







Languages
Pages
Legal


• Only 5-15% of blood cultures are (+) in febrile patients
A. Types of bacteremia: Extravascular via the lymphatic's Intravascular: i.e. CVC infections
B. Types of bacteremia: Transient: Disruption of mucosal surfaces (dental
or surgical procedures) Intermittent: Associated with abscesses Continuous: Infective endocarditis
Bacteremia: Pathogens
• S. Aureus
• S. Pyogenes
• S. Pneumoniae
• H. Influenzae
• Enterobacteriaceae
• Bacteroides
• Pseudomonas Aeruginosa
• Candida species

Occurrence of False Positive Blood Cultures (Trash)
True(%) Trash(%)
S. aureus876
Coag negative staph1282
Enterococcus7016
Diphtheroids296
C. perfringens2377
C. albicans90
Blood Cultures: Methods
• Two blood cultures for separate venipuncture sites is adequate
• Three sets of blood.
• At least 10ml/ venipuncture.• Blood culture > 5ml blood: 92% yield• Blood culture < 5 ml blood: 69% yieldDiagnostic yield increased by 3% for every 1 ml
of blood drawn
Blood Cultures: Interpretation
• Organisms isolated > 72 hours are often contaminants.
• A single blood cultures with coagulase (-) staphylococci is often a contaminant.
• A single (+) blood cultures with S. Aureus, gm (-) bacillie or candida is always a pathogen and requires therapy.
• The patient does not have leukocytosis or a left shift
Bacteremia: Contaminants
• Coagulase (-) Staphylococci.• Corynebacterium species• Bacillus species• If multiple isolated from separate sites are
obtained, the organisms could be pathogenic• Viridans Streptococci can be a contaminant

Aim of the test
• Diagnosis of bacteremia byAerobic and anaerobic cultivation of the blood, With identification and Susceptibility test of the isolated organism (s).
• Pediatrics: only aerobic.
• Blood culture should be made for cases with :
• suspected septicemia, endocarditis, and bacteremia secondary to localized infections (pneumonia, intraabdominal abscesses,
pyelonephritis, epiglottitis, meningitis).

Aerobic/Anaerobic Blood Culture Bottles
Criteria of specimen rejection
• Blood collected in tubes or bottles other than aerobic and anaerobic blood culture bottles.
• If the information on the label does not match that of the request form.
• Specimens for anaerobic blood culture received in aerobic bottles or vice versa.
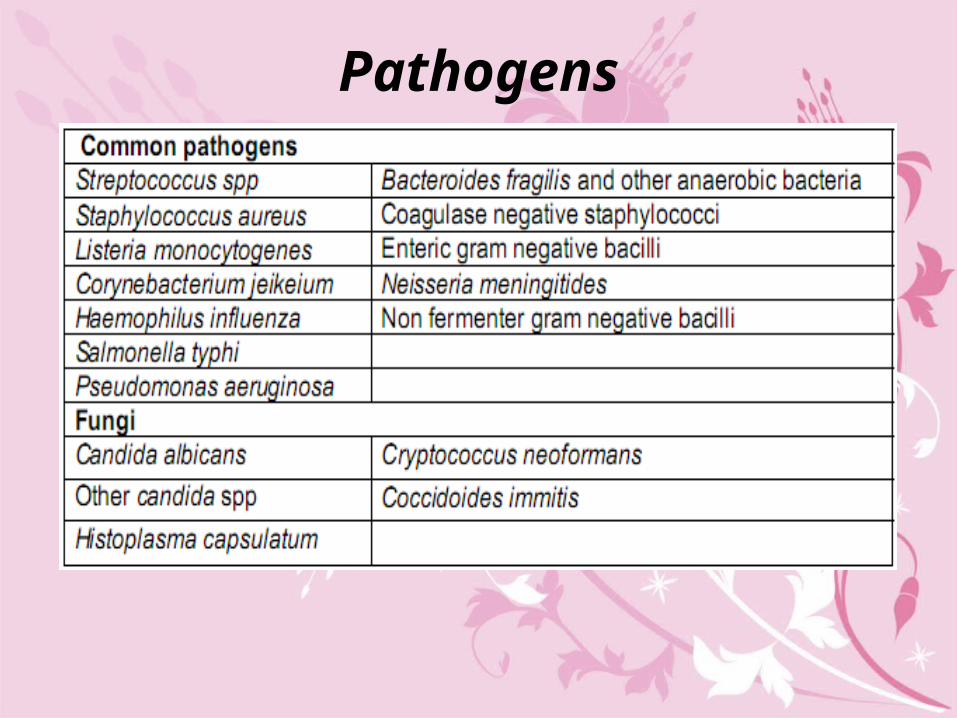
Pathogens
Patient preparing • The major difficulty in interpretation of blood cultures
is potential contamination by skin microbiota.
• So: careful attention to the details of skin preparation and antisepsis prior to collection of the specimen.

Obtaining Blood Culture
• Locate the vein (usually anticubital fossa)
• Attention to IV line.
• Prep kit
• Alcohol 5 sec. Dry 30-60 sec
• Tincture of Iodine-center to periphery. Dry 45-60 sec
• Remove caps, clean with alcohol
• Put on gloves
• Without palpating, draw 20 ml and put 10 in anaerobic and 10 in aerobic bottle.
• Dispose of syringe in sharps container.
• Label bottles and send to lab.

Set 1 = L. antecubital fossa at 0 minutes
Set 2 = R. antecubital fossa at 30 minutes
Set 3 = L. or R. antecubital fossa at 90 minutes.
Best time for sample collection: during fever spike\chills.
1st sample: 90% detection.

Quantity of specimen
Method
• Blood is injected to both aerobic and anaerobic bottles and incubated for up to 10 days at 37 C.
• Discard as negative after the 10 days• During the incubation period, a gram stain and
subculture onto appropriate media should be done.

Interpretation of Positive Blood Cultures
• Virtually any organism, including normal microbiota, can cause bacteremia.
• A negative culture result does not necessarily rule out bacteremia; • false-negative results occur when pathogens fail to
grow.
• A positive culture result does not necessarily indicate bacteremia; • false-positive results occur when contaminants grow.

• Gram-negative bacilli, anaerobes, and fungi should be considered
• pathogens until proven otherwise.
• The most difficult interpretation problem is to determine whether an organism that is usually considered normal skin microbiota is a true pathogen.

Top Related