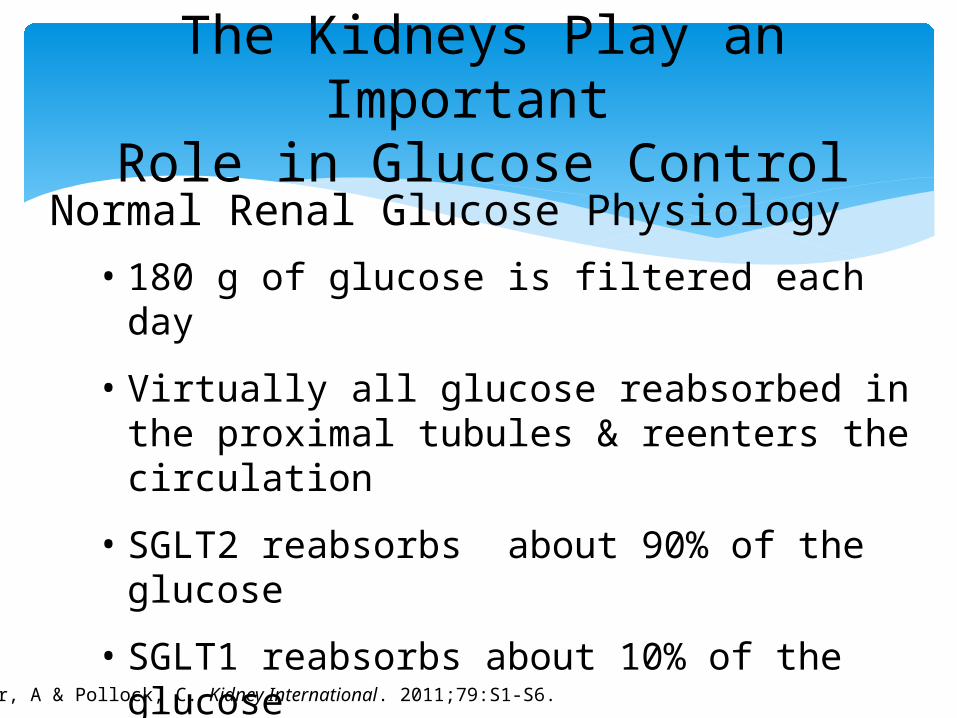
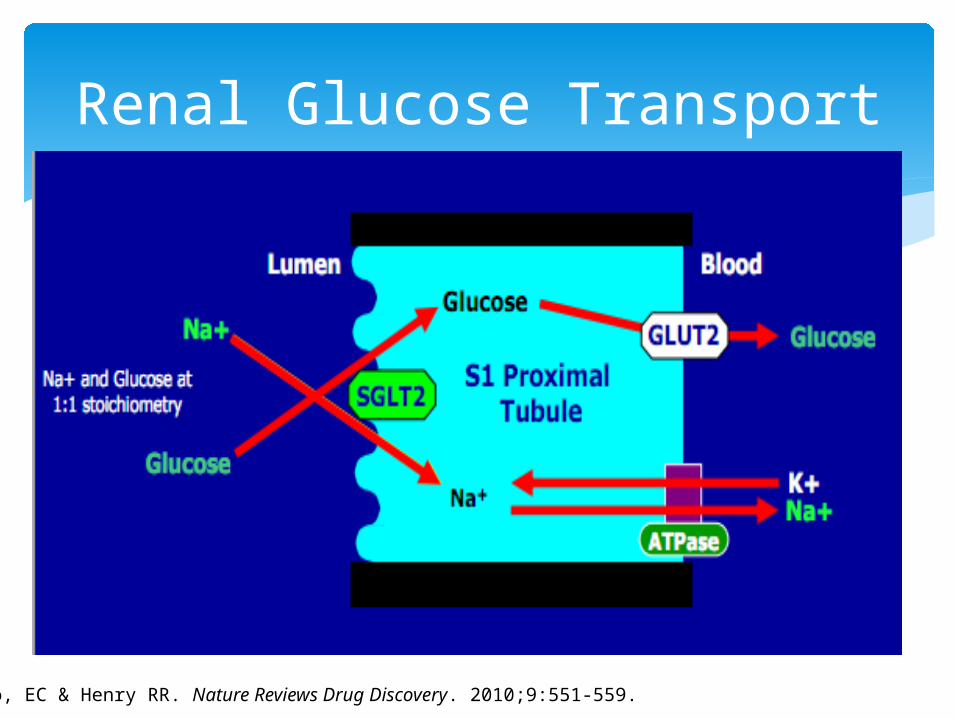
Normal Renal Glucose Physiology• 180 g of glucose is filtered each day
• Virtually all glucose reabsorbed in the proximal tubules & reenters the circulation
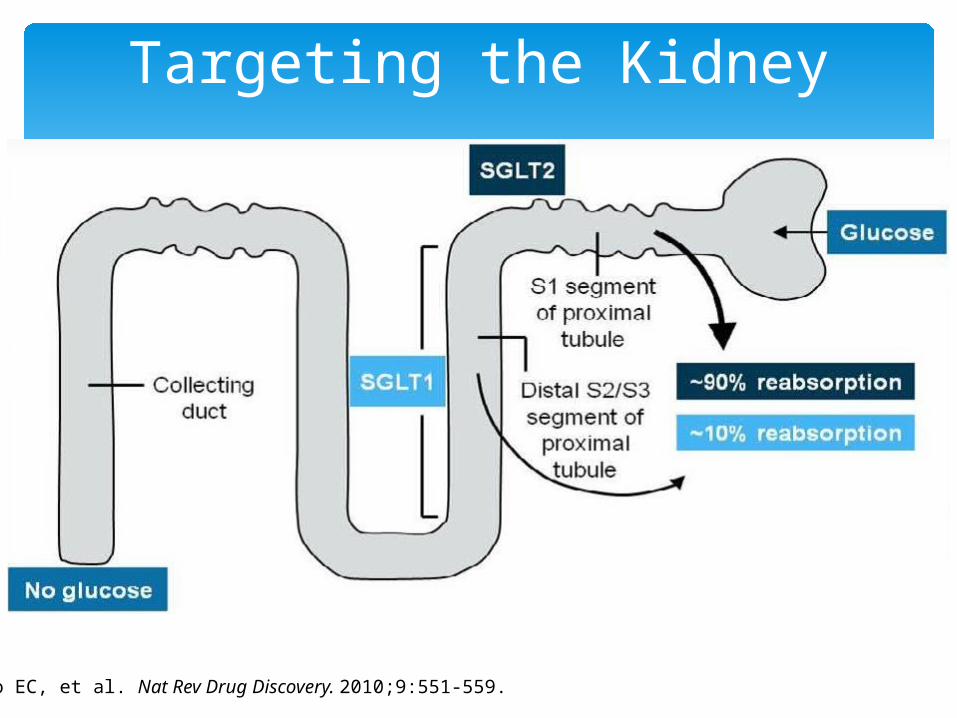
• SGLT2 reabsorbs about 90% of the glucose
• SGLT1 reabsorbs about 10% of the glucose
• Virtually no glucose excreted in urine
The Kidneys Play an Important Role in Glucose Control
Mather, A & Pollock, C. Kidney International. 2011;79:S1-S6.
Chao EC, et al. Nat Rev Drug Discovery. 2010;9:551-559.
Targeting the Kidney
Chao, EC & Henry RR. Nature Reviews Drug Discovery. 2010;9:551-559.
Renal Glucose Transport
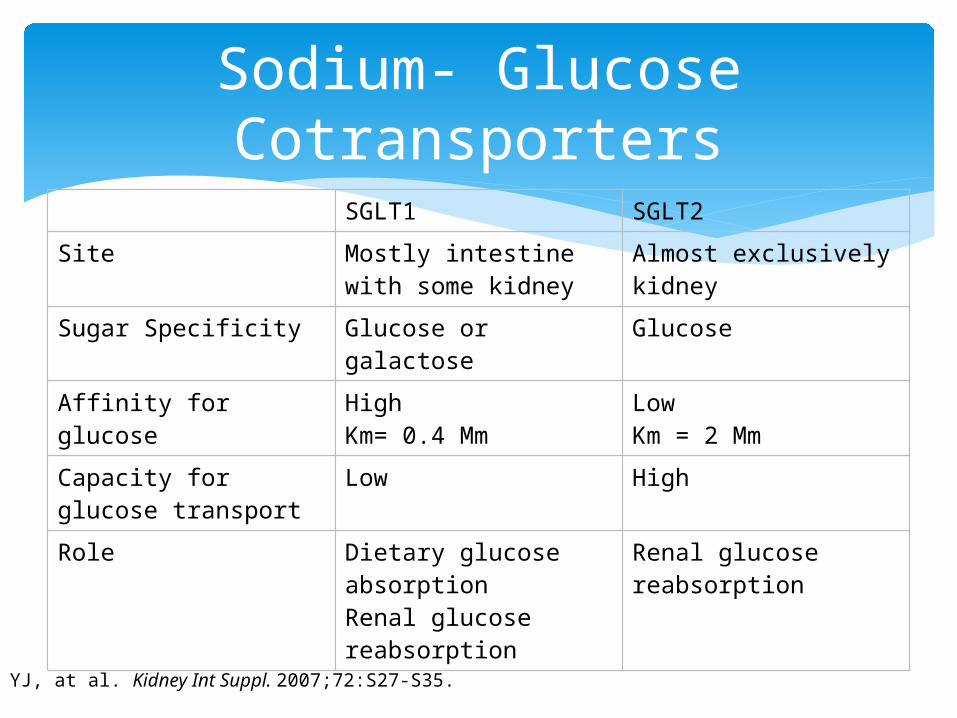
Sodium- Glucose Cotransporters
SGLT1 SGLT2
Site Mostly intestine with some kidney
Almost exclusively kidney
Sugar Specificity Glucose or galactose Glucose
Affinity for glucose HighKm= 0.4 Mm
Low Km = 2 Mm
Capacity for glucose transport
Low High
Role Dietary glucose absorptionRenal glucose reabsorption
Renal glucose reabsorption
Lee YJ, at al. Kidney Int Suppl. 2007;72:S27-S35.
Familial Renal Glucosuria: A Genetic Model of SGLT2 Inhibition
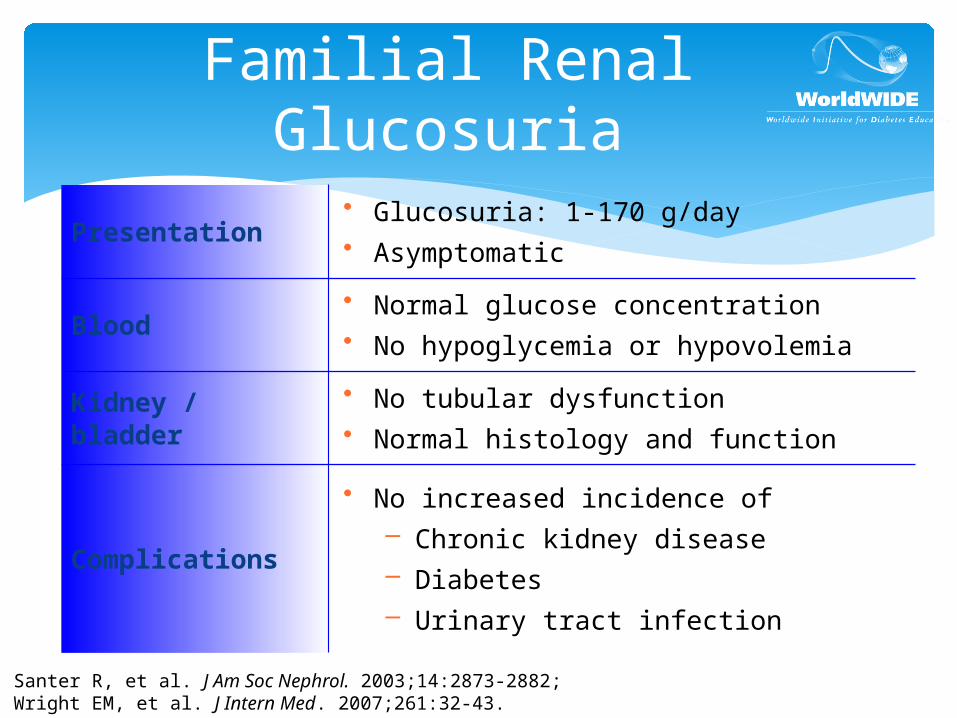
Familial Renal Glucosuria
Presentation• Glucosuria: 1-170 g/day• Asymptomatic
Blood• Normal glucose concentration• No hypoglycemia or hypovolemia
Kidney / bladder• No tubular dysfunction• Normal histology and function
Complications
• No increased incidence of– Chronic kidney disease– Diabetes– Urinary tract infection
Santer R, et al. J Am Soc Nephrol. 2003;14:2873-2882;Wright EM, et al. J Intern Med. 2007;261:32-43.
Altered Renal Glucose Control in Diabetes
Gluconeogenesis is increased in postprandial and postabsorptive states in patients with Type 2 DM Renal contribution to hyperglycemia 3-fold increase relative to patients without diabetes
Glucose reabsorption Increased SGLT-2 expression and activity in renal
epithelial cells from patients with diabetes vs. normoglycemic individuals Marsenic O. Am J Kidney Dis. 2009;53:875-883.
Bakris GL, et al. Kidney Int. 2009;75(12):1272-1277. Rahmoune H, et al. Diabetes. 2005;54(12):3427-3434.
SGLT2 Inhibitors in Phase 3 Development
• Empagliflozin
• Canagliflozin
• Dapagliflozin
• Ipragliflozin
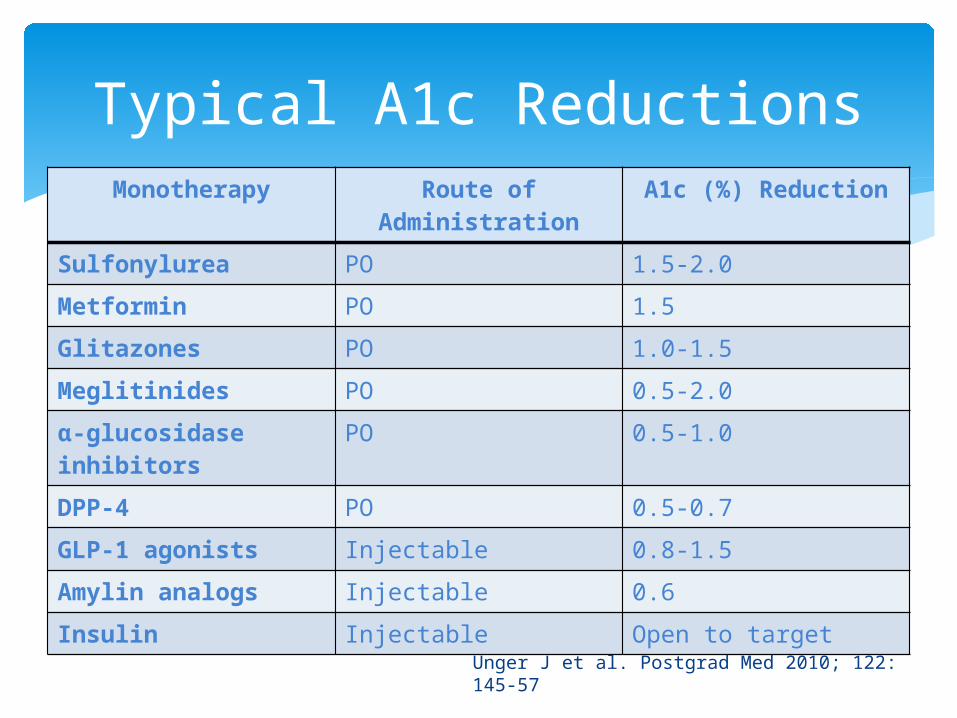
Typical A1c ReductionsMonotherapy Route of
AdministrationA1c (%) Reduction
Sulfonylurea PO 1.5-2.0
Metformin PO 1.5
Glitazones PO 1.0-1.5
Meglitinides PO 0.5-2.0
α-glucosidase inhibitors
PO 0.5-1.0
DPP-4 PO 0.5-0.7
GLP-1 agonists Injectable 0.8-1.5
Amylin analogs Injectable 0.6
Insulin Injectable Open to target
Unger J et al. Postgrad Med 2010; 122: 145-57
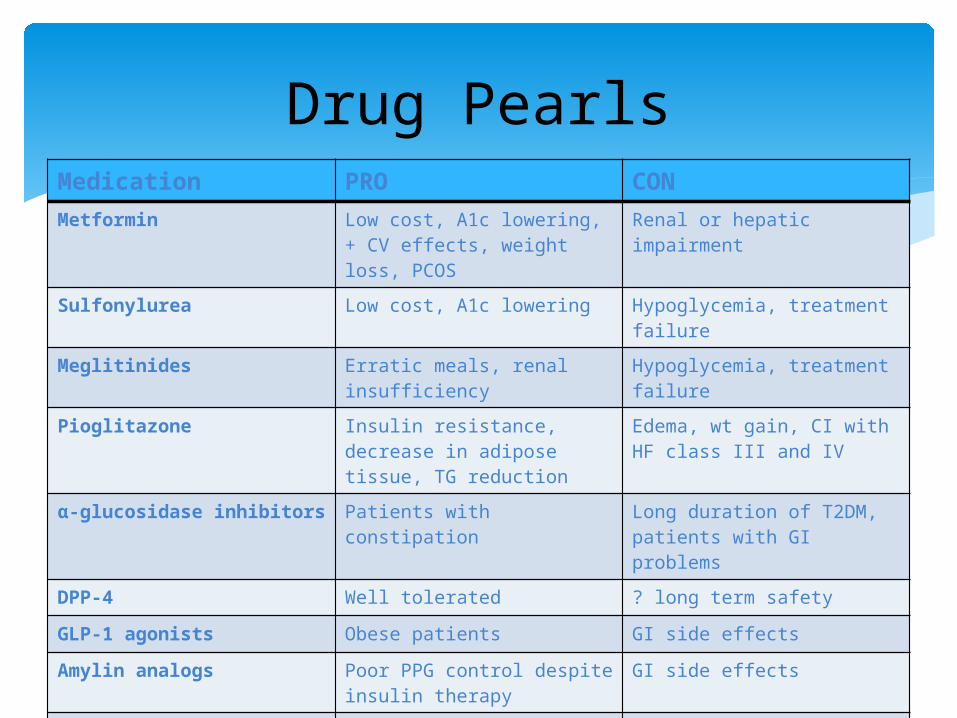
Drug PearlsMedication PRO CONMetformin Low cost, A1c lowering, +
CV effects, weight loss, PCOS
Renal or hepatic impairment
Sulfonylurea Low cost, A1c lowering Hypoglycemia, treatment failure
Meglitinides Erratic meals, renal insufficiency
Hypoglycemia, treatment failure
Pioglitazone Insulin resistance, decrease in adipose tissue, TG reduction
Edema, wt gain, CI with HF class III and IV
α-glucosidase inhibitors Patients with constipation Long duration of T2DM, patients with GI problems
DPP-4 Well tolerated ? long term safety
GLP-1 agonists Obese patients GI side effects
Amylin analogs Poor PPG control despite insulin therapy
GI side effects
Insulin Flexible treatment (basal, basal bolus, etc)
Hypoglycemia, weight gain
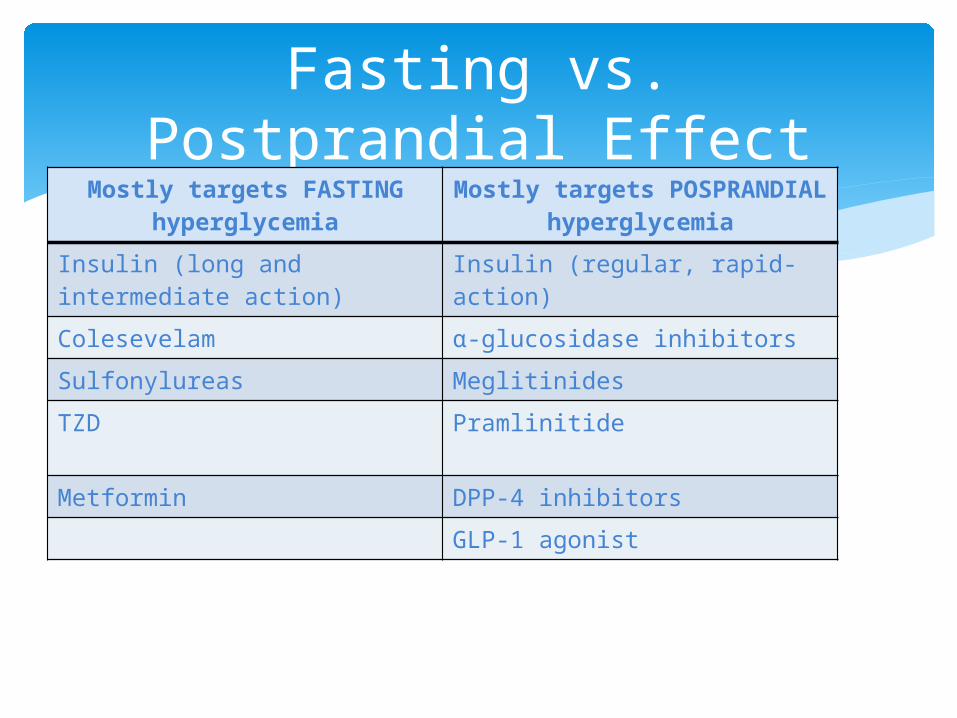
Fasting vs. Postprandial Effect
Mostly targets FASTING hyperglycemia
Mostly targets POSPRANDIAL hyperglycemia
Insulin (long and intermediate action)
Insulin (regular, rapid-action)
Colesevelam α-glucosidase inhibitors
Sulfonylureas Meglitinides
TZD Pramlinitide
Metformin DPP-4 inhibitors
GLP-1 agonist
Considerations When Selecting Therapy
How long has the patient had diabetes (duration of disease – preservation of β-cell function)?
Which blood glucose level is not at target (fasting, postprandial, or both)?
Patient preference for route of administration (oral, injection)?
The degree of A1c lowering effect required to achieve goal?
Side effect profile and the patients tolerability? Co – existing conditions ( CVD, osteoporosis, obesity,
etc)?
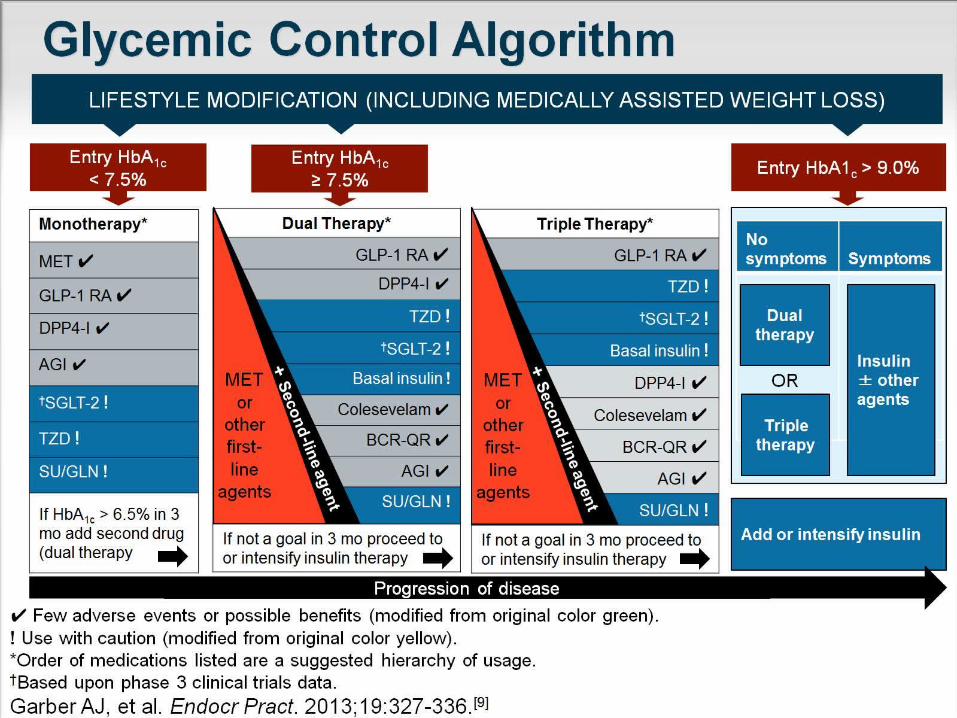
Glycemic Control Algorithm
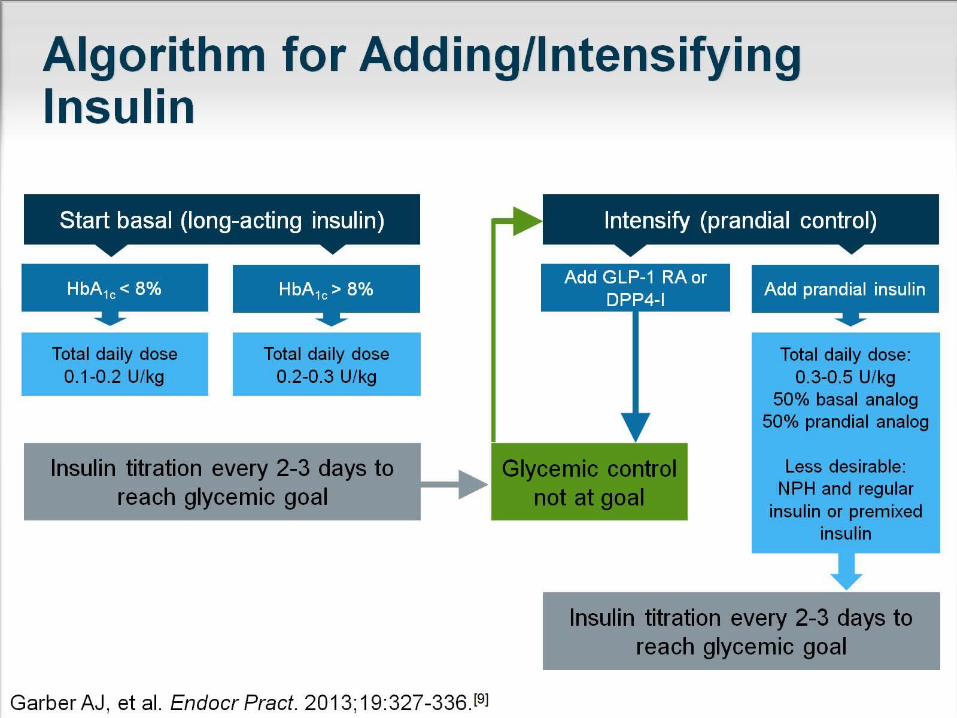
Algorithm for Adding/Intensifying Insulin

QUESTIONS
Top Related